
|
International Journal of Reproductive BioMedicine
Research and Clinical Center for Infertility, Shahid Sadoughi University of Medical Sciences of Yazd
ISSN: 1680-6433 EISSN: 2008-2177
Vol. 9, Num. 2, 2011, pp. 135-140
|
Iranian Journal of Reproductive Medicine Vol. 9, No. 2, Spring 2011 , pp. 135-140
Case report
Unexplained infertility as primary presentation of celiac disease, a case report and literature review
Mohammadreza Ghadir1 M.D., Abolfazl Iranikhah1 M.D., Mahboubeh Jandaghi1 M.D., Farahnaz Joukar2 M.S., Massih Sedigh-Rahimabadi2 M.D., Fariborz Mansour-Ghanaei2 M.D.
- Department of Gastroenterology, Qom University of Medical Sciences, Qom, Iran.
- Gastrointestinal and Liver Diseases Research Center, Guilan University of Medical Sciences, Rasht, Iran.
Corresponding Author: Fariborz Mansour-Ghanaei; Gastrointestinal and Liver Diseases Research Center (GLDRC), Guilan University of Medical Sciences, Razi Hospital, Rasht, Iran. Email: ghanaei@gums.ac.ir
Received: 12 June 2010; accepted: 31 October 2010
Code Number: rm11022 Abstract:
Background: Celiac sprue (gluten sensitive enteropathy) is an autoimmune disease which is hereditary and its pathology mainly bases on immunologic intolerance to gluten. It has a vast variety of signs and symptoms and its clinical features range from a silent disease to a typical gastrointestinal disorder. In this study we reviewed and summarized some other related issues about this disease and its relation with infertility.
Case: The case is a 26 years old lady who had referred to a gynecologist because of infertility for 2 years and later it revealed that she has celiac sprue.
Conclusion: Screening for its silent or subtle types especially among suspicious cases such as unexplained infertility seems to be a cost effective action. Meanwhile, in time administration of a gluten-free diet can lead to an almost complete cure.
Key words: Celiac Disease, Infertility, Wight loss, Diarrhea.
Introduction
Celiac disease (CD) known as gluten sensitive enteropathy (GSE) is an autoimmune disease which presented by hypersensitivity reaction to the gliadin of wheat and barley in genetically prone individuals and has a prevalence rate around 1% in many developed countries (1-5). Celiac has a vast variety of manifestations which range from a typical malabsorption syndrome to a subclinical iron deficiency anemia (6, 7). The clinical tabloids of CD depend on its onset time, duration and severity (8).
Therefore, its classic presentation has an iceberg effect and each patient with CD has about 3 to 10 undetected signs or symptoms (4). Meanwhile, unlike to the traditional belief which classified CD as a digestive illness, it is a systemic disease that can occur in any time and in more than 50% of adult cases it has an atypical onset (9). There are several findings about impacts of CD on fertility among both sexes and some of these complications include; delayed menarche, menstrual discomforts, premature menopause, recurrent abortion and infertility )10-11(. Although overall prevalence of infertility is between 10- 15% and in 10- 15% of infertile women we cannot find any particular cause, CD as a risk factor of infertility and dramatic therapeutic response to gluten free diet justifying screening for this disease among unexplained infertile women (11).
Case report
The case is a 26 years old lady who had referred to a gynecologist because of infertility 2 years ago. She has married 8 years ago and after 2 years, she decided to have child. During the first two years of marriage they used natural method for contraception and she had not used any OCP or IUD. Her menarche was at the age of 14 and from then on she has a regular and normal monthly menstruation.
