 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
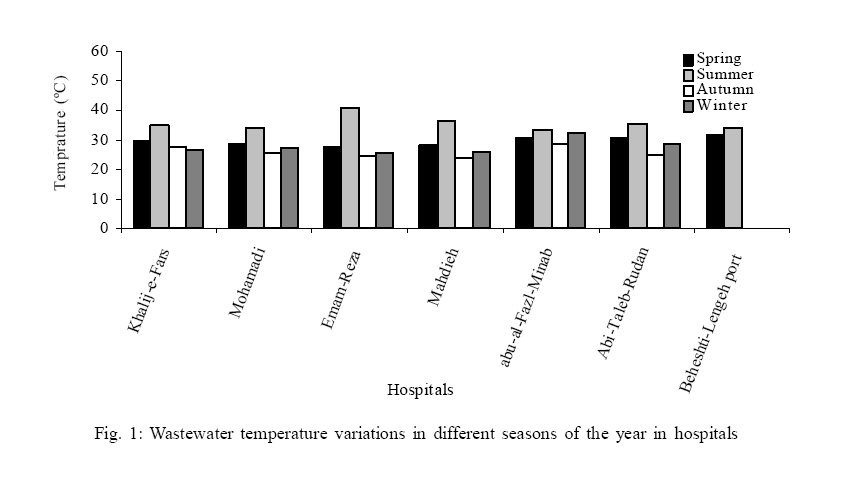
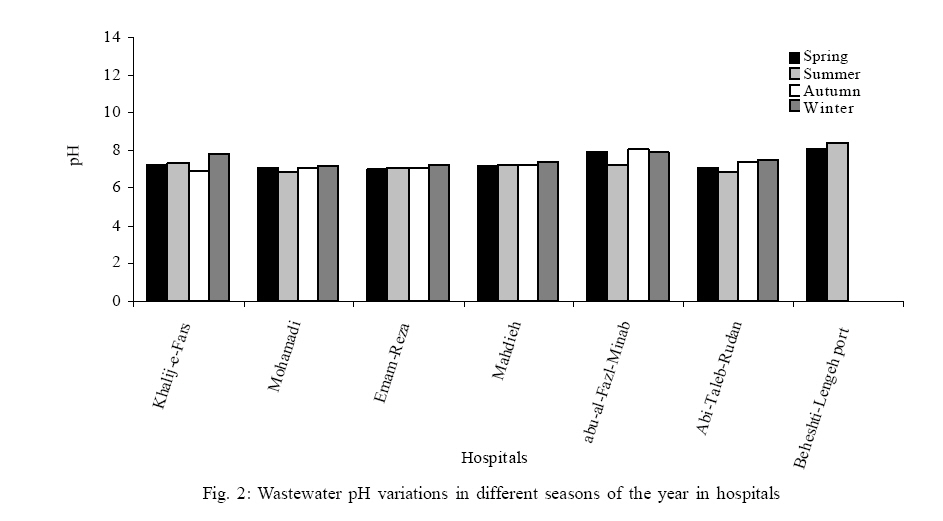
