 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Reproductive Medicine, Vol. 8, No. 4, 2010, pp. 161-166 Relationship between anti-mullerian hormone and assisted reproductive technique outcome in patients with polycystic ovary syndrome Marzieh Agha Hosseini M.D., Ashraf Aleyasin M.D., Atossa Mahdavi M.D., Sara Mokhtar M.D., Leila Safdarian M.D., Parvin Fallahi M.L.D. Department of Infertility, Shariati Hospital, Tehran University of Medical Sciences, Tehran, Iran. Corresponding Author: Atossa Mahdavi, Department of Infertility, Shariati Hospital, North Karegar Street, Tehran, 1411713135, Iran. Email: atossa_mahdavi@yahoo.com Received: 19 December 2009; accepted: 2 June 2010 Code Number: rm10028 Abstract Background: Anti-mullerian hormone (AMH) levels may represent the ovarian follicular
pool and could be a useful marker of ovarian reserve. The clinical application
of AMH measurement has been proposed in the prediction of quantitative and
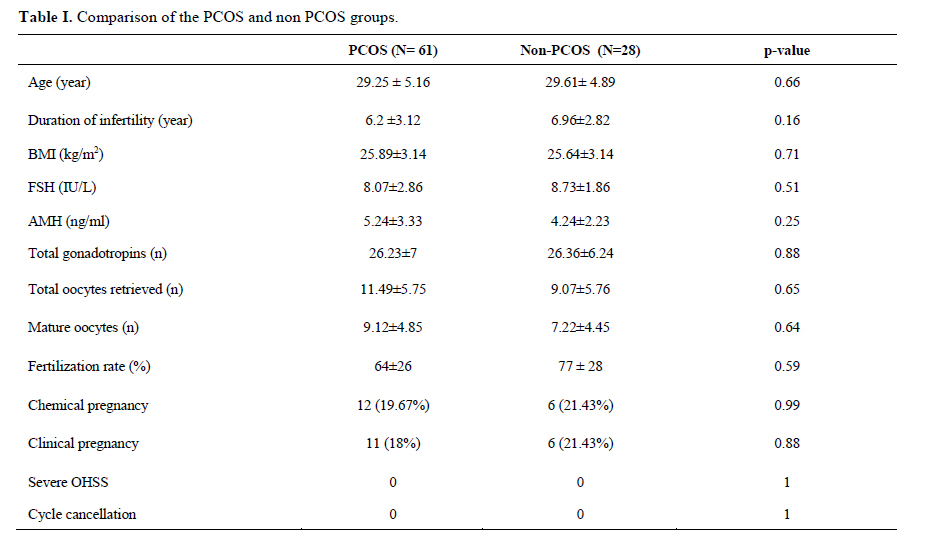
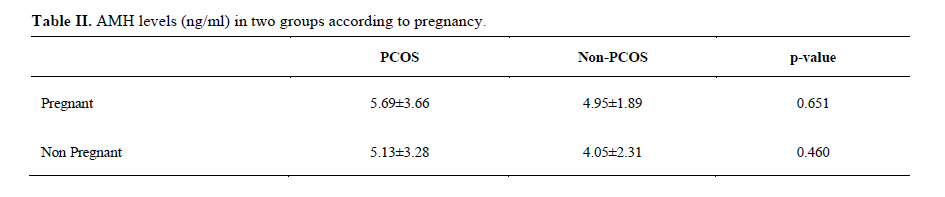
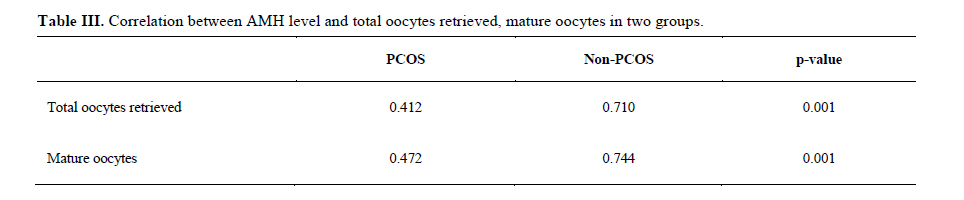
qualitative aspects in assisted reproductive technologies. Key words: Anti-Mullerian hormone, Polycystic ovary syndrome, Assisted reproductive technique. Introduction Fertility clinicians have been faced with the challenge of determining the degree of ovarian reserve to better tailor assisted reproductive technology (ART) treatment. The costly drug regimens, the discomfort to patients and the significant risk of complications associated with ovarian stimulation, all justify the need for obtaining clinically relevant information before commencement of treatment (1). A useful biomarker of ovarian response to controlled ovarian hyperstimulation in assisted reproduction is needed (2). Many tests have been developed to screen for diminished ovarian reserve. Traditional methods used to predict prospectively response to ovarian stimulation. These included mainly the measurement of baseline cycle day 3 serum concentrations of hormones such as FSH, estradiol and inhibins, or ultrasonographic tests such as pretreatment ovarian volume and the number of early antral follicles (3). Recently, anti-mullerian hormone (AMH), also referred to as Mullerian-inhibiting substance, has been proposed as a novel marker for predicting ovarian response to gonadotropin stimulation (2, 4). Antimullerian hormone is a member of the transforming growth factor beta super family (5). In the women, it is solely produced by the granulosa cells of growing preantral and small antral ovarian follicles. Serum AMH levels may be used as a marker of ovarian reserve, representing the quantity and quality of the ovarian follicle pool (5-7). Women with PCOS are known to have elevated baseline AMH levels when compared with age-matched normoovulatory women (8, 9). As a marker for ovarian reserve, MIS/AMH correlates positively with ovarian response to COH in normoovulatory women, but this has not been assessed in women with polycystic ovary syndrome (PCOS) (10). Disturbed dominant follicle selection leading to an excess accumulation of preantral and small antral follicles in women with PCOS presumably causes the elevated MIS/AMH levels (10). Although MIS has been shown to reflect antral follicle counts and to be elevated in PCOS, it is unclear how well measurements of MIS may reflect ovarian morphological parameters in PCOS, specifically ovarian size and blood flow (8). Searching available literature, we did not find any study comparing ART outcomes according to AMH levels between PCOS patients and non PCOS patients. To gain