She had a negative past medical history with no sign or symptoms of neurologic diseases such as anxiety or depression. She had also no history of any clinical disease, pelvic or abdominal surgery, and extensive weight loss and drug or alcohol abuse. In her family history the only positive clues were; the presence of hypothyroidism, diabetes and vitiligo in her mother and aunts. In physical exams: BMI=23, secondary sexual signs were normal and there was no sign or symptom of hirsutism, acne or any other systemic disease. Evaluation of her husband revealed normal male factor and spermogram. Laboratory findings included: serum FSH, serum LH, serum prolactin, TSH, testosterone, progesterone and estradiol which all of them were at the normal range. Post coital test (PCT) and histrosalpangography were normal. Diagnostic laparoscopy showed no signs of tubal adhesion or endometriosis. After seven months and performing primary and secondary evaluation, she was diagnosed as a case of unexplained infertility and IVF was suggested for her.
About 9 months ago, the patient had a medical consultation because of diarrhea and 3 kg of weight loss. She reports a history of 12 months intermittent, non bloody and osmotic diarrhea which consists of normal bowel habits intervals. There was no history of fatty stool or consumption of laxatives.
Lab findings: HB: 11.8 (NL: 12-16) MCV: 76 (NL: 80-95)
MCH: 27 (NL: 36-48) Serum Fe: 110 (NL: 80-180) TIBC: 320 (NL: 250-460) Serum Ferritin: 54 ngr/ml
(12-300) CRP: +ESR: 18 S/E: negative
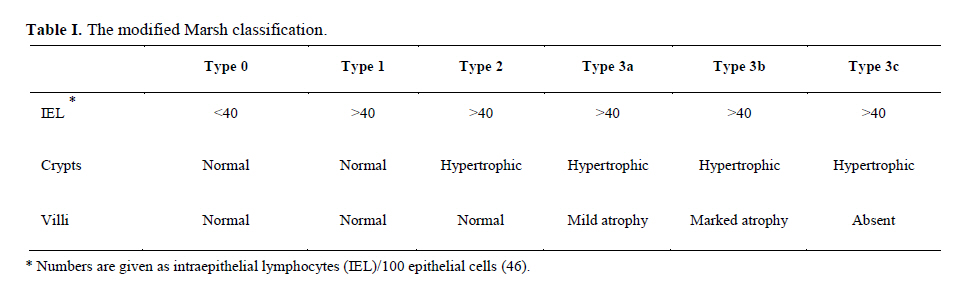
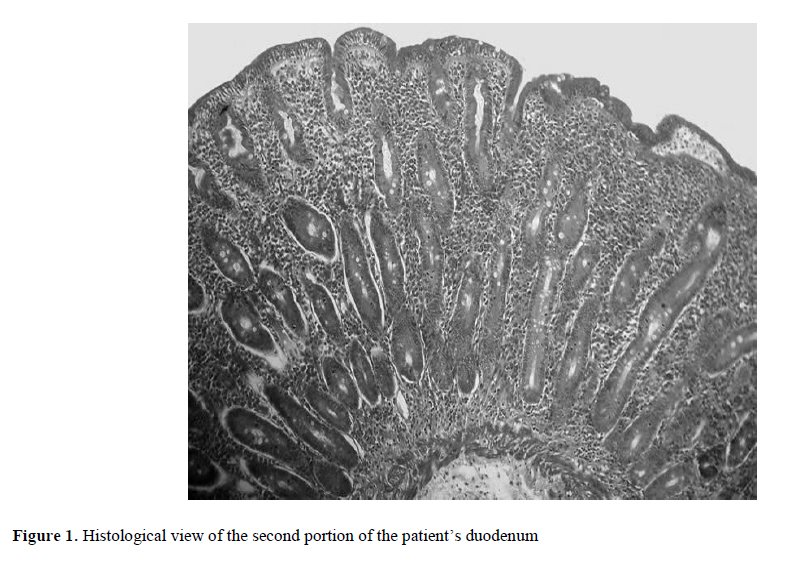
OB: negative. AST: 29 IU (NL: 5-40) ALT: 31 IU (NL: 8-40) Considering iron deficiency anemia, intestinal signs and the history of 4 years infertility, we became suspicious to celiac disease and checked serological factors (total IgA and tTG). The positive results of these tests (Total IgA>40 and tTG>30) followed by upper GI endoscopy and biopsy of the second portion of duodenum. The obtained tissues were observed by two expert pathologists and they reported severe malabsorption with flattening of villi, hyperplasia of crypts and total atrophy of mucosa which was presenting stage III of modified marsh classification (Table I and Figure I). Based on patient's history and serologic and pathologic findings diagnosis of CD was confirmed and she received a complete gluten free diet. After 3 months all her clinical features including; diarrhea, flatulence and anemia were eradicated and pregnancy occurred.
