 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Exposure to Inhalable Flour Dust and Respiratory Symptoms of Workers in a Flour Mill in Iran *H Kakooei1 and H Marioryad 2 1Dept. of Occupational Health, School of Public Health, Tehran University of Medical Sciences, Iran2School of Environmental Health, Yasuj University of Medical Sciences, Iran *Corresponding author: E-mail: hkakooei@sina.tums.ac.ir Tel: +98 21 66461334, Fax: +98 21 66462267 Code Number: se05008 ABSTRACTIn 1999 the American conference of governmental industrial hygienists (ACGIH) proposed a threshold limit value (TLV) of 0.5 mg/m3 for flour dust with a sensitization notation. As part of this study, a relationship between flour dust concentrations and respiratory symptoms were examined. All 24 male flour subjects and 10 male controls were studied using air samples, ventilatory function testing, and questionnaire on respiratory symptoms. On average, breathing zone respirable and total flour dust in the flour mill were 4.97 mg/m3 and 12.11 mg/m3, respectively. The prevalence of cough, phlegm, difficulty to breathe, and respiratory symptoms were higher in subject group, also during an 8-h shift ventilatory function tests, it was demonstrated that respiratory capacities (FVC, FEV1, PEF) in the flour workers decreased, however, there was no significant statistical difference between case and control groups. Our results suggest that all of different job activities in flour mill may have a great impact on the development of work- related symptoms. Therefore, to minimize the risk of sensitization of occupational exposure during the work process, along with a decrease in mean 8-h TLV average exposure should be achieved. Keywords: Flour mill workers, Flour dust, Respiratory symptom, Respiratory capacity INTRODUCTIONThe American Conference of Governmental Industrial Hygienists (ACGIH) defines flour as a complex organic dust consisting of wheat, rye, millet, barely, oats or corn cereal, or a com- bination of these, which have been processed or ground by milling (Karpinski, 2003). Inhalation of flour dust can produce allergic reaction and chronic respiratory disorders, including sensitization and asthma (Fakhari, 1992; Massin et al., 1995; Smith and lumlely, 1996; Taylard et al., 1998; Smith and Patton, 1999). Epidemiological studies focusing on exposure-response relationships, as well as personal exposure to inhalable flour dust, wheat, and α-amylase allergens in flour mills and bakeries have been analyzed by several authors (Burdof et al., 1994; Houba et al., 1998). In 1999, the ACGIH proposed a TLV of 0.5 mg/ m3 for flour dust with a sensitization notation. In some Canadian provinces, flour dust with the exposure limit of 10 mg/m3 total dust, and 5mg/m3 for respirable dust, respectively has been established (Karpinski, 2003). In Germany and Denmark, specific occupational exposure limits for flour dust have been set at 4 and 3 mg/m3, respectively. Nordic countries, including Finland, Iceland, and Norway, have set their exposure limit at 5 mg/m3 for organic dust (Karpinski, 2003). The health and safety commission of the United Kingdom has established an 8-h TWA maximum exposure limit of 10 mg/m3 for flour dust, with a 15-min exposure limit of 30 mg/m3 (Fakhari, 1992; cullinan, 2001). Flour dust is a hazardous substance with respirtory sensitizing with pre- existing disease and also causes chronic bronchitis (Smith and Lumley, 1996). In occupational respiratory disease, spirometry is one of the most important diagnostic tools (Taylard et al., 1998). It is the most widely used, most basic effort dependent pulmonary function test (PFT) and can measure the effects of restriction or obstruction on lung function (Fouad et al., 1995). The present study was initiated to determine the relevance of occupational exposure to flour dust in a flour mill and the respiratory symptoms as well as lung function during the work shift in total of workers with considerable exposure. MATERIALS AND METHODSThis study was conducted in a flour mill located in Yasuj, the center of south-west province of Iran. In this mill, the grain is delivered in bulk and held in elevators prior to use. Before grinding, the wheat is inspected, classified, cleaned of impurities, and tempered with water to soften or mellow endosperm. Different types of wheat are then blended to make specific flour. The final steps involve bleaching and enriching the flour. The final product in powder form is bagged and supplied for home and bakery uses or is delivered in bulk by truck to bakeries. All available male employees of the flour mill were invited to participate as study subjects. Twenty four flour mill workers as full-time employees were selected. To insure coverage of all possible duration of exposure, it was decided to include workers with five years or more experience. The results obtained in the group of workers were compared with 10 employees who worked in the office and laboratory as control subjects. This study was carried out in 2 stages as follows:
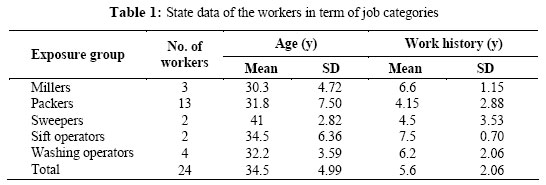
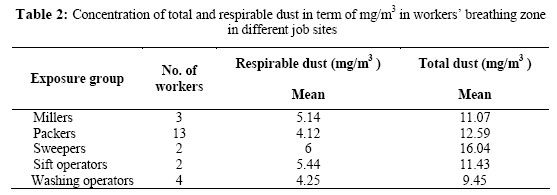
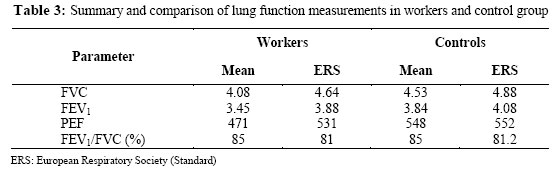
