 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Reproductive Medicine Vol. 8, No. 2, Spring, 2010, pp. 86-89 Short communication Frequency of poly cystic ovary syndrome in patients with premenopausal breast cancer Nasrin Ghasemi1 M.D., Ph.D., Mohammad Reza Mortazavizadeh2 M.D., Aboolfazl Khorasani Gerdekoohi3 M.D. 1Department of Medical Genetics, Research and Clinical Centre for
Infertility, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
Corresponding Author: Nasrin Ghasemi, Department of Genetics, Research and Clinical Centre for Infertility, Shahid Sadoughi University of Medical Sciences, Yazd, Iran. Email: n479g@ssu.ac.ir Received: 4 August 2009; accepted: 3 February 2010 Code Number: rm10016 Abstract Background: Polycystic ovary syndrome (PCOS) is a heterogeneous, complex
genetic disorder characterized by hyperandrogenemia, hyperinsulinemia, insulin
resistance,
and chronic anovulation. It is the most common endocrine disorder in women
of reproductive age with an enigmatic pathophysiologic and molecular basis.
Obesity, hyperandrogenism, and infertility occur frequently in PCOS, which
mostly have a genetic predisposition, and are features known to be associated
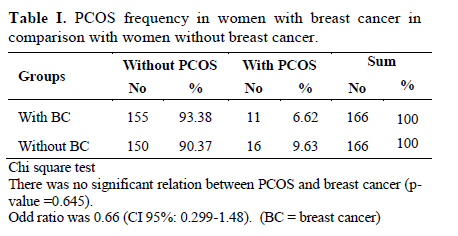
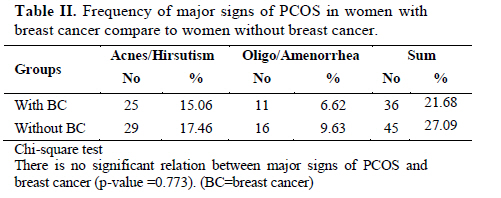
with the development of breast cancer risk. Key words: Polycystic ovary syndrome, Premenopausal breast cancer, Endocrine disorder. Introduction Polycystic ovary syndrome (PCOS) was seen in 15% of women at reproductive age (1). It is one of the most important endocrine problems in reproduction, which in it chronic anovulation and hyperandrogenism happens (2). The risk of a number of gynecological neoplasias, including endometrial , breast , and ovarian cancer increase in women with PCOS (3). Obesity, hyperandrogenism, and infertility occur frequently in PCOS, and are features known to be associated with the development of breast cancer. However, studies examining the relationship between PCOS and breast carcinoma have not always identified a significantly increased risk (4). The endocrine abnormalities in PCOS including prolonged exposure to estrogen, progesterone deficiency, and androgen excess, could contribute to an increased risk for gynecological cancers. Previous studies have revealed that the etiology of breast cancer is linked to long exposure of breast epithelium to estrogens, especially in conjunction with progesterone (5). Long reproductive period (early age at menarche and/or late age at menopause) represents risk factors for this malignancy (6). As for the effect of pregnancy on breast cancer risk, there is a transient increase risk in the first 3–4 years after delivery of a baby, but lifetime risk seems lower than that of women who remain nulliparous (5). The elevated androgen levels and the increased levels of insulin and IGF-I detected in PCOS and obesity could enhance the development of breast cancer. PCOS usually accompanies with obesity, which have elevated androgen levels and increased levels of insulin and IGF-I. These conditions could enhance the development of breast cancer, which could happens to direct stimulation of AR-positive cancer cell in binding with androgen; stimulation of ER-positive cells by intratissular changes of testosterone to estradiol, mitogenic stimulation of cancer cells by insulin and IGF-I; and decreased levels of SHBG and increased levels of free estrogens in hyperandrogenic women (7-8). Because of the etiologic implications of the previously reported positive association between polycystic ovaries and breast cancer (9-11), present study attempted to confirm the relation. The study used data from a case-control study that compare frequency of PCOS among breast cancer patients with healthy controls. Materials and methods To investigate the relation between polycystic ovaries and breast cancer, frequency of PCOS was evaluated between 166 patients with breast cancer. Cases included premenopausal women with histologically confirmed primary breast cancer. This frequency was compared with frequency of PCOS among 166 women without breast cancer, which was confirmed by mammography in last six months. The age of cases and controls was matched. All cases and controls were fertile and the frequency of the use of contraceptive pill in both groups was not significantly different. PCOS patients in women with breast cancer and healthy controls were detected by face to face interview and filling