Discussion
Gluten sensitive enteropathy known as celiac disease (CD) or celiac sprue is an autoimmune disease with a prevalence of 1/270 in Finland to 1/5000 in North America (11). Manifestations of CD range from no symptoms to overt malabsorption with involvement of multiple organ systems and an increased risk of some malignancies (12). Some common and rare signs and symptoms of CD are shown in table II (3, 11, 13-20). Although CD has some classic clinical features which mainly consist of several gastrointestinal tabloids, its extra intestinal manifestations such as anemia and infertility need adequate attention and several studies put an emphasize on them. In many studies including Westerberg et al it is shown that CD prevalence rate is somehow more than estimations because of its silent and subtle types (21). In a study by Collin et al it is suggested that in unexplained infertility, silent celiac disease should be screened (22). Collin et al showed that the prevalence of CD among unexplained infertile cases (4.1%) is significantly higher than control group (0.0%) (p=0.02). Also, in this study it is shown that iron deficiency anemia is an important associated condition in patient with CD and unexplained infertility. Additionally, osteopenia and osteoporosis as common complications of CD (3, 23-26) put an especial importance on the time of diagnosis and treatment of suspicious cases.
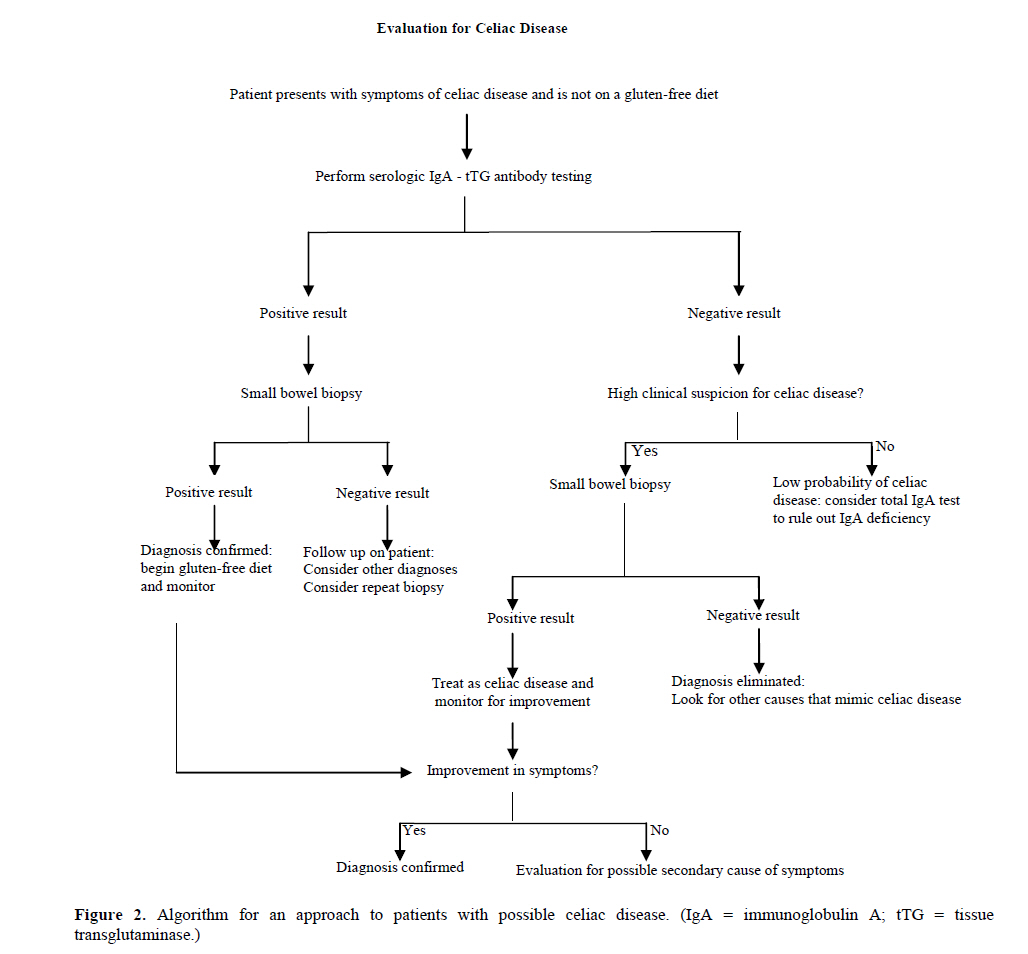
The diagnosis of CD is based on clinical suspicion plus positive serological tests and positive histological findings (11, 12, 21). The standard serologic tests which include IgA endomysial and tTG antibodies, according to many studies has a sensitivity and specificity of more than %95 (27-30). An algorithm for step by step approach to a suspicious patient with possible CD is shown in figure 2 (12). The important point is that serologic and biopsy samples should be taken before starting a gluten free diet (12, 31).
