 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Reproductive Medicine, Vol. 8, No. 4, 2010, pp. 173-`78 Is karyotyping and Y chromosome microdeletion study necessary in men candidate for ICSI? Mohammad Reza Nowroozi1 M.D., Keivan Radkhah1 M.D., Alireza Ranjbaran1 M.D., Saeed Reza Ghaffari2 Ph.D., Mohammad Ali Sedighi Gilani3 M.D., Hamid Gourabi4 Ph.D.
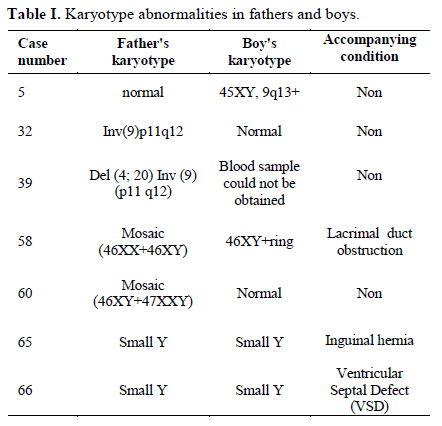
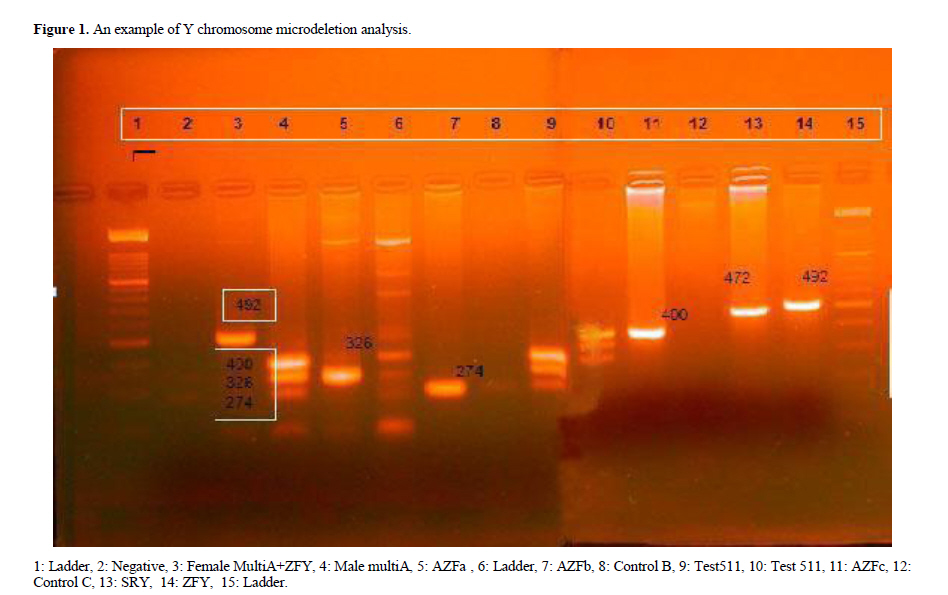
Corresponding Author: Mohammad Reza Nowroozi, Department of Urology, Tehran University of Medical Sciences, Urology Research Center, Tehran, Iran. Email: mrnowroozi@yahoo.com Received: 29 July 2009; accepted: 14 March 2010 Code Number: rm10030 Abstract Background: The sperm count and function may be affected by karyotype abnormalities or microdeletion in Y chromosome. These genetic abnormalities can probably transmit to the children. Key words: Y chromosome microdeletion, Karyotype, Intracytoplasmic Sperm Injection (ICSI). Introduction Men with azoospermia and severe oligospermia, who were not afforded to bear child before, can experience fatherhood in blessing of intracytoplasmc sperm injection (ICSI) nowadays. Chromosomal abnormalities are responsible for azoospermia in some cases, in another subgroup, microdeletion of Y chromosome is the actual chromosomal abnormality, while the karyotype appears to be normal (1-4). Chromosomal abnormities may be transmitted to the offspring, and Y chromosome microdeletion is vertically transmitted to all the sons (5-10). In this way, offspring inherits some or all the chromosomal abnormalities existing in parents. So it would be ethical to put it forth to the parents, before going forward to assisted reproductive technology (ART). Chromosomal studies could be considered in every case of azoospermia and severe oligoasthenotheratospermia in future. De novo appearance of chromosomal abnormalities after conception might be of concern in ICSI (11). If de novo chromosomal abnormalities are clinically significant, preimplantation genetic diagnosis (PGD) may be practiced routinely before embryo transfer. This study had been designed to study the extend and significance of such chromosomal abnormalities. Materials and methods This cross-sectional study aimed men with male factor infertility who were candidate for ICSI and the result was a live born son. They were gathered by making phone call from the IVF center where they had done ICSI. Informed consent was obtained in all cases. Male factor infertility was assured by reviewing their medical records. The result of testis biopsy in azoospermia and semen analysis in cases of severe oligoastheno-theratospermia was seen to. A complete history consisted of spouse ages at the time of delivery; duration of infertility, and previous ART experiences (successful or unsuccessful) was obtained. The method of delivery (normal vaginal delivery or caesarian section) and fetal age at delivery beside the history of previous surgeries and medical conditions were asked for. A general physical exam performed for overall physical and mental health and development and a genital exam was made for hypospadiasis and undescendent testis. Blood samples were taken from fathers for karyotyping and Y chromosome microdeletion study, and from the sons for karyotyping. The blood was banked for Y chromosome study in the sons; this study would have performed only if their fathers showed microdeletion. Genomic DNA was extracted from peripheral blood samples using the Genomic DNA Extraction kit (Bioneer, Korea). Deletion method for Y-microdeletions was based on three multiplex PCRs [1]. It includes of nine STS amplified in three multiplex PCRs: sY158 (AZFb), sY254 (AZFc), sY157 (AZFc), sY154 (AZFc), sY142 (AZFb), sY134 (AZFb), sY84 (AZFa), sY83 (AZFa) and SRY (sY14) as internal controls. PCR products were run by electrophoresis on a 3.3% agarose gel and stained with ethidium bromide for visualization under UV light. We studied two to four STS markers for each AZF regions to coverage the sparse regions of Yq chromosome and when the studied marker of the region were not completely deleted, it assign as partial against full deletion. Each deletion analyzed was verified by repetition of PCR experiments. Informed written consent was obtained from all patients who underwent in this study (12). Chromosome preparations were made from routine peripheral blood lymphocyte cultures according to the modifications of Verma and Babu (13). Lymphocytes from heparinized fresh