the questionnaire, then it was confirmed by sonography in both groups. Cases and controls filled the informed consent form to be part of this study. The number of cases and controls were calculated according to approximately 10% prevalence of PCOS in population. The 2003 Rotterdam consensus workshop was used to diagnose PCOS, which is a syndrome of ovarian dysfunction along with the cardinal features hyperandrogenism and polycystic ovary PCO. The results were analyzed by SPSS software (version 15) using chi-square test and odd ratio with CI. Statistical analysis The frequency of PCOS in women with breast cancer compare with healthy controls using chi-square test. Results Frequency of PCOS in 166 women with breast cancer was compared with normal controls. The mean age of the cases was 44.3 ± 3.80 (31 to 51 years old) and in controls was 44.2 ± 3.84 (30 to 50 years old). In this study, the frequency of PCOS in breast cancer patients was 6.62% compare to 9.63% in control group. The risk of breast cancer was lower among women with history of physician-diagnosed polycystic ovaries than women without such a history (Table I). The odd ratio was 0.66 (CI 95%: 0.299-1.48). Current data show that of women with breast cancer, 15.1% have hyperanderogenism, 6.6% have anovulation, 1.8% have obesity, and 1.8% have infertility, which were not significantly different with control group. There was not a relation between the frequency of PCOS signs and breast cancer (Table II). Discussion Obesity, hyperandrogenism, and infertility are features of PCOS, which were known to be associated with the development of breast cancer. However, the epidemiological data in the literature about PCOS and breast cancer risk are contrasting (4, 12-17). The results of present study did not show increased risk of PCOS in breast cancer patients. In an English cohort study, women with PCOS had no significantly increased risk of mortality or morbidity from breast cancer (18). In a US cohort study on 34 835 women, of whom 833 developed a breast cancer during the follow-up, subjects with PCOS were not more likely to have a breast cancer, and adjustment for age at menarche, age at menopause, parity, oral contraceptive use, BMI, waist/hip ratio and family history of breast cancer lowered the RR to 1 (4). Recently, a pentanucleotide repeat [(TAAAA)n] polymorphism in the promoter region of the CYP11A gene, that encodes the cholesterol sidechain cleavage enzyme, has been found to be associated with the risk of PCOS (19-22). Zheng et al investigated the association of this polymorphism with breast cancer risk in a Chinese population-based case–control study including 1015 breast cancers and 1082 community controls (23). Therefore, a pentanucleotide repeat polymorphism in the CYP11A gene could represent a linkage between PCOS and breast carcinogenesis. Gammon and Thompson, 1991 reported a reduced risk of breast cancer in women with PCOS finding an odds ratio of 0.52 (95% CI 0.32-0.87), this study however is difficult to interpret as the prevalence of PCOS as identified by a self-assessed questionnaire (13). Conversely, the study of Atiomo et al detected a statistically significant positive family history of breast cancer among women with PCOS (16). In an English study designed to test whether cardiovascular mortality was increased in 786 women with PCOS followed for an average of 30 years, the standardized mortality ratio (SMR) for all causes was 0.90, based on 59 deaths, the SRM for circulatory disease was 0.83, based on 15 deaths, and the SRM for breast cancer was 1.48, based on 13 deaths (17). In conclusion, present study did not find significant relation between PCOS and risk of breast cancer. However, most of previous study suggested the relation between PCOS and risk of breast cancer in postmenopausal women by adjusting age. This statement could be confirmed by the other study for the frequency of the PCOS in postmenopausal women with breast cancer. The age of menarche, the age at the first pregnancy and the duration of breast feeding should be considered in future study. Acknowledgment The authors thank Dr. Afsaneh Ghasemi who did sonograghy for control group, and Yazd Shahid Sadoughi University of Medical Sciences for financial support of this medical student dissertation. References
© Copyright 2010 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm10016t2.jpg] [rm10016t1.jpg] |
| |||||||||

{kind=link}
{kind=link}