Finally all the authors believe that complete and lifelong gluten free diet is the only treatment of CD. Most of the dietary gluten is presented in wheat, rye and barely (12, 13, 21, 32-33). According to many studies, oat does not have gluten although its products are frequently contaminated with gluten (34-42). Like our case, in most of the studies, it is shown that all the complications of celiac patients can be completely cured by following a long life gluten-free diet (11-22, 43-46)
Conclusion
Screening for silent or subtle CD especially among suspicious cases such as unexplained infertility seems to be a cost effective action and in time administration of a gluten-free diet can lead to an almost complete cure.
References
- Fasano A, Catassi C. Current approaches to diagnosis and treatment of celiac disease: an evolving spectrum. Gastroenterology 2001; 120: 636-651.
- Rewers M. Epidemiology of celiac disease: what are the prevalence, incidence, and progression of celiac disease? Gastroenterology 2005; 128: 47-51.
- Fasano A, Berti I, Gerarduzzi T,
Not T ,
Colletti RB ,
Drago S , et al. Prevalence of celiac disease in at-risk and not-at-risk groups in the United States: a large multicenter study. Arch Intern Med 2003; 163: 286-292.
- Cronin CC, Shanahan F. Exploring the iceberg- the spectrum of celiac disease. Am J Gastroenterol 2003; 98: 518-520.
- Szaflarska-Szczepanik A, Czerwionka-Szaflarska M. The frequency of occurrence and clinical picture of celiac disease in the parents of children with the disease. Med Sci Monit 2001; 7: 971-976.
- United European Gastroenterology. When is a coeliac a coeliac? Report of a working group of the United Euro-pean Gastroenterology Week in Amsterdam. Eur J Gastroenterol Hepatol 2001; 13: 1123-1128.
- Troncone R, Bhatnagar S, Butzner D,
Cameron D ,
Hill I ,
Hoffenberg E , et al. Celiac disease and other immunologically mediated disorders of the gastrointestinal tract: Working Group report of the second World Congress of Pediatric Gastroenterology, Hepatology, and Nutrition.
J Pediatr Gastroenterol Nutr 2004; 39: 601-610.
- Pereira MA, Ortiz-Agostinho CL, Nishitokukado I,
Sato MN ,
Damião AO ,
Alencar ML , et al. Prevalence of celiac disease in an urban area of Brazil with predominantly European ancestry. World J Gastroenterol 2006; 12: 6546-6550.
- Makharia GK ,
Baba CS ,
Khadgawat R ,
Lal S ,
Tevatia MS ,
Madan K , et al. Celiac disease: variations of presentations in adults.