peripheral blood were cultured. Whole complete blood cultures were set up in10 ml culture tubes, the medium had the following composition: 100ml RPMI medium (Sigma) supplemented with 20ml fetal calf serum (Gibco BRL), 1.2ml L-Glutamine (Sigma), 1ml phytohemagglutinin (Sigma) and penicillin streptomycin (Sigma) mix. Five to ten drops of heparinized blood were added to 5 ml of the complete media .Culture tubes were incubated for 72 hours in a slanted position at 37˚C. Colcemid (Sigma) was added at 4μg/ml to the cultures 2 hours before harvesting and mixed by shaking gently. Slides were prepared after hypotonic treatment of the cells with KCL (0.075M) followed by fixation in fresh ethanol/glacial acetic acid (3/1vol/vol). A concentrated suspension of the cells was dropped on slides, which were dried in room temperature. G-banded chromosomes were obtained by aging the slides in a dry oven at 55-60˚C, removing and bringing them to room temperature just prior to banding then treating with standard trypsin solution and stained in 4% Giemsa solution (Merk), dried and examined microscopically using the image analyzer programmed (Cytovision, version 2008, Applied Imaging). Metaphases were karyotyped and interpreted according to the International System for human Cytogenetic Nomenclature (ISCN) (14). Statistical analysis The data were collected and descriptive analysis was performed by using SPSS software. Results The mean age of 70 fathers at the time of their sons’ birth was 35.11±4.9 years (range, 26-44 years), while mothers were 30.5±4.1 years (range, 22-38 years) at the occasion. These parents experienced infertility for 8.7±4.6 years before conception with ICSI with the maximal infertility of 19 years. The sons aged 2.4±1.8 years old in average at the time of exam, the youngest infant was 6 months and the oldest child was 6 years old. The average fetal age at the time of delivery was 33±5.8 weeks, the earliest preterm delivery was at 26 weeks in a twin pregnancy ended with emergency caesarian section which lead to mentally retarded handicapped children, and the latest was 42 weeks at term with no post term mothers. 18.6% of mothers had unsuccessful IUI trials before the success in ICSI, and each mother in this group experienced IUI for 1.8 times (between 1 and 3 courses). History of previous unsuccessful IVF-ICSI obtained in 8.6% of the mothers. They have had tried IVF on for 1.38 times, all had only one or two failed course. The first ICSI course was achieved live birth in 76.7%, and in 18.6% the second and in 4.7% the third course over came. ICSI was indicated in 62.1% due to severe oligospermia and in 37.9% because of azoospermia, and only 6.9% of them proved to be obstructive in nature. All the mothers delivered under caesarian section, 42.9% in preterm course in which 2 cases (2.9%) suffered from mental retardation due to severe prematurity. Overall 13 children had some kind of problem. 57.1% of pregnancies were singleton, while 40.5% and 2.4% were twins and triples consecutively. In genital exam, 8.6% of boys had hypospadiasis; all had distal hypospadiasis and none occurred proximal. 7.1% of boys had history of undescendent testis, in 5.7% bilateral and in 1.7% unilateral UDT were observed. Five cases had medical consequences which lead to operation, although they were overall healthy by now. One had gastroesophageal reflux with pneumonia probably due to aspiration, one case happened to have bilateral inguinal hernia, the other one had lacrimal ducts obstruction. In one case hypothyroidism coincided with inguinal hernia, and in another one, ventricular septal defect (VSD) was the cause of operation. We detected 6 cases of karyotype abnormalities in 70 fathers. In one case Inv (9) (p11q12) was found in father while the son revealed normal karyotype. In other case of Del (4; 20) Inv (9) (p11 q12) in father we could not obtain blood sample form the infant boy despite of frequent trial by 9 experienced persons. One of the fathers proved to have mosaicism 46XY+46XX; although the son was 46XY, he had ring formation in chromosomes; this was the very case with lacrimal ducts obstruction. Another father with mosaicism of 46XY+47XXY had son with completely normal karyotype. In 2 cases small Y in fathers directly transmitted to the sons after ICSI. Only in one case the son had De novo chromosomal abnormality 45XY, (9q13+) without father's abnormality. This boy was 6 years old at the time of study and had normal mental performances and physical exams. Table