 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
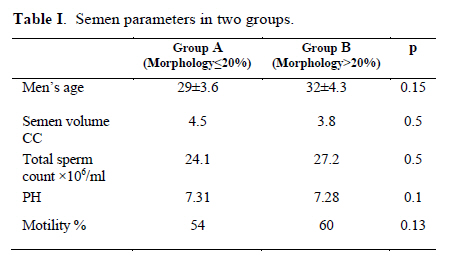
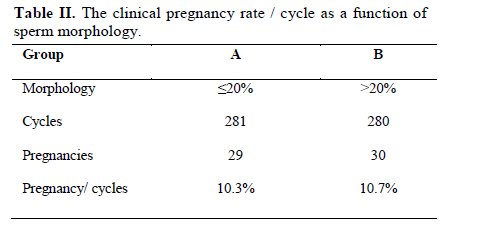
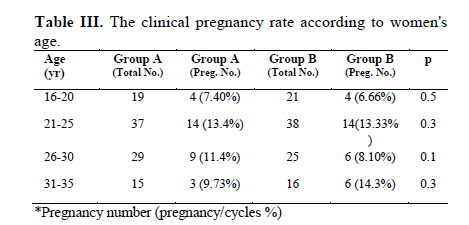
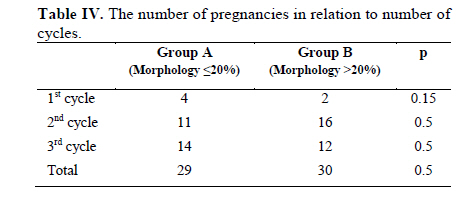
Iranian Journal of Reproductive Medicine Vol. 8, No. 1, Winter, 2010, pp. 41-44 The effect of sperm morphology on IUI outcome in cases with unexplained and male factor infertility Shahdokht Motazedian M.D., Bahareh Hamedi M.D., Jaleh Zolghadri M.D., Khatereh Mojtahedi M.D., Nasrin Asadi M.D. Division of Infertility, Department of Obstetrics and Gynecology, Shiraz University of Medical Sciences, Shiraz, Iran. Received: 17Jun 2009; accepted: 9 December 2009 Corresponding Author: Shahdokht Motazedian, Professor of Obstetrics and Gynecology, Infertility and Gyn Endoscopy Specialist, Shiraz University of Medical Sciences, Shiraz, Iran. E-mail: sh.motazedian@yahoo.com Code Number: rm10007 Abstract Background: Although intrauterine insemination (IUI) is one of the most common methods which is used for male factor and unexplained infertility, the relative influence of various semen parameters on the likelihood of a successful outcome is controversial. Several semen parameters have been evaluated as predictors of a successful outcome with intrauterine insemination. Key words: Male infertility, Unexplained infertility, Sperm morphology. Introduction Intrauterine insemination (IUI) recognized to be an effective and inexpensive method managing the patients with unexplained and male factor infertility.It is generally attempted before proceeding to more invasive assisted reproductive techniques such as in vitro fertilization (IVF) and intracytoplasmic sperm injection (ICSI). IUI is a widely utilized method for treating distinct types of infertility such as unexplained infertility, endometriosis, male infertility, anovulation and cervical antisperm antibody (1, 2). Predictive sperm parameters for successful IUI have been controversial (1, 3-5). Several semen parameters have been shown to correlate with IUI outcome such as number of motile sperm and normal morphology (3). Although WHO reference values for semen analysis are often used to assess sperm quality, more often unsuccessful pregnancies with IUI have been achieved in subfertile couples with sperm parameters below WHO reference values. The minimal recommended number of normal sperm morphology inseminated varies from 30% (by WHO reference value) to 4% depending on some studies (1, 2, 6-10). The aim of our study was to assess the likelihood of IUI outcomes based on sperm morphology in the case of unexplained and male factor infertility and to help clinicians predict IUI outcomes. Materials and methods This study was a prospective descriptive between Jan 2007-Nov 2008 in 200 patients with unexplained infertility (primary or secondary) and male factor infertility (low sperm morphology) in Department of Infertility in Zeinabieh Hospital. Diagnostic workups for female patients included physical examination, hormonal assay; hyterosalpingography, base line sonography and laparoscopy within normal limits. Patients were chosen in to 2 groups, group A: 100 patients with normal semen parameters such as motility and count but low morphology of ≤20% before wash and group B: 100 patients with morphology >20% before wash and unexplained infertility. Normal sperm values were determined by the most recent WHO criteria of semen analysis (8). Other sperm parameters were as table 1 with no significant differences between the two groups. Both groups underwent induction of ovulation by clomiphene citrate (CC, Razi, Iran) with dose of 100mg from 5th - 9th days of menstrual cycle. Vaginal sonography was done on 14th or 15th day of cycle. If the response to medication was satisfactory (≥3 follicles with the size of 16-18mm), HCG (Charwoman, IBSA, 10,000U) was injected intramuscularly. IUI was done 24-30 hrs after HCG injection for 3 cycles. Immediately before performing IUI, removal of any excess cervical mucus was done and tip of the insemination catheter (Wallace, Wallace, USA) was inserted in to the cervical OS and then slowly into the uterine cavity and washed semen was injected. If no pregnancy was occurred with clomiphene after 3 cycles, human menopausal gonadotropin (HMG, Merional, IBSA) was added from 8th day of next cycle. After satisfactory sonographic results (as mentioned above), HCG was injected and IUI was done 24-36 hrs after that (11). Statistical analysis A global X2 - test was calculated to determine whether there was a statistically significant difference between the 2 groups (using SPSS software, version 15). P-value<0.05 was considered significant. Results The mean age of the women was 23.7±4.7 years in group A and 26.5±4.1 in group B. The mean age of men and semen parameters was as table I. The indications for IUI were: unexplained infertility (n=100) and male factor infertility (n=100). There were 561 IUI cycles among 200 patients for which all data were available on age, sperm morphology (before wash) and pregnancy rate / cycle. Patients underwent 2 forms of controlled ovarian hyperstimulation (clomiphene citrate + HCG, or clomiphene citrate + HMG+ HCG). Fifty nine clinical pregnancies followed 561 IUI cycles for a clinical pregnancy rate/ cycle of 10.5%. Pregnancies occurred in 29 patients of 281 cycles in group A and 30 patients of 280 cycles in group B. Table II shows the clinical pregnancy rate / cycle as a function of the sperm morphology. In pregnancies of group A: 21 live birth, 6 spontaneous abortions and 