further insight about MIS/AMH as a predictor of ovarian response, we investigated the relationship between the serum levels of anti-mullerian hormone (AMH) and results of assisted reproductive techniques (ART) in PCOS patients versus non PCOS patients (Control group). Material and methodsIn this cohort study, 61 polycystic ovary syndrome (PCOS) patients and 28 non PCOS patients (controls), candidates for assisted reproductive technique entered the study. The study was conducted in the infertility department of Shariati Hospital, affiliated to Tehran University of Medical Sciences during 2008. The project was approved by the ethical committee of the infertility department of the university and was initiated after achieving written consents of the participants. PCOS diagnosis was according to Rotterdam criteria (9). According to the Rotterdam criteria, we accepted the presence of two of the three following characteristics for inclusion in the study: (1) oligomenorrhea/amenorrhea, (2) clinical (hirsutism) or biochemical finding of hyperandrogenism, and (3) polycystic ovaries on transvaginal sonography. All the patients aged less than 35 years with normal prolactin and thyroid hormone levels and normal male spermogram in their spouse. In the control group, 28 patients candidates for COH and ART due to unexplained or/and tubal factor infertility were selected. Ages, body mass index (BMI), and duration of infertility were similar between two groups. In all patients the serum levels of anti-mullerian hormone (AMH) was measured on the 3rd day of menstrual cycle. Serum AMH was measured by enzyme-linked immunosorbent assay (ELISA) using the MIS/AMH ELISA kit (DRG instruments GmbH, Germany). The patients underwent controlled ovarian hyperstimulation (COH) with Gonadotropin/GnRH-agonist long protocol. All the participants received folic acid 1mg/day before initiating the induction cycle, low dose oral contraceptive pills on day 3 of the previous cycle and doxycycline 100 mg twice a day for the first 10 days of the previous cycle. Long term desensitization protocol using the GnRH agonist Buserelin 500 micrograms subcutaneously was started at the day 21 of the previous cycle. After complete desensitization, ovarian stimulation using Gonal F (Serono, Switzerland) was commenced on day 3 of the next cycle at a daily dose of 150 IU. It was replaced by HMG (Ferring, Germany) after the 7th day of the stimulation. Transvaginal ultrasound (Siemens, Sonoline G20) for follicular development was done every 3-5 days. Final oocyte maturation was triggered when at least 2 follicles with diameter of at least 17 mm was observed, with HCG (Ferring, Germany) 10000 IU administered as a single intramuscular injection. Oocytes were collected 36-38 hours later using transvaginal guided follicle aspiration under general anesthesia. After fertilization through intracytoplasmic sperm injection (ICSI), three good quality embryos were transferred transcervically 3 days later. Luteal phase support was started the day after ovum pick up by administration of progesterone suppository Cyclogest (Actavis, UK), 1200 mg daily. Chemical pregnancy was detected by serum beta-hCG analysis 14 days after embryo transfer and transvaginal ultrasound scan was scheduled 2 weeks later to detect the gestational sac of pregnancy. Primary outcome measure was pregnancy and secondary outcome measures were stimulation cycle characteristics. Age, body mass index (BMI), infertility duration, number of oocytes retrieved, number of mature oocytes, number of gonadotropin injections, chemical