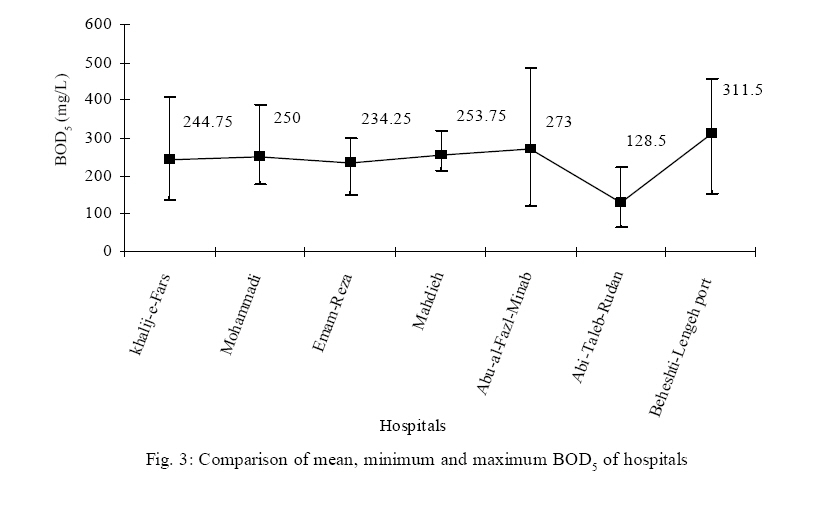
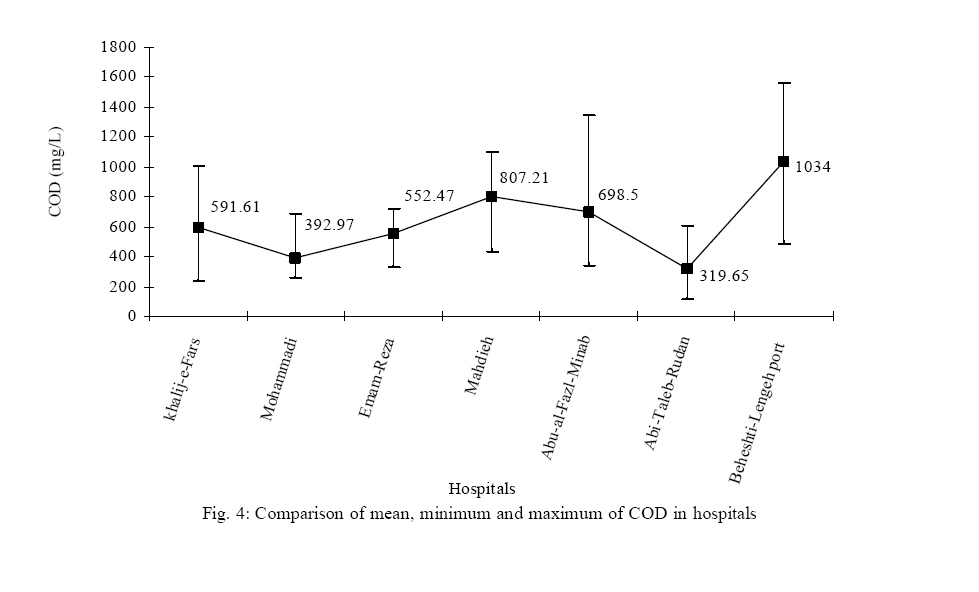
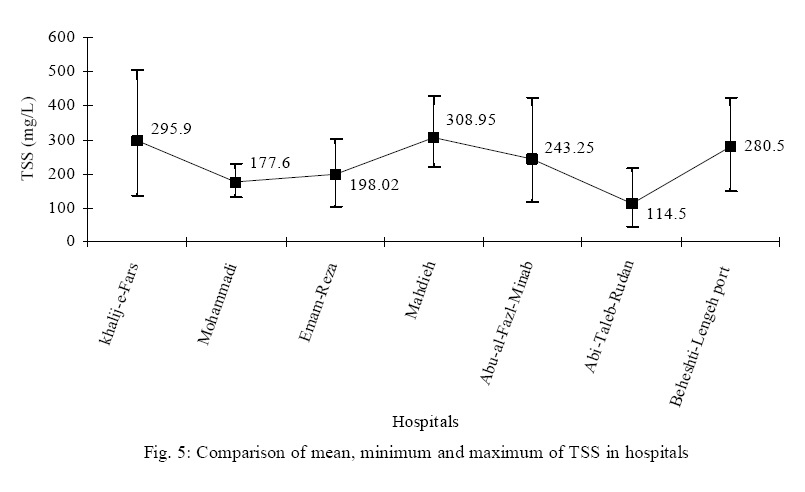
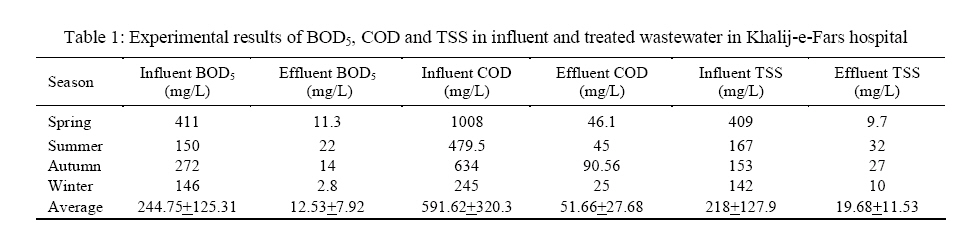
