 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Reproductive Medicine Vol. 8, No. 3, Summer, 2010, pp. 135-138 Short communication Perifollicular and subendometrial blood flow and ICSI cycle outcome Elham Pourmatroud1, 2*M.D., Batool Hosein Rashidi1*M.D., Maryam Rahmani 3M.D.
Corresponding Author: Elham Pourmatroud; Azadegan Street, Emam Khomini Hospital, Ahvaz, Iran. Email: e.pourmatroud@yahoo.com *These authors have contributed equally to this work. Received: 25 November 2009; accepted: 28 April 2010 Code Number: rm10024 Abstract Background: There is a fundamental correlation between follicles and endometrium
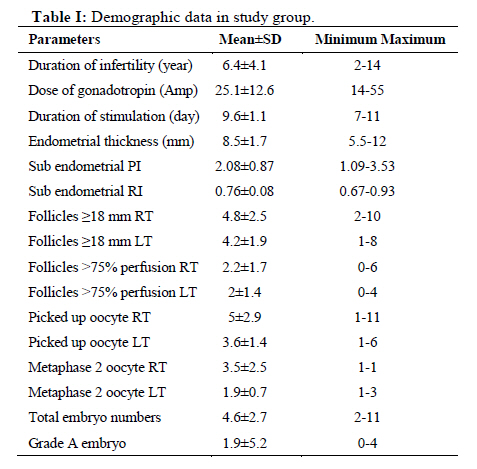
in intracytoplasmic sperm injection (ICSI) cycles. Key words: Doppler sonography, Endometrium, Follicle, ICSI. Introduction Perifollicular perfusion and ovarian stromal blood flow are useful markers for optimal evaluation of follicles, with the former having a direct relationship with follicular oxygenation and oocyte maturation (1). The chance of obtaining a high-quality oocyte, and thus a good embryo, increases when perifollicular blood flow which is preferably between 50% and 75% (2) and higher pregnancy rate will be expected when at least one embryo is from a highly-perfused follicle (3). In the past decade, several studies showed that endometrial thickness does not indicate better receptivity, nor does it have a correlation with the outcome of ART cycles (4, 5). The multi-layered endometrium is not always with pregnancy outcome, after embryo transfer. Because a good endometrial blood flow is necessary for implantation to take place in ART, Doppler sonography could be a helpful tool in the assessment of endometrial and sub-endometrial blood flow. The aim of our study was to evaluate two topics at the same time; perifollicular perfusion as well as PI (pulsatility index), and RI (Resistance index) of subendometrial blood flow. We focused on those parameters because the association between perifollicular perfusion and follicular oxygenation and oocyte maturation has been approved. Furthermore, PI and RI are the most conventional and comprehensive characters for subendomertial blood flow description. Materials and methods Subject selection This prospective-analytical pilot study was conducted in the infertility clinic (Vali-e-Asr Reproductive Health Research Centre) of a tertiary teaching hospital, affiliated to Tehran University of Medical Sciences, Tehran, Iran. Approval was obtained from institutional Research Ethics Board. Also, oral consent was taken from all participants. All subjects were 20-35 years old women who were in the first ART cycle. All participants were non-smokers, did not use any drug and had normal basal follicle stimulating hormone level (FSH<10 mIU/ml) and regular menstruation cycles. Exclusion criteria were: 1) History of or present disease of uterus such as endometrial polyp, uterine myoma or congenital uterine anomaly. 2) History of or present disease of ovaries (like ovarian cyst) or fallopian tubes (especially hydrosalpinx) (7). 3) History of or present endometriosis which has been confirmed by laparoscopy. Within a period of six months (July 2008- December 2008), ten patients met all the above-mentioned criteria and were enrolled into the study. ICSI protocol Rutine OCP+long GnRH agonist protocol (Superfact, Avantis, Germany+Gonal F, Merk serono, Germany) was used for ovarian stimulation. Patients with only one 18mm follicle or excessive ovarian response with tendency of developing ovarian hyperstimulation syndrome (OHSS) were excluded from the study. Oocyte retrieval was done with vaginal sonographic guidance 36-40 hours after HCG (Pregnyl, Organon, Spain) administration. From each ovary, oocytes in metaphase II maturation phase were determinated separately. Intra-cytoplasmic sperm injection was performed for fertilization of oocytes. On the third day, eight-cell embryos of equal size and regular blastomeres (grade A) (8) calculated in each patient and a maximum of two grade A embryos were transferred vaginally and if there, the others were frozen. Luteal phase support was started from oocyte pickup day by micronized vaginal progesterone (400mg BID) and continued for 14 days. Pregnancy was then checked by the serum βhCG level and luteal support was continued in case of positive result. Six weeks after embryo transfer, vaginal ultrasonography was done in pregnant women to determinate the status of pregnancy. Intervention Ultrasonographic evaluation was done on the day of oocyte retrieval. In order to reduce diurnal variation of blood flow, patients evaluated on the morning (7.5-8.5AM) before going to the operation room (9). All 2D ultrasonographic measurements were performed by a single observer, using a 7.5 MHz transvaginal transducer (EV 9-4) with colour Doppler facility (Siemens Sonoline G605). At first, conventional vaginal 2D-ultrasonography was done and the number of follicles≥18mm in each ovary, maximum endometrial thickness (mm), and its morphologic appearance (triple-layer or non-triple layer) were determinated. After that, the power Doppler window was placed on the highest longitudinal plane of both ovaries (with normal quality of colour, colour gain - 3.4 pulse repetition frequencies of 600HZ and wall motion filter of 50HZ). When an adequate power Doppler signal was obtained, perifollicular perfusion was evaluated according to follicular circumference. Follicles with ≥75% perfusion were determinated in each ovary. If “flash” artefacts were seen (due to patient’s breathing or intestinal movement), the evaluation was repeated until a constant result was achieved. The probe was then placed over the longitudinal section of the uterus, which presents the whole subendometrial area. The uterine subendometrial region was evaluated using a scanning angle of 90 degrees and colour setting. The form of the velocity wave was analyzed in at least three points during three to five cardiac cycles and mean RI and PI values were calculated. Statistical analysis Data were entered into SPSS version 11.5 computer software and subsequently analyzed using statistical tests. Student’s t-test was used for quantitative parameters. Correlation was assessed by Pearson method. P-value <0.05 was considered as significant (power study was 80%). Results The mean age of patients was 28.2±4.7 years (range=21-35years). Eight patients had primary and two had secondary infertility. Causes of infertility were: unexplained (3 cases), male factor (4 cases), ovulatory dysfunction (2 cases), and tubal factor (2 cases). One patient had two infertility factors. Other data of the subjects have been listed in table I. Resistance index (RI) and pulsatility index (PI) had direct correlation (p-value=0.007). Neither endometrial thickness nor its appearance had any relationship with subendometrial blood flow, RI, or PI. Also, the dose of gonadotropins and duration of ovarian stimulation had no effect on these parameters. There was a significant correlation between bilateral ovarian follicles with ≥18 mm in diameter and the number of follicles with ≥75% perifollicular perfusion (p-value=0.004), but none had a relationship with the number of metaphase II oocytes or grade A embryos. Also, the total number of oocytes picked-up from the right ovary correlated with the number of metaphase II oocytes (p-value=0.006) and the total number of embryos (p-value=0.005). Surprisingly, the total dose of gonadotropins has a positive correlation with grade A embryos (p-value=0.01). Regarding the correlation between subendometrial blood flow or perifollicular perfusion with other parameters, a significant negative relationship was found to exist between subendometrial RI and ≥75% perfused follicles in the right ovary (p-value=0.040) and a positive relationship was found to exist with the total oocytes retrieved from the left ovary (p-value=0.01). In this study, two patients became pregnant but none of the parameters were found to have significant relationship with this outcome. Discussion In this study, due to the presence of several confounding factors and strict inclusion criteria, we finally managed to enroll only ten patients. Unfortunately, the correlation between clinical outcome and colour Doppler ultrasonographic parameters was not efficacious with our low study population. In order to increase the chance of pregnancy in ART cycles, better synchronization between ovarian follicles and the endometrium is required; with a suitable oocyte (metaphase II), endometrial receptivity must be around a specific time (implantation window). Therefore, it would be more helpful if utero-ovarian vascularity was assessed at the same time, especially in cases with monofollicular cycles (10) or in patients which need natural cycle, such as those with specific medical conditions. On the other hand, although there is evidence suggesting a link between uterine and ovarian perfusion and outcome of ART cycles (11), however it is difficult, at present, to interpret the actual relationship. In our study, we found a new correlation between resistance index (RI) of subendometrial blood flow and ovarian response but we couldn't explain why the correlation was negative in one side. Probably if other parameters like flow index (FI) or vascularization index (VI) were used, our results would have been different. Also, another explanation would have been needed if the evaluation had been done on the day of HCG administration (12) or if it was repeated within two or three days (13). In conclusion, we believe that the utilization of Doppler ultrasonography usage in ART cycle is in its primary stages. This report re-emphasizes that: the evaluation with Doppler ultrasonography should focus on two compartments together as one functional part at the same. It means even in presence of good markers in each part, the final decision must be taken by co-evaluation of follicles and endometrium. References
© Copyright 2010 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm10024t1.jpg] |
| |||||||||

{kind=link}