 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Reproductive Medicine Vol. 8, No. 2, Spring, 2010, pp. 90-93 Case report Hemoperitoneum during pregnancy with endometriosis; report of four cases Tae-Hee Kim1, 2 M.D., Hae-Hyeog Lee1 M.D. 1Department of Obstetrics and Gynecology, College of Medicine, Soonchunhyang
University, Bucheon, 420-767, Republic of Korea. Corresponding Author: Hae-Hyeog Lee, Department of Obstetrics and Gynecology, Soonchunhyang University, Bucheon Hospital 1174 Jung-1-dong, Wonmi-gu, Bucheon-si, Gyunggi-do, 420-767, Republic of Korea. Email: hhl22@chol.com, hhl22@schbc.ac.kr Received: 30 November 2009; accepted: 14 March 2010 Code Number: rm10017 Abstract Background: Endometriosis is a chronic inflammatory gynecologic disease.
Problems associated with endometriosis include dysmenorrhea, dyspareunia, and
infertility.
While endometriosis does not generally cause complications during pregnancy,
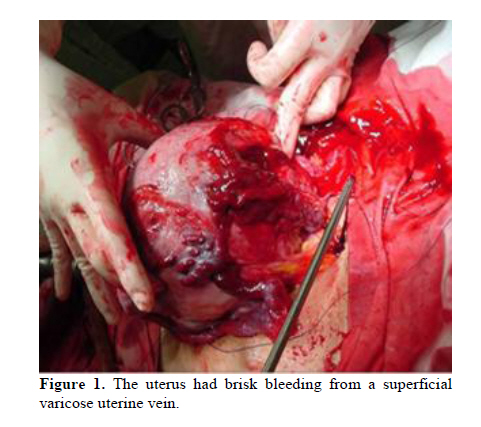
endometriosis clearly causes complications before pregnancy. Key words: Hemoperitoneum, Endometriosis, Pregnancy. Introduction The main complication of endometriosis is infertility. With the development of assisted reproduction technology (ART), it is possible that endometriosis patients with infertility secondary to an anatomic distortion of the ovaries and tubes have been able to conceive (1). A spontaneous hemoperitoneum during pregnancy is a rare and life-threatening condition. Previous reports have shown that the majority of hemoperitoneums during pregnancy occur before labor; most cases have involved uterine rupture. Most causes of obstetric hemoperitoneum are unknown (2). The purpose of this retrospective review was to evaluate the complications of pregnancies in women with chronic pelvic pain who had undergone laparoscopic resection of endometriosis. The appropriate management of a hemoperitoneum during pregnancy is discussed with a brief review of the literature. Case report Case 1 A 33 years old primigravida with a bichorial, biamniotic twin pregnancy presented to our hospital at 33 weeks gestation. The patient was known to have stage IV endometriosis which was diagnosed during laparoscopy performed as part of a fertility diagnosis. She became pregnant by in vitro fertilization (IVF) with embryo transfer (ET). She experienced a sudden increase in pain, nausea, vomiting, and dizziness. Prolonged fetal heart rate decelerations were recognized in baby A, along with frequent uterine contractions. The vital signs were unstable, the blood pressure was 90/70 mmHg, the pulse rate was 100 /min, and the hemoglobin was 6.5g/dL. An ultrasonography showed a large fluid collection in the right upper quadrant of the abdomen. The patient had abdominal guarding with severe rebound tenderness. Based upon these clinical findings, the provisional diagnosis was placenta abruption or panperitonitis. An emergency cesarean section was performed. At the time of the cesarean delivery, about 2 liter hemoperitoneum was present. The placenta appeared normal and complete, with no evidence of abruption. Two live infants were delivered (baby A was a male weighing 2,190 grams with Apgar scores of 3 and 7 at 1 and 5 minutes, respectively; baby B was a male weighing 2,300 grams with Apgar scores of 4 and 7 at 1 and 5 minutes, respectively). She was transfused 6 units of packed red blood cells and 3 units of fresh frozen plasma. Examination of the uterus revealed brisk bleeding from a superficial varicose uterine vein (Figure 1). The surface of the uterus appeared lacerated with multiple bleeding endometriotic lesions. Complete hemostasis was achieved with interrupted sutures and electrocauterization of the bleeding points. Case 2 A 28 years old primigravida presented to our department at 25 weeks gestation. After confirming preterm premature rupture of the membranes (PPROM) and fetal well-being, she was admitted to the hospital and received prophylactic antibiotics. During her stay in the hospital she complained of mild lower abdominal pain, nausea, epigastric pain, and vomiting. After 6 days, she experienced a sudden increase in pain and dizziness. There was no vaginal bleeding. The vital signs were stable, the blood pressure was 100/70 mmHg, the pulse rate was 80 /min, and the hemoglobin was 8.0 g/dL. The patient had abdominal guarding with rebound tenderness. Based upon these clinical findings, a provisional diagnosis of placental abruption or acute abdomen was made. An emergency cesarean section was performed. At the time of the cesarean section, a 1 L blood clot was noted in the cul-de-sac. The placenta appeared normal and was removed completely; there was no evidence of abruption. A live female infant weighing 720 grams was delivered and had Apgar scores of 5 and 7 at 1 and 5 minutes, respectively. The infant was admitted to the neonatal intensive care unit (NICU). The patient received 2 units of packed red blood cells. The posterior surface of the uterus appeared lacerated with multiple bleeding from endometriotic lesions. Rupture of a superficial varicose uterine vein was found. Complete hemostasis was accomplished with electrocauterization of the bleeding points. Case 3 A 37 years old gravida 2, para 1 with a single pregnancy at 40 weeks gestation presented to a local private obstetric clinic with cervical dilation > 5 cm. Labor progressed rapidly and culminated in the delivery of the fetus in < 1 hour. The patient was transferred to our hospital due to