2 ongoing pregnancies were detected. In group B: 19 live birth, 8 spontaneous abortions and 3 ongoing pregnancies occurred. There were no statistical differences between 2 groups in pregnancy outcome. Looking at the clinical pregnancy rate according to women's age (Table III) shows no significant differences in pregnancy /cycle in relation to age. Also numbers of pregnancies in relation to numbers of cycles show no statistically significant differences between the 2 groups (Table IV). Discussion Intrauterine insemination using the husband's sperm is commonly performed to overcome male factor problems as well as to enhance the probability of conception in various other causes of infertility. This study sought to evaluate the effect of sperm morphology (before preparation), on intrauterine insemination related pregnancy. In our study, 59 clinical pregnancies were achieved after 560 IUI cycles, for a total clinical pregnancy rate / cycle of 10.5%. This rate is within the range of previous reports (1, 3, 12). In a study done by Badawy et al 393 couples underwent 714 IUI cycles for a pregnancy rate / cycle of 11.6% (9). Also, Wainer et al showed a total clinical pregnancy rate/ cycle of 12.9% among 2564 IUI cycles in couples with male factor infertility (1). As in most forms of infertility treatment, the success of IUI is largely influenced by the etiology of the infertility and the sperm quality (1, 2, 6-10). Unfortunately, the majority of studies attempting to find which sperm characteristics correlated better with cycle outcome included multiple female infertility problems as well. Therefore, the results might be biased by the other infertility etiologies that were treated in parallel (3). The prognosis for success with IUI in the treatment of male infertility is best when there is no other coexistent infertility (11, 13). Pregnancy rate after IUI has been evaluated according to indication, age and semen parameters (such as motility, morphology and volume) in some studies (1, 3, 9, 13-16). Most specifically, the prognosis is greatly influenced by the age of the female partner and the consistency and quality of her ovulatory function (11, 14).Sperm morphology reflects the quality of spermatogenesis. Morphologic abnormalities (teratospermia) are categorized by location, involving the head, neck (midpiece), or tail (11). Strict sperm morphology represents the best current predictor of sperm function (the capacity to fertilize a mature oocyte). The most recent WHO criteria (1999) for the evaluation of sperm morphology are very similar to those known as the Kruger (Tygergerg) criteria (17-19). In our study, only the morphology of semen characteristics was recruited to make the differences in pregnancy rate. We divided the patients into two groups on sperm morphology: (A: ≤20% normal morphology and B: ≥20% normal morphology). We evaluated the effect of sperm morphology on the success rate of IUI. Our results had not shown any significant statistically difference between rate of pregnancy and success of IUI in both groups. Also, we did not show any significant difference in pregnancy/cycle in relation to age (maybe due to small volume of specimen). Also, in some other studies, the effect of sperm morphology has been evaluated on the success rate of IUI, but published reports have been controversial in this regard (1, 3). On the other hand, patient’s normal sperm forms less than 20% according to WHO criteria have no benefit in the IUI (4). As the same, some authors concluded, that IUI used for treating male factor infertility has little chance of success when normal sperm morphology is < 30% (3). Other authors suggested that when the normal morphology of the sperm after preparation is < 30%, higher number of motile spermatozoa (a minimum of 5 ×106 ) should be inseminated for effectiveness of IUI (1). However, it has been concluded in other studies, which success rates with IUI are high when 14% or more of the sperm have normal morphology, intermediate with values between 4% and 14% , and generally quite poor when fewer than 4% of sperms are normal (5). Reviewing medical literature some studies reported a very low pregnancy rate (1%per cycle) when the sperm morphology score was < 4% (20), whereas in other studies were reported comparable pregnancy rate per cycle reported between the two groups (14, 21). It seems that in cases with very low sperm morphology in semen analysis (<5%), in vitro fertilization and intracytoplasmic sperm injection may enhance the chances of success (11). Although some have suggested that two inseminations (12 and 34 hours after hCG-induced ovulation) yield higher cycle fecundability than a single IUI, other similarly designed studies have found no such advantage. Most women who pursue therapeutic insemination are otherwise fertile and conceive within 4-6 insemination cycles; cycle fecundability declines by half to two-thirds thereafter (22, 23). We believed that management must be individualized to the specific needs of a couple and a multitude of factors should be considered to optimize the chance of pregnancy. In this study, we evaluated the sperm morphology and the success rate of IUI. We showed no differences in the success rate of IUI in patients with male factor infertility (normal semen analysis except for morphology≤ 20%) and normal sperm morphology (> 20%). References
© Copyright 2010 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm10007t4.jpg] [rm10007t1.jpg] [rm10007t2.jpg] [rm10007t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}