 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Iranian Journal of Reproductive Medicine Vol. 9, No. 1, Winter 2011, pp. 21-24 Infertility in Mazandaran province - north of Iran: an etiological study Abbasali Karimpour Malekshah1 Ph.D., Amir Esmailnejad Moghaddam2 Ph.D., Narges Moslemizadeh3 M.D., Sepideh Peivandi3 M.D., Ayyub Barzegarnejad4 M.D., Nadali Musanejad4 M.D., Gholamali Jursarayee5 Ph.D.
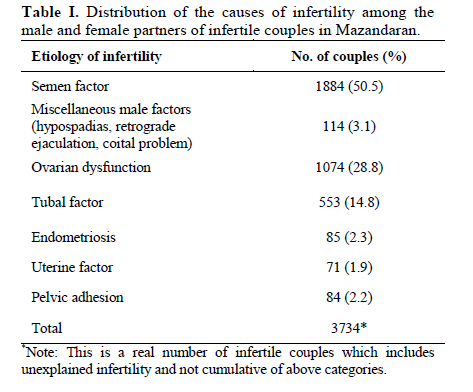
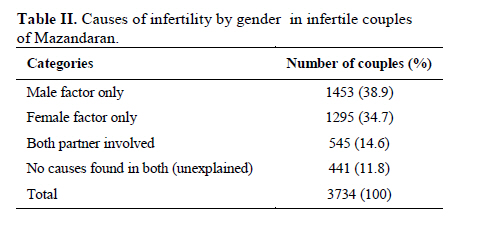
Corresponding Author: Ayyub Barzegarnejad, Department of Urology, Imam University Hospital, Infertility Center, Mazandaran University of Medical Sciences, Sari, Iran. Email: ayubbarzgarnejad@gmail.com Received: 22 December 2009; accepted: 31 July 2010 Code Number: rm11004 Abstract Background: The prevalence and etiology of infertility are not similar in different parts of the world. There are only few reports of this topic in Iran. Key words: Primary infertility, Secondary infertility, Male factor, Ovarian dysfunction, Varicocel. Introduction Infertility, defined as the inability of couple to achieve conception after at least 1 year of regular unprotected intercourse, is a common problem in the world and affects about 8-12% of couples (1). The levels and patterns of infertility apparently vary widely and also are different in developed countries compare to those in developing regions of the world (2).We found in our previous study, a prevalence of 13.2% of infertility in Mazandaran province - north of Iran (3). But Vahidi et al (2006) reported a prevalence of 24.9% of infertility around the country (4). Cultural, socioeconomic, health care practices and policies and environmental factors play a major role in the prevalence and etiology of infertility (5). Also the proportions of causes of infertility have changed over time (6). The most cost-effective approach to solving the infertility problem is prevention and education. Further research in both developed and developing countries is needed to understand the high prevalence and causes of infertility (7). There are only a few reports on this topic in Iran (8,9) Therefore, determination of the clinical patterns and a review of the major causes of infertility in north of Iran were the main objectives of this study. Materials and methods In this descriptive study the medical records of 3734 consecutive couples attending two infertility centers in Mazandaran province, from 2003 to 2008, were reviewed. A complete history was taken and a complete physical examination was performed for all patients. In the men, particular attention was paid to the pattern of pubertal development, history of cryptorchidism, inguinal surgery, mumps, orchitis, testicular torsion, viral illness, and sexually transmitted diseases. The external genitalia were examined for number, site, and size of the testes and presence of varicocele and any other congenital or acquired defect. In the women, the emphasis in history was on the pattern of pubertal development, menstrual history, galactorrhea, any virilization or defeminition, and drug or hormone intake. Sexual history focused on libido, erectile function, frequency and timing of intercourse. Specific investigations performed for the male partner included semen analysis and hormone estimations. Semen analyses were performed according to the method described in the World Health Organization laboratory manual (10). A detailed gynecologic examination was carried out to ascertain cervical cause of infertility such as cervical stenosis, abnormal cervical mucus, or diseases such as endometriosis. The specific investigations performed for the female partner included tests for documentation of ovulation (gonatorophins and steroids assays and ultrasonography), test for tubal patency, and laparoscopy (when indicated). Tubal patency was assessed hysterosalpinography. Laparoscopy was performed in some cases to study tubal diseases and to look for endometriosis. Statistical analysis Descriptive statistics and statistical analysis was performed using the software package SPSS 13. Results The total of 3734 infertile couples were assessed in this study. Of these, 2941 (78.7%) couples had primary infertility and 793 (21.3%) had secondary infertility. The mean age (±SD) of the men was 33±7 (range, 21-64 years), and the mean age (±SD) of the women was 29 ± 6 (range, 17-47 years). The mean duration (±SD) of infertility at the time of presentation to infertility clinic was 5.7±4 years. The distribution of causes of infertility in study couples is shown in Tables I and II. Of the entire of infertile couples, 38.9%, 34.7% and 14.6% had infertility due to at least a male factor, a female factor and both couple involvement respectively. In 11.8% of infertile couples, the cause remained unexplained (Table II). Semen factor was the most common identifiable etiologic factor, documented in 1884 (50.5%) couples. Among these men 804, (42.7%) had varicoceles. Other important causes were vas deferens agenesis (1.2%), cryptorchidism (0.5%), and testicular torsion (0.1%). In 1045 (55.5) men, no cause could ascertained. Ovarian dysfunction was the second most common etiologic factor of infertility, recognized in 1074 (28.8%) women. Of these 610 (56.8%) women had polycystic ovary syndrome. Tubal factor was the other main etiologic factor of infertility, recognized in 553 (14.8%) women (Table I). Discussion In this study a relatively high frequency of primary infertility (78.7%) was observed. While secondary infertility was determined in 21.3% of couples. This finding confirms other regional and national studies in this aspect (11,12). The most comprehensive study of infertility- a WHO study of 5800 infertile couples seeking help at 33 medical centers in 22 developed and developing countries- found that most infertile couples around the world suffer from primary infertility (13). Sub-Saharan Africa is an exception, in this region most couples (52%) suffered from secondary infertility (13). A study was conducted by Orhue and Aziken (2007) in Nigeria confirmed WHO report and showed even greater discrepancy in parity distribution. According to their findings the percentage of secondary infertility is 85.7% among infertile couple of Nigeria (14). Latin America also had a relatively high rate of secondary infertility (40%). In contrast, only 23% of infertile couples in Asia and 16% in North Africa suffered from secondary infertility (13). Mongolia is an exception in Asia with 43.7% of secondary infertility (15). The results of WHO study suggest that repeated pregnancy play a greater role in the etiology of infertility in Africa and Latin America, while repeated abortions are important in Asia and developing countries (16). In many cases in the developing countries, infertility in women results from untreated pelvic inflammatory disease (PID), a sequel of an sexually transmitted diseases (STDs) or other reproductive tract infections (2,15). The mean age of the male and female partners were 33±7 years and 29±6 years respectively which are almost similar to some other reports from national studies (11,12) and those from developing countries (15,17-19). The causes of infertility can be divided into four major categories: the female factor, the male factor, combined factors and unexplained infertility. In our study, male factor consists 38.9% of infertility, female factor occurred in 34.7% of the infertile couples, in 14.6% of the couples both partners involved and in 11.8% of couples no cause could be ascertained. In a field study in central part of Iran (Yazd province), Aflatoonian et al (2009) reported female factor as the main cause of infertility (57.7%) (8). On the contrary, in another study on infertile couples referred to Royan Institute in Tehran, male factor was found to be the most important etiologic factor (50.5%) (9). Different sampling and laboratory analytical methods may be attributable to these controversies. Most studies have reported a male factor in 20-40%, female factor in 30-55%, both couple involvement in 5-35% and undetermined cause in 5-15% (8, 11, 12, 19-24). However, the results of some studies are quite different, for example a study conducted in Western Siberia, found that male factors were responsible for infertility in 6.4%, and female factors were responsible in 52.7% of couples (25). While differences in data sources and analyses make it difficult to accurately measure or compare infertility rates, it is clear that the level and causes of infertility vary widely, both among and within countries (2). Approximately only 5% of the infertility incidence in couples is due to endocrinological, anatomical, genetic an immunological problems leaving about 95% of the infertility preventable. These preventable conditions, including: STD, parasitic diseases, health services and exposure to environmental toxic substances. (2).The factors that contribute to these conditions vary from region to region (2, 5, 9, 26, 27). The duration of infertility found in our study was longer (5.7±4 years) than that in developed countries (19), as well as some developing countries (19). It is however, similar to that in some other developing countries e.g. Indian Kashmir (17) and Iran (11, 12). Infertile couples do not usually present in time to the infertility clinics due to inadequate general knowledge regarding infertility and about the presence of special centers in the country. There are state owned as well as private general and special hospitals, but almost all of the medical doctors have private single special small clinic without any paraclinical facilities at the same place. These small private clinics are available to the patients without any waiting list and only by paying a visit charge of less than $15. They may (at least in some cases) offer advice or treatments without conducting a complete evaluation, sometimes even without seeing both partners. This situation makes the patients curious to try many such clinics especially when they do not obtain suitable results from the first prescription. This, in turn, makes a considerable confusion for the patients and a substantial delay before attending to an infertility clinic. Based on these data it is recommended to take measures to improve the referral system, fertility health education and implementing infertility prevention programs. Moreover, merging all those small private clinics into private, public or states owned hospitals is suggested, in order to assure timely, proper and adequate treatment. References
© Copyright 2011 - Iranian Journal of Reproductive Medicine The following images related to this document are available:Photo images[rm11004t1.jpg] [rm11004t2.jpg] |
| |||||||||

{kind=link}
{kind=link}