 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Reproductive Medicine Vol. 8, No. 3, Summer, 2010, pp. 119-124 Follistatin concentrations in women from Kerala with polycystic ovary syndrome Ramaswamy Suganthi1 Ph.D., PGDBI, Subbian Manonayaki2 Ph.D., Jahangir Ali Fathima Benazir1 Ph.D., PGDNBT.
Corresponding Author: Ramaswamy Suganthi, School of Biotechnology, Dr. G. R. Damodaran College of Science, Coimbatore –641 014, India. Email: sugantham2000@gmail.com Received: 13 October 2009; accepted: 14 April 2010 Code Number: rm10023 Abstract Background: Polycystic ovary syndrome (PCOS) is a disorder in which there are
numerous benign cysts that form on ovaries under a thick white covering that
is one of the causes of infertility. Follistatin is a single chain glycosylated
polypeptide that can bind to activin. When follistatin binds to activin it
suppresses the role of activin to stimulate the secretion of Follicle Stimulating
Hormone (FSH). FSH plays an important role in folliculogenesis and decrease
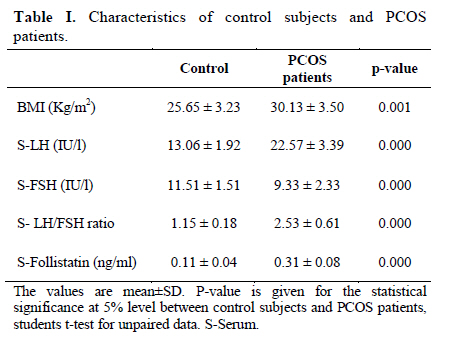
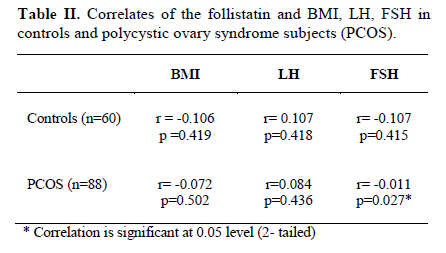
in FSH level may arrest follicular development. Key words: Follistatin, Polycystic ovary syndrome, Follicle stimulating hormone. IntroductionPolycystic ovary syndrome (PCOS) is a heterogeneous disorder affecting female infertility originally described as early as 1935 (1, 2). PCOS is very common in women under thirty years of age and have numerous benign cysts that form on ovaries under a thick, white covering (3). PCOS is an important cause of infertility as a result of chronic anovulation and menstrual irregularities such as amenorrhea or oligomenorrhea. The symptoms that contribute to this heterogeneous phenotype of PCOS are obesity and several dermatological features such as seborrhea, alopecia, acne or hirsutism (4). The syndrome has a significant reproductive and metabolic impact, and is associated with increased risk of type-2 diabetes, dyslipidemia, cardiovascular disease (CVD) and endometrial carcinoma (5, 6). Development of PCOS may require the interaction of multiple inherited and environmental factors (7). Follistatin is a single chain glycosylated polypeptide that can bind to activin. When follistatin binds to activin it suppresses the role of activin to stimulate the secretion of Follicle Stimulating Hormone (FSH) (7). FSH is very important for folliculogenesis (8); decrease in FSH level may arrest follicular development. Increased ovarian androgen production and decreased FSH levels are characteristics of PCOS. Follistatin was initially identified and isolated from follicular fluid on the basis of its inhibition of pituitary FSH secretion (1). It is expressed in multiple tissues including the ovary, pituitary, adrenal cortex and pancreas (8). It has been isolated from human placenta (9) and is also found in fetal membranes and amniotic fluid (10). The structure of follistatin is typical of “mosaic” proteins derived from exon shuffling. Follistatin is variably glycosylated at two N-linked consensus sites within the Follistatin -domain region, but these carbohydrates do not affect activin-binding bioactivity (11). Follistatin may modulate the granulose cell function in an autocrine/paracrine fashion through the binding and neutralization of activin and this will favor the process of follicular lutenization or atresia. Over expression of follistatin or an increase in its functional activity would therefore be expected to arrest follicular development (12). When a high amount of follistatin was introduced in the transgenic female mice, some of them became infertile and showed small ovaries due to the blockage of folliculogenesis and suppressed serum FSH concentration (13). Early reports highlight that the circulating follistatin concentration is higher and activin concentrations are lower in PCOS (11). Follistatin concentrations may be a useful tool to study pathological conditions in PCOS women. Thus the aim of the present study was to assess the fluctuations in circulating follistatin concentrations in PCOS patients compared to regularly menstruating women of Kerala state and demonstrating the importance of follistatin in PCOS. Materials and methods Subjects and study design The PCOS study group screened based on the NIH (14) and Rotterdam's citeria (15) consisted of 88 oligo/amenorrheic women with PCOS diagnosed by ovarian morphology assessed by vaginal ultrasonography and hyperandrogenism from different hospitals in Kerala. The criteria for a polycystic ovary were: an enlarged or normal sized ovary with multiple (10 or more) small subcortical follicles (2–10 mm in diameter). The control group consisted of 60 healthy women with regular menstrual cycles (26–30 days) and no signs of hyperandrogenism. The PCOS patients were examined during their oligo/amenorrheic periods, and the controls during the early follicular phase of the cycle (period days 3–7). Care was taken to ensure that they took no hormonal medication for at least 2 months before the study. Blood samples were obtained after an overnight fast. The sera were stored at -20ºC until analyzed. Body mass index (BMI, Kg/m2) was calculated (16) and underweight‟ was defined as BMI ≤ 19.4 Kg/m2 'normal weight' as BMI 19.5–26.4 Kg/m2, and 'overweight' as BMI ≥ 26.5 Kg/m2. Serum follistatin was measured by the quantitative sandwich enzyme immuno technique using human follistatin as a standard (R & D systems GmbH, Germany). Serum LH, and FSH were determined by an enzyme immunoassay sandwich method with a final fluorescent detection (BIOMERIEUX, France). Statistical analysis Statistical analysis of the data was carried out by Student's t-test. BMI was calculated by dividing body weight by height2, and this value was used in Student‟s t-test. In correlation analyses Pearson correlation coefficients were used. Differences were considered significant at the conventional p≤ 0.05. Statistical analyses