Indian J Gastroenterol
2007; 26: 162-166.
- Goddard CJ, Gillett HR. Complications of coeliac disease: are all patients at risk? Postgrad Med J 2006; 82: 705-712.
- Holtmeier W, Caspary WF. Celiac disease. Orphanet J Rare Dis 2006; 1: 3.
- Presutti RJ, Cangemi JR, Cassidy HD, Hill DA. Celiac Disease.
Am Fam Physician 2007; 76: 1795-1802.
- Ciclitira PJ,
King AL ,
Fraser JS . AGA technical review on celiac sprue. American Gastroenterological Association. Gastroenterology 2001; 120:1526-1540.
- AGA Institute. AGA Institute Medical Position Statement on the Diagnosis and Management of Celiac Disease. Gastroenterology 2006; 131:1977-1980.
- Sanders DS, Hurlstone DP, Stokes RO,
Rashid F ,
Milford-Ward A ,
Hadjivassiliou M , et al. Changing face of adult coeliac disease: experience of a single university hospital in South Yorkshire. Postgrad Med J 2002; 78: 31-33.
- Collin P. Should adults be screened for celiac disease? What are the benefits and harms of screening? Gastroenterology 2005; 128: 104-108.
- Green PH. The many faces of celiac disease: clinical presentation of celiac disease in the adult population. Gastroenterology 2005; 128: 74-78.
- Dewar DH, Ciclitira PJ. Clinical features and diagnosis of celiac disease. Gastroenterology 2005; 128: 19-24.
- Bodé S, Gudmand-Hoyer E. Symptoms and haematologic features in consecutive adult coeliac patients. Scand J Gastroenterol 1996; 31: 54-60.
- Farrell RJ, Kelly CP. Celiac sprue. N Engl J Med 2002, 346:180-188.
- Westerberg DP, Gill JM, Dave B, DiPrinzio MJ Quisel A, Foy A. New strategies for Diagnosis and Management of Celiac Disease. J Am Osteopath Assoc 2006; 106: 145-151.
- Collin P, Vilska S, Heinonen PK, Hällström O, Pikkarainen P. Infertility and coeliac disease. Gut 1996; 39: 382-384.
- McFarlane XA, Bhalla AK, Reeves DE, Morgan LM, Robertson DA. Osteoporosis in treated adult coeliac disease. Gut 1995; 36: 710-714.
- Kemppainen T, Kroger H, Janatuinen E,
Arnala I ,
Kosma VM ,
Pikkarainen P , et al. Osteoporosis in adult patients with celiac disease. Bone 1999; 24: 249-255.
- Collin P, Kaukinen K, Maki M. Clinical features of celiac disease today. Dig Dis 1999; 17: 100-106.
- Mustalahti K, Collin P, Sievanen H, Salmi J, Maki M. Osteopenia in patients with clinically silent coeliac disease warrants screening. Lancet 1999; 354: 744-745.
- Hill ID. What are the sensitivity and specificity of serologic tests for celiac disease? Do sensitivity and specificity vary in different populations? Gastroenterology 2005; 128: 25-32.
- Lewis NR, Scott BB. Systematic review: the use of serology to exclude or diagnose coeliac disease (a comparison of the endomysial and tissue transglutaminase antibody tests). Aliment Pharmacol Ther 2006; 24: 47-54.
- Maki M, Mustalahti K, Kokkonen J,
Kulmala P ,
Haapalahti M ,
Karttunen T , et al. Prevalence of Celiac disease among children in Finland. N Engl J Med 2003; 348: 2517-2524.
- Russo PA, Chartrand U, Seidman E. Comparative analysis of serologic screening tests for the initial diagnosis of celiac disease. Pediatrics 1999; 104: 75-78.
- Green PH, Jabri B. Coeliac disease. Lancet 2003; 362: 383-391.