I summarizes data. Deletion of Y chromosome was not found in 70 fathers in AZFa, AZFb, or AZFc locations. Discussion Disregard to descriptive data, like age and duration of infertility which are similar to other ICSI groups, some points about safety and long term results of ICSI are to be discussed further. In our study, we detected 7% chromosomal abnormality in fathers who experienced successful ICSI. Most of the abnormalities were minor or mosaicism. It is to be emphasized that this figure is lower than we expect from severe oligospermic and azoospermic patients who are candidates of TESE, as a great portion of major karyotype abnormalities like Kleinfelter with negative TESE have been omitted. Mihura (15) reported 5.1% chromosomal abnormality in infertile men in Japan, while Nagvenkar and coworkers (16) reported overall 10.2% chromosomal abnormality in the same group. They also estimated this amount in azoospermic 14.3% and 6.5% in oligospermic men. It seems that genetic and race can also affect chromosomal abnormality in infertile men. In our study, we found 8.6% hypospadiasis in ICSI boys, which is fairly higher than general population. Several other studies are in agreement and reported a higher rate of hypospadiasis in ICSI (17-20). Although Källen and associated researchers (21) reported no difference between hypospadiasis and other congenital defects in IVF and ICSI, Lie and coworkers (22) claim that major birth defects increases by 1.12 folds in ICSI compared with IVF. In some studies 3 to 10 fold increase in major birth defects like neural tube defects are reported (18-19), others believe that except hypospadiasis there is no increase in rate of congenital anomalies in IVF and ICSI (21). Pinborg and associates (23) mentioned the risk of anomalies increases with multiple pregnancies and decrease in gestational age. In our study, the only major anomaly which was mental retardation occurred in twins with low gestational age. Y chromosome microdeletion reported in 5 to 10% of cases in azoospermia or severe oligospermia (24-27). Sperm can be retrieved in many of these cases, but live births are not as commonly reported and it is only limited to few reports of vertical transmission (28), otherwise in an ICSI series of more than 1000, 12 to 25 cases of vertical transmission are expected. Besides, there is only one known case of natural transmission of Y chromosome ring abnormality (not even deletion) (29). In our successful ICSI cases who father a son, we did not find any case of Y chromosome microdeletion. This might be due to lower frequency of microdeletion in Iranian cases or most probably because of unsuccessful practice of ICSI in cases with microdeletion. So, Y chromosome analysis before ICSI performance may be used more to determine the probability of unfulfilled ICSI than the possibility of vertical transmission to offspring, although that might be of special concern. In addition some studies mentioned the incomplete penetrance of the deletion (30). In order to convey the precision we made in Y chromosome analysis a typical example of this study is given in figure 1. Conclusion Y chromosome microdeletion is not prevalent in fathers with successful ICSI. We concluded from our study that it is not necessary to analyze Y chromosome microdeletion before performing ICSI in azoospermic men or those with severe oligospermia, provided that they are counseled about the vertical transmission. Only if the patient is determined to call off ICSI in case of microdeletion, it would be vise to perform the analysis before ICSI. On the contrary, we suggest chromosomal study in these cases to determine the risk and future abnormalities in offspring, as Karyotype anomaly may be transmitted to the sons. Most of the complications are the result of prematurity. All together, ICSI is a reliable and safe method for treatment of severe oligospermia and azoospermia. Acknowledgment This study has been performed with financial support of Tehran University of Medical Sciences. The authors express their greatest acknowledgment to all the personnel and colleagues in following settings, without their assistance this study could never be achieved. Vali-asr Hospital Fertility and Infertility Center, Urology Research Center, Alvand Hospital IVF Center, Rooyan Institute, Gene Genetic Lab, Mrs. Rezaii and Dr Zarrabi. References
© Copyright 2010 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm10030f1.jpg] [rm10030t1.jpg] |
| |||||||||

{kind=link}
{kind=link}