Four different job activities were selected in the flour mill. Total and respirable dusts were collected from following sites: Millers, pckers, sweepers and operators. Total dust samples were collected using a 0.5 µm pore size and 37mm diameter P.V.C filter attached to closedface 37-mm cassette at flow rate 2 l/ min (MSA. Model 2G- 2867 and DESAGA. GS312). Respirable dust samples were collected using a 10 mm cyclone at a flow rate of 1.7 1/min. The mass of dust in all samples were weighed to 0.0001 g on a calibrated sartorious balance before and after sampling. In order to obtain precise results, all filters were allowed to equilibrate in desiccator’s atmosphere for 24h prior to weighing. A minimum of one blank filter cassette assembly for every 10 samples was provided to determine a correction to the final weight of the samples. Personal samples were collected during full-shift periods of 8 and 12 h depending on the employee being sampled. The samples were analyzed gravimetrically. Respiratory symptoms and ventilator function were conducted before entering the workplace and at the beginning of the shift. The participants were directed to a test room isolated from the work area. Subjects were interviewed using a respiratory questionnaire to record personal characteristics, medical and occupational history. For each subject, forced vital capacity (FVC), forced expiratory volume in 1 sec (FEV 1), FEV1/ FVC, and peak expiratory flow (PEF), were obtained using the spirometer. The ventilator function parameter was measured five times, and an average of three best results was calculated and connected to body temperature and pressure saturated with water vapor. The tests were performed with a nose clip and with the subject in the sitting position. RESULTSThe state data of workers in term of job categories are shown in Table 1. The results of 36 samples of flour dust are presented in Table 2. With regard to the finding, the workers who worked in sweep process had the highest exposure to total dust and respirable dust, i.e.16.04 and 6 mg/m3, respectively. While the wheat operators had the lowest exposure for above mentioned order as 9.45 and 4.25 mg/m3, respectively. The results gained from evaluation of the workers’ respiratory symptoms are shown in Fig. 1. In this case, χ2-test showed the mean value of respiratory symptoms to be higher among workers than the control group. But these difference only in the morning humor problem were significant (P<0.02). Table 3 summarizes the comparison of the lung function parameters for flour mill workers and control groups, in comparison with ERS (European Respiratory Society) standards. The results showed that respiratory function parameters in the workers group are decreased, although there was no significant statistical difference. DISCUSSIONThis study was performed in a flour mill with typical occupational health problems. During the course of the study, the work stations were generally filled with visible dust. The mean concentration of the worker ’s respiratory zone air at different exposure group was more than TLV-TWA, i.e. 0.5 mg/m3, recommended by American Conference of Governmental Industrial Hygienists ACGIH. Therefore, the emission sources of the particulate should be of the most special attentions and needed to be highly controlled by means of using more powerful ventilation systems either generally or locally as well as a continuous environmental monitoring of the emitted flour dust. Air sampling showed that in the operator ’s work station, the concentration of 80% of total flour dust samples exceeded the threshold limit value (TLV) of 0.5 mg/m3 recommended for respirable dust by ACGIH. The concentrations of the total dust collected at each exposure group by personal sampling were about two times higher than those taken by respirable sampling. As the results showed, the sweepers were exposed to the highest concentration of respiable dust (6mg/m3) while the wheat washing operator had the lowest exposure (4.25 mg/m3). In one of the British studies cited in risk assessment document for flour dust prepared by the health and safety executive, it was found that 20 percent of mill workers were exposed to the levels of inhalable flour dust exceeding 10 mg/m3 (Karpinski, 2003). Congruent with many studies (Duke, 1935; Cullinum et al., 2001; Smith et al., 2001; Karpinski, 2003), this study confirms that flour mill workers have a higher prevalence of respiratory symptoms than unexposed control subjects. However, the prevalence of respiratory symptoms in this study was generally lower than that of other studies (Musk et al., 1990; Karpinski, 2003; Meo, 2004). Schwartz et al., (1995), reported that grain mill workers had significantly reduced spirometric measures of air flow FEV1, FEV1/FVC, and FEF25-75%. MEO, (2004) found a significant decrease in the mean values of FVC, FEV1, PEP and MVV; this impairment increased with duration of exposure in the flour mills. In this study, there are no significant differences between the ventilatory function test results of the flour mill workers and control subjects. This is contrary to the results obtained by Karpinski, (2003), MEO (2004), who observed that flour workers had a significantly lower mean FVC and FEV1 than controls. Karpinski, (2003) reported that 101 employees (97.1%) were exposed to levels and exceeding 0.5 mg/m3, 66 (67.3%) to levels exceeding 5 mg/m3, and 44 (42.3%) to levels exceeding 10 mg/m3. Bulat et al., (2004) observed that in traditional bakeries among bread and pastry workers were exposed levels (geometric mean 2.10 mg/m3 and 1.80 mg/m3), respectively. The most important finding of this study was that some of these values (total dust) were more than 33 times higher than the TLV recently proposed by ACGIH (0.5 mg/m3). The present study confirms the finding of others and suggests that flour dust adversely affects lung function parameters, such as FVC, FEV1, PEF and causes an obstructive pattern of lung function impairment which is associated with the dose- effect of years of exposure to flour dust. The respiratory functions test in workers and control groups indicated that respiratory capacities in workers decreased; however there was no significant statistical difference. These measures will help to prevent lung damage, which often, overtime contributes to morbidity and mortality. It is also suggested that flour workers must undergo pre-employment and periodic medical surveillance tests. Improvement in housekeeping and the ventilation system to reduce air contaminant levels are strongly suggested. The use of personal protective equipment is also recommended to provide additional protection. ACKNOWLEDGEMENTSThe authors are grateful to M Lahmi, MD, for his medical support. The authors also thank the workers for their participation. REFERENCES
© Tehran University of Medical Sciences Publications 2005 |

{kind=link}
{kind=link}
{kind=link}