- Marsh MN. Gluten, major histocompatibility complex, and the small intestine. A molecular and immunobiologic approach to the spectrum of gluten sensitivity (celiac sprue).
Gastroenterology 1992; 102: 330-354.
- Kasarda DD, Okita TW, Bernardin JE,
Baecker PA ,
Nimmo CC ,
Lew EJ , et al. Nucleic acid (cDNA) and amino acid sequences of alpha-type gliadins from wheat (Triticum aestivum). Proc Natl Acad Sci USA 1984; 81: 4712-4716.
- Shield J, Mullin MC. Patient Education Materials. Supplement to the Manual of Clinical Dietetics. 3rd Ed. Chicago; III: American Dietetic Association; 2001.
- Thompson T. Oats and the gluten-free diet. J Am Diet Assoc 2003; 103: 376-379.
- Lundin KE, Nilsen EM, Scott HG,
Løberg EM ,
Gjøen A , Bratlie J , et al. Oats induced villous atrophy in coeliac disease. Gut 2003; 52: 1649-1652.
- Hardman CM, Garioch JJ, Leonard JN,
Thomas HJ ,
Walker MM ,
Lortan JE , et al. Absence of toxicity of oats in patients with dermatitis herpetiformis. N Engl J Med 1997; 337: 1884-1887.
- Janatuinen EK, Pikkarainen PH, Kemppainen TA,
Kosma VM ,
Järvinen RM ,
Uusitupa MI , et al. A comparison of diets with and without oats in adults with celiac disease. N Engl J Med 1995; 333: 1033-1037.
- Janatuinen EK, Kemppainen TA, Pikkarainen PH,
Holm KH ,
Kosma VM ,
Uusitupa MI , et al. Lack of cellular and humoral immunological responses to oats in adults with coeliac disease. Gut 2000; 46: 327-331.
- Janatuinen EK, Kemppainen TA, Julkunen RJK,
Kosma VM ,
Mäki M ,
Heikkinen M , et al. No harm from five year ingestion of oats in coeliac disease. Gut 2002; 50: 332-335.
- Hogberg L, Laurin P, Falth-Magnusson K,
Grant C ,
Grodzinsky E ,
Jansson G , et al. Oats to children with newly diagnosed coeliac disease: a randomized double blind study. Gut 2004; 53: 649-654.
- Vader LW, de Ru A, van der Wal Y,
Kooy YM ,
Benckhuijsen W ,
Mearin ML , et al. Specificity of tissue transglutaminase explains cereal toxicity in celiac disease. J Exp Med 2002; 195: 643-649.
- Curione M, Barbato M, Viola F, Francia P, De Biase L, Cucchiara S. Idiopathic dilated cardiomyopathy associated with coeliac disease: the effect of a gluten-free diet on cardiac performance. Dig Liver Dis 2002; 34: 866-869.
- Shahbazkhani B, Forootan M, Merat S,
Akbari MR ,
Nasserimoghadam S ,
Vahedi H , et al. Coeliac disease presenting with symptoms of irritable bowel syndrome. Aliment Pharmacol Ther 2003; 18: 231-235.
- Patwari AK, Anand VK, Kapur G, Narayan S. Clinical and nutritional profile of children with celiac disease. Indian Pediatr 2003; 40: 337-342.
- Volta U, De Franceschi L, Lari F, Molinaro N, Zoli M, Bianchi FB. Coeliac disease hidden by cryptogenic hypertransaminasaemia. Lancet 1998; 352: 26-29.
- Oberhuber G, Granditsch G, Vogelsang H. The histopathology of coeliac disease: time for a standardized report scheme for pathologists. Eur J Gastroenterol Hepatol 1999; 11: 1185-1194.
© Copyright 2011 - Iranian Journal of Reproductive Medicine
The following images related to this document are available:
Photo images
[rm11022t2.jpg]
[rm11022t1.jpg]
[rm11022f2.jpg]
[rm11022f1.jpg]
|

{kind=link}
{kind=link}
{kind=link}