pregnancy, clinical pregnancy, ovarian hyperstimulation syndrome (OHSS) and cycle cancellation were considered. The relationship between serum level of measured hormonal markers with retrieved oocytes, mature oocytes and pregnancy rate were assessed. Statistical analysis For each participant a questionnaire was filled by the researchers. Data were collected from questionnaires, clinical, laboratory notes and ultrasound reports. SPSS16 software (SPSS Inc. Chicago IL.) was used for data collection and analysis. T-test, Mann-Whitney U-test for quantity data, χ2 and fisher’s exact test for quality variables, Pearson test for correlation were used. P value less than 0.05 was considered for statistical significance. ResultsThe mean±SD age of patients in PCOS group was 29.25±5.16 years and in control group was 29.61±4.89 years (p=0.655). The duration of infertility was 6.2±3.12 years in PCOS group and 6.96±2.82 years in non PCOS group (p=0.161). Body mass index (BMI) of patients in PCOS group was 25.89±3.14 kg/m2 and in control group was 25.64±3.14 kg/m2 (p=0.708). The MIS level in PCOS group was 5.24±3.33 ng/ml and in non PCOS group was 4.24±2.23 ng/ml (p=0.251) (Table I). In PCOS group total oocytes retrieved was 11.49±5.75 and in non PCOS group was 9.07±5.76 (p=0.65). The number of mature oocytes was 9.12±4.85 in PCOS group and 7.22±4.45 in control group (p=0.64). Fertilization rate was 64±26 percent in PCOS and 77±28 percent in control group (p=0.59). Twelve cases in PCOS group and six cases from non PCOS group had chemical pregnancy (positive beta HCG). Eleven cases in PCOS group and six cases in non PCOS group had clinical pregnancy (pregnancy sac on ultrasound scan). Severe ovarian hyper stimulation syndrome (OHSS) and cycle cancellation were not reported in any groups (Table I). Although AMH level was higher in pregnant group (in both PCOS and non PCOS groups) but there was no significant difference between AMH levels in both groups according to pregnancy (Table II). There was a significant direct correlation between the serum MIS (AMH) level with number of total oocytes retrieved (r=0.412), and mature oocytes (r=0.472) in PCOS group and there was a significant direct correlation between MIS (AMH) level with number of total oocytes retrieved (r=0.710) and mature oocytes (0.744) in control group (Table III). There was not a significant difference between two groups. Discussion This study revealed that AMH is not a definite predictor for pregnancy and ART results in PCOS patients. Although, it is proven that AMH measurement prior to gonadotropin stimulation could provide useful information to direct the application of mild patient-friendly stimulation protocols in order to avoid OHSS (7). Evaluation of patients who underwent Assisted Reproductive Technique (ART) is very important for both patients and physicians, because it is very expensive and time consuming and stressful for patients. It is important to predict who poor responder is before starting the procedure. Nowadays many tests such as FSH, estradiol, inhibins, antral follicle count (AFC), testosterone and free testosterone for predicting ovarian reserve are suggested. Thus, despite the different validity of all these tests, there still remain patients who respond poorly to stimulation despite having normal tests of ovarian reserve. This supports the idea that ovarian reserve is not a simple static anatomic number and is not yet fully understood (11). Participants in our study had the same age, though despite their same mean BMI they seemed somewhat overweight. Basal characteristics (including basal AMH) and cycle characteristics of the 89 patients were similar. In recent studies AMH has been proposed as a new method for predicting ovarian reserve. According to Aflatoonian et al, small AFC and AMH are equally accurate predictors of high ovarian response to COH and allow us to identify the patients who are at increased risk of OHSS prior the commencement of stimulation, and help to determine the appropriate treatment protocols (12). AMH is the most significant predictor of embryo quality (AUC =0.728) (12). It has the ability to predict poor and excessive response to stimulation with exogenous gonadotropins. This biomarker is superior to basal FSH and AFC, and has the potential to be incorporated in to work-up protocols to predict patient's ovarian response (1). On the other hand, serum level of AMH is a good predictor of the ovarian response to COH in normoovulatory women but not in PCOS (10). This study showed that, there was not a statistically significant difference between AMH level and pregnancy in PCOS in contrast to the control group. Wang et al, stating that baseline MIS/AMH is not a good predictor of the ovarian response to COH in PCOS women. The arrest of follicular growth and the heterogeneity of FSH sensitivity among MIS/AMH-secreting follicles in PCOS render baseline measures of MIS/AMH a poor predictor of the gonadotropin response in PCOS (10). However, there are few published studies confirming the relation between AMH and ovarian response in COH in this group of patients exclusively. In a recent study to relate follicular fluid AMH and FSH levels in patients with PCOS, it was suggested that the granulosa cells from polycystic ovaries continue to produce elevated levels of AMH, possibly because of impaired access of FSH to follicles. Such an excess in follicular fluid AMH may have harmful consequences on oocyte quality and final maturation (13). Polycystic ovaries have an abnormally rich pool of growing follicles and a disturbance in the selection and subsequent maturation of a dominant follicle. Increased serum AMH is due to increased production per granulosa cell, suggesting an intrinsic granulosa cell dysregulation in PCOS. Not only is AMH expression increased, but it also might be protracted in polycystic ovary (PCO) follicles. The potential role of AMH on oocyte quality could be future field of reproduction research. There was not a significant relationship between AMH levels and pregnancy rate in our study. This raises the hypothesis of a negative link between AMH and final oocyte maturation. In the four studies which evaluated the role of MIS/AMH in pregnancy prediction, two studies (14, 15) supported it and two studies did not (16, 17). On the other hand pregnancy rates after IVF are influenced by multiple (non-ovarian) factors including in vitro laboratory conditions, semen parameters, psychological stress and technique of embryo transfer. Predicting response to gonadotropin treatment; nevertheless, remains an important aim in the evaluation of the couple struggling with infertility (18). Our study, despite its limitations like small sample size, has the benefit of comparing PCOS patients with a control (non PCOS) group which recommends further well designed investigations in this regard. Acknowledgement The authors would like to thank the staff of Infertility Department and Endocrine Research Center of Shariati Hospital. References
© Copyright 2010 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm10028t1.jpg] [rm10028t2.jpg] [rm10028t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}