massive uterine bleeding. The patient’s medical history included endometriosis diagnosed during an operative laparoscopy before the current pregnancy in which lysis of adhesions and ablation of endometriotic lesions were performed. Lacerations of the vagina in the posterior fornix and cervix on the right side were noted on vaginal examination. After the lacerations of the vagina in the posterior fornix and cervix were repaired and emergency uterine artery embolization (UAE) was performed, a hemoperitoneum was found. When the abdomen was opened, fresh liquid and clotted blood was observed. There were two causes of the hemoperitoneum (rupture of a subserosal uterine vessel on the uterine fundus and rupture of a deep infiltrated endometriotic lesion located under dense adhesions in the cul-de-sac), resulting from strong pressure or stretching during the vaginal delivery. We performed a cesarean hysterectomy and achieved hemostasis with sutures. The initial laboratory studies revealed hemoglobin of 7.9 g/dL, a hematocrit of 23%, and coagulation parameters consistent with disseminated intravascular coagulopathy (DIC). A massive transfusion of blood products (22 units of packed red blood cells, 5 units of fresh frozen plasma, and 28 units of platelet concentrate) was required. Case 4 The case was 29 years old gravida 1, para 0 with a single pregnancy at 40+6 weeks gestation. Her previous medical history included endometriosis diagnosed during an operative laparoscopy. The current pregnancy was conceived after IVF treatment because of pelvic adhesions. When cervical dilation was complete, the baseline fetal heart rate was 70-80 beats/minute. An emergency cesarean hysterectomy was performed for uterine rupture at a local clinic. The mother and baby were transferred to our hospital for the purpose of bleeding control of operation site. She was hypotensive and tachycardic on arrival. Abdominal guarding with rebound tenderness was present. An emergency laparotomy was performed. When the abdomen was opened, a hemoperitoneum of several large clots and fresh blood in the cul-de-sac was noted. There was oozing and rupture in deep infiltrated endometriotric lesions located under dense adhesions in the cul-de-sac. Transfusion of blood products (6 units of packed red blood cell, 6 units of fresh frozen plasma, and 10 units of platelet concentrate) was required. Her 3,200 gram male infant was admitted to the neonatal intensive care unit (NICU) due to asphyxia, hypoxic brain damage, and cerebral ischemia. Discussion Endometriosis is an inflammatory disease that affects 10-15% of women of reproductive age (3). The main clinical features are chronic pelvic pain, dyspareuria, and subfertility. It is commonly believed that pregnancy reduces the symptoms in patients with endometriosis. The use of assisted reproduction technology (ART) for treating infertile couples is increasing in the United States and other countries (1). Women with endometriosis are more likely to have difficulties conceiving, but ART provides an increased chance of conceiving for infertile women with endometriosis and anatomic distortion of the ovaries and tubes. About 120 cases have been reported in the literature since 1778, most cases were reported before the 1980s (4). Between 2000 and 2009, epidemiologic studies or case reports suggest that women with endometriosis may have an increased risk for preterm birth (5). Women with endometriosis are more frequently affected by preeclampsia and antepartum hemorrhage (1). Urohemoperitoneum during pregnancy with fetal death in a patient with deep endometriosis is rare, but reported (6). We have found other reported cases in which endometriosis was associated with hemoperitoneum during pregnancy (7). Most cases had uterine vessel hemorrhage and histories of laparoscopic surgery for endometiosis (8-10). Three of our cases had moderate-to-severe endometriosis and had undergone laparoscopic lysis of adhesions. The presence of surgical scar tissue and deep infiltrated endometriotic lesions located under dense adhesions in the cul-de-sac could have been avulsed by uterine contractions and pushing in labor. Four cases had bleeding from superficial varicose uterine veins. It is commonly believed that pregnancy has good effects on endometriosis by reducing the symptoms, but we have to be aware of complications of endometriosis during pregnancy. During first trimester, endometriosis is associated with an increased risk of fetal loss that includes miscarriage and ectopic pregnancy. During the second and third trimesters, spontaneous hemoperitoneum from rupture of uterine or ovarian vessels is possible. During labor, a spontaneous hemoperitoneum from deep infiltrated endometriosis lesions located under dense adhesions in the cul-de-sac is possible. Dense adhesions in the cul-de-sac could be avulsed by strong pressure or stretching during vaginal delivery. The management and etiology of endometriosis continues to be debated, but chronic inflammation due to endometriosis may make superficial varicose uterine and ovarian veins more friable. In summary, hemoperitoneum during pregnancy is a very rare condition, and difficult to diagnose. The precise causes and incidence of hemoperitoneum during pregnancy are still unknown. We have to be aware, however, that endometriosis is a risk factor for hemoperitoneum. References
© Copyright 2010 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm10017f1.jpg] |
| |||||||||

{kind=link}