were performed using Statistical Package for Social Sciences (SPSS version 14) (SPSS, Inc., Chicago, IL, and USA). ResultsSerum follistatin levels were 0.11±0.04 and 0.31±0.08 ng/ml in control subjects and PCOS patients respectively (mean±SD), and mean follistatin concentration in PCOS showed an increased value. The statistical difference was significant (students t-test: p=0.000) (Table I). In Pearson correlation analysis, serum follistatin was negatively correlated with BMI in control subjects and PCOS (r= -0.106, p=0.419; r= -0.072, p= 0.502) (Table II) and was not significant. The relationship between serum follistatin and Leutinizing Hormone (LH) for control study and PCOS was positively correlated (r= 0.107, p= 0.418; r=0.084, p=0.436) (Table II) and the p-values were however not significant. The relationship between serum follistatin and FSH for control study was negatively correlated (r = -0.107, p=0.415) (Table II) and it was not significant. When the same relation was done for PCOS patients, the correlation was negative (r= -0.011, p=0.027) (Table II) and significant. Discussion Studies on the pathogenesis of PCOS could not identify a single causative gene involved. Recently it has been identified that there is a relation between PCOS and disordered insulin metabolism, and this indicates that the syndrome may be the presentation of a complex genetic trait disorder (17). The features of obesity, hyperinsulinaemia and hyperandrogenaemia, which are commonly seen in PCOS, are also known to be factors, which confer an increased risk of cardiovascular disease and non-insulin dependent diabetes mellitus (NIDDM) (18). In infertile women with PCOS, usually overweight or obesity is more prevalent. The relative importance of PCOS status and overweight/obesity in this group of women is yet to be fully understood, although increasing evidence suggests that BMI contributes significantly towards the severity of many problems, such as the risk of miscarriage (19). Recently evidence for linkage between the follistatin gene and PCOS (20) was identified. This sheds some light on the genetic basis of PCOS implicating the role of follistatin gene in the disease process. Follistatin concentrations were high in subjects with PCOS (p<0.05) and were statistically significant (Table I). This investigation has shown that, circulating concentrations of follistatin are higher in PCOS subjects compared to those with no evidence of this syndrome. While the exact contribution of the ovary to circulating concentrations of this protein is not known, these data raise the possibility that alterations in secretion of follistatin from the ovary or other organs may explain the change in circulating concentration of the protein. As reported earlier, PCOS is closely linked to areas near the follistatin gene in genetic studies in women with PCOS (20). As reported by Magoffin et al (21) examination of follicular fluid from small ovaries found no difference in the activin A and follistatin concentrations between controls and PCOS in size-matched follicles, whereas inhibin B concentrations were higher in dominant follicles from control ovaries. Liao et al (22) recently reported preliminary results in follistatin gene mutations in PCOS. They did not find a mutation in the coding region of the Chinese population, but there may be changes in follistatin in other ethnic populations or indeed changes in the regulation of the follistatin gene. Norman et al (11) reported higher levels of follistatin and lower activin levels in the circulation of women with PCOS. This report of Norman et al (11) strongly supports the results of the present study. Another study by Eldar-Geva et al (23) reported that follistatin was increased by 80% - 90% in PCOS patients, independent of obesity. Moreover Philips et al (24) reported PCOS as the most significant variable that independently increased follistatin and it has been shown that virtually all-circulating follistatin in women is activin bound. Follistatin is found to be increased in PCOS subjects selected for the present study than in the normal controls and there is no significant correlation between BMI and follistatin (Table I). Similarly Eldar-Geva et al (23) reported an increased level of follistatin in PCOS patients regardless of BMI. According to Norman et al (11) there is no significant association between follistatin and BMI, which supports our findings. FSH concentration in PCOS subjects selected for the study, decreased with increase in follistatin. Table II illustrates clearly the significant (p< 0.05) association of follistatin and FSH, and recorded a negative correlation. This data is supported by the report of Odunsi and Kidd (25) that over expression of follistatin will be expected to lead to increased ovarian androgen production and reduction in circulating FSH levels, which are the features of PCOS. Supporting the present investigation Liao et al (22) reported an over expression of follistatin. However, LH level and follistatin concentration was not related both in PCOS and control subjects and did not show any significant correlation (Table II). In the rat models, follistatin modifies FSH action on rat granulosa cells, as evidenced by its inhibition of aromatase activity and inhibin production while enhancing progesterone production, follistatin reverses the enhancing effect of activin on FSH–stimulated steroidogenesis and inhibin production and inhibits activin–induced FSH receptor number and basal inhibin production by granulosa cells (12). Follistatin concentrations are high in PCOS patients than in control subjects in this study. The high concentration of follistatin in PCOS lowers the FSH level and thus follistatin and FSH levels are negatively correlated in our study. References
© Copyright 2010 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm10023t2.jpg] [rm10023t1.jpg] |
| |||||||||

{kind=link}
{kind=link}