 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Reproductive Medicine Vol. 8, No. 1, Winter, 2010, pp. 24-28 Incidence of gestational diabetes mellitus in pregnant women Sedigheh Soheilykhah1 M.D. Mahdie Mogibian2 M.D., Sodabeh Rahimi-Saghand1 M.D., Maryam Rashidi1 M.D., Saeideh Soheilykhah1 M.D., Maryam Piroz1 M.D.
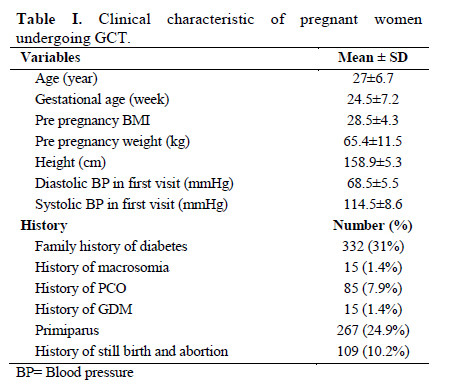
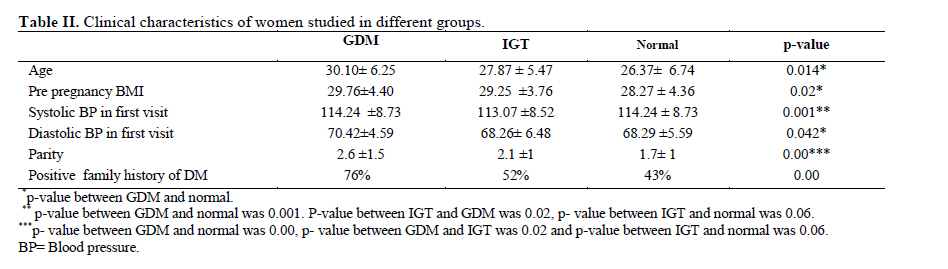
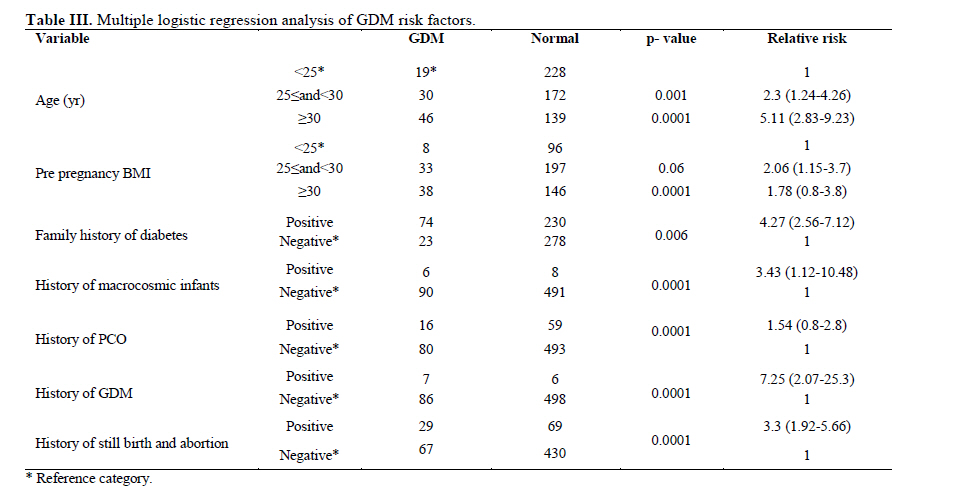
Corresponding Author: Sedigheh Soheilykha, Yazd Diabetes Research Center, Jomhoori Blvd., Afshar street, Yazd, Iran. E-mail: s_soheilykhah@yahoo.com Received: 28 September 2009; accepted: 10 January 2010 Code Number: rm10004 Abstract Background: Gestational Diabetes Mellitus (GDM) is the most common metabolic complications of pregnancy, and causes fetal mortality and morbidity. Therefore, early diagnosis of GDM is necessary to reduce maternal and fetal morbidity and to help prevent or delay the onset of type 2 diabetes Key words: Gestational diabetes mellitus, Glucose Challenge Test, Oral Glucose Tolerance Test. Introduction Gestational diabetes mellitus (GDM) is a state of glucose intolerance with the onset or first recognition occurring during pregnancy (1, 2). It shows the most common metabolic complications of pregnancy, and fetal mortality and morbidity (1).Therefore, early diagnosis of GDM is necessary to reduce maternal and fetal morbidity and to help to prevent or delay the onset of type 2 diabetes (3). GDM causes significant and often potentially maternal and fetal complications including preeclampsia, polyhydramnios, fetal macrosomia, birth trauma, perative delivery, neonatal metabolic complications and perinatal death. Development of obesity and diabetes in offspring during childhood and later development of diabetes mellitus in the mother are also related with GDM. Therefore, accurate screening and early diagnosis of this condition is very important to allow timely intervention in order to make certain a satisfactory pregnancy outcome (4). The GDM incidence, as reported in different studies, varies between 1% and 14% (5), and it is estimated that 90% of all pregnancies associated with diabetes are due to GDM. The differences in the incidence of GDM reported in studies are related to different ethnic and racial characteristics as the screening protocols and diagnostic criteria used by the researchers in question. Therefore, the present study was conducted to determine the incidence and risk factors of GDM in our population. Material and methods A cohort study on 1071 Iranian pregnant women was performed from 2007 to 2009. This study was approved by the Shahid Sadoughi University of Medical Science Ethical Committees. The participants were recruited from two prenatal clinics in Yazd, after obtaining informed consent for the scientific use of the data. Women with diabetes before pregnancy were not included in the study. From their medical records, information was obtained including maternal age, parity, gestational age, height, pre-pregnancy weight, systolic and diastolic blood pressure at the first prenatal visit, and reproductive and medical histories which were entered in analysis of the data as covariates. BMI was calculated by dividing the weight before pregnancy in kilograms by the height in meters squared. For all pregnant women universal screening with a 50 g oral glucose challenge test (OGCT) was done between 24-28 weeks of gestation. But, when risk factors such as positive family history of diabetes, age more than 30 years, obesity (BMI >30 kg/m2), previous history of GDM, and history of macrosomia were present; OGCT was done at the 14th and18th week of gestation. In the latter group, when the GCT result was negative (GCT ≤130), another GCT was performed at 24–28th weeks of gestation. Women, who have one abnormal OGTT value on the 3-hours OGTT, retest on 32 weeks of gestation by 100g OGTT. The study protocol was according to the recommendations for universal screening by the Fifth International Workshop Conference on Gestational Diabetes (1). One hour blood Glucose value ≤130 mg/dl was used as the cut-off value of the screening test irrespective of pregnancy age. Each participant was interviewed and maternal age, gestational age, reproductive and medical histories, history of fetal macrosomia (birth weight >4000g), outcome of previous pregnancy, and family history of diabetes, history of poly cystic ovarian syndrome (PCO), and history of cesarean section were considered. In all subjects, weight and height were measured on the screening day, while pre-pregnancy weight was asked from each woman. The gestational age was estimated by last menstrual period, confirmed or corrected by ultrasonography. At first all the participants were screened for GDM using an initial screening by measuring the serum glucose concentration 1h after a 50g OGCT. Then a diagnostic OGTT was performed on that subset of women exceeding the glucose threshold value on the GCT (130 mg/dl). In all women with positive GCT a 3-h OGTT with 100-g glucose was performed. The results interpreted according to the Carpenter and Coustan criteria (5) for GDM. The OGTT was performed after an overnight fast of 8 to 14 h while subject was on an unrestricted diet and unlimited physical activity for at least 3 days. Two or more of the venous plasma concentrations must be met or exceeded for a positive diagnosis (normal values: 0 h <95 mg/dl, 1 h<180 mg/dl, 2 h <155 mg/dl and 3 h <140 mg/dl). Women with one abnormal OGTT were classified in the impaired glucose tolerance (IGT) group (1). Women who did not have GDM were followed up monthly until delivery. Statistical analysis The incidence of GDM was calculated in all pregnant women. Data were presented as a percentage or mean ± SD. The t-test was carried out to test the difference between two groups. To assess the independent effect of each individual risk factor attributed to GDM multiple logistic regression were applied. Relative risk with a 95% confidence interval (CI) was calculated. Results During the study period, GCT was performed on a total 1071 pregnant women. Mean age of these women was 27±6.7 years and mean of gestational age was 24.5±7.2 weeks. A positive history of diabetes in first degree relatives was 31%. Mean of pre pregnancy BMI was 28.5 ± 4.3. Table I shows clinical characteristics of women. Incidence of GDM and IGT were 10.2% and 7.1% respectively. Among the 1071 studied pregnant women, 125 (11.5%) did not complete GTT and 10.6% of subjects with positive GCT had normal OGTT. From the remaining subjects, 110 cases of GDM diagnosed. GCT was performed early in pregnancy (less than 28 week of gestation) in 247 women, while in 251 women it was performed later than the 28th week of gestation and in 573 women between the 24-28 weeks. The mean time of GCT was 24.34±7.02 week. GCT was positive in 95 pregnant women in less than 24 week of gestation and in 155 subjects in 24-28 week and in 92 subjects more than 28 week. Analysis on the gestational weeks of the total 110 GDM women showed that 37 subjects (33.6%) were within less than 24 weeks of gestation, 42 (38.1%) were between 24 and 28 week and 31 (28.2%) were more than 28 weeks of gestation. A group of women (n=48) at low risk according to the ADA recommendation (5) was identified. In this group, women one met the criteria for GDM (2.1%), two had IGT (4.2%) and 4 had impaired GCT with normal OGTT (8.4%). In table II clinical characteristics of pregnant women in different groups (GDM, IGTT, normal) are shown. When we compared GDM group with normal and IGTT, pregnant women who had GDM were older, more parous and more obese. This study also showed that systolic and diastolic blood pressure in diabetic patients was higher than normal group. GDM was more prevalent in women with a positive history of diabetes (76.3% vs. 23.7%, p=0.0001); with older age ( <25 years 20%, 25-29 years 31.6% and ≥30 years 48.4%, p=0.0001); with pre pregnancy BMI (<25 kg/m2 10.1%, 25-29.9 kg/m2 41.7% and ≥30 kg/m2 48.1%, p=0.01); and with history of macrosomic infant (Positive 93.8% vs. Negative 6.3%, p=0.05).To establish the independence of these variables a multivariate analysis was performed by using a multiple logistic regression model (Table III). Relative risk of history of GDM, positive family history of diabetes, history of macrocosmic infant and history of still birth and abortion were 7.25, 4.27, 3.43 and 3.3 respectively. Discussion GDM has been recognized for decades, but controversies remain regarding the screening test and diagnostic criteria. There is general consensus that incidence of GDM is increasing globally. The incidence of GDM in the current study was 10.2% within the reported range in literature (6), but was higher than in other studies in Iran (7). This difference may be related to the screening methods, diagnostic criteria used or population studied. Another reason for this difference might be high prevalence of type 2 diabetes in Yazd (8). Data from previous studies show that the incidence of GDM in Iran is between 4.8-7.4% (7, 9, 10). We have estimated incidence of GDM in pregnant women at low risk for GDM according to ADA recommendation (5). Our results showed if we did not screen low risk pregnant women for GDM we would have missed one woman with GDM. In agreement with other studies (11-14), this group included few women with a low risk of GDM, resulting in a very low incidence. This would provide evidence for an acceptable performance of the selective screening, because it would miss no more than 2.1% of GDM in a low risk population. In the present population, about 97.2% were at medium/high risk for GDM, showing an acceptable indication for screening. Family history of diabetes has a strong correlation with occurrence of GDM. Our study reported a positive family history of diabetes in 76% of women with GDM compared with 43% in normal group. This result compared with the study of Hadaegh et al and Jawad et al (15, 16). Incidence of GDM is also affected by previous pregnancy outcome. Naylor et al found glucose intolerance in 14.5% of women who had adverse obstetric outcomes (17). In our study the incidence in GDM increased in women who had previous abortion, still birth, history of macrosomia and previous history of GDM. Pre pregnancy BMI was considered to be a predictor development of GDM (18). The other studies also showed GDM tend to occur more frequently in women with BMI more than 25 (15-18). This is in agreement with results of our study. Our results indicated the number of parity in GDM was higher than normal group. It was inline with Hadaegh et al (15). It may be due to this fact that increasing parity is associated with other diabetic risk factors like increasing age, body weight and fat deposit. Some studies showed incidence of GDM in pregnant women with PCO was higher than normal group (19). Similarly in our study the risk of GDM was 1.54 in women with PCO. However, we defined PCO according to history of irregular menstruation and/or hirsutism before pregnancy and it was not an accurate diagnostic tool for PCO (20). We did not have ultrasound finding about PCO before pregnancy. In our study there was no significant association between height and GDM. Unlike the other studies which reported that GDM tends to occur more frequently in women who are short (21-23). After logistic regression analysis, GDM was significantly correlated with age, pre pregnancy BMI, family history of diabetes, history of PCO, history of GDM and previous adverse outcome of pregnancy. These results are in concordance with other studies (15-18). Our finding showed universal screening remains a good method to identify women with GDM at least in populations like our area with a large percentage of women at medium/high risk for GDM. In conclusion this study emphasized the need for GDM screening in Iranian population, because the number of medium/high risk population for GDM was high and should be assessed after proper risk stratifications. A significant higher incidence of GDM was found in women who are aged, multiparus, have high pre pregnancy BMI, and previous history of GDM or adverse outcome of pregnancy. Acknowledgment This study was supported by Yazd Diabetes Research Center of Shahid Sadoughi University of Medical Sciences. The authors wish to thank all the colleagues who supported the research, and Yazd Blood Transfusion Center staff for assistance with sampling. References
© Copyright 2010 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm10004t1.jpg] [rm10004t3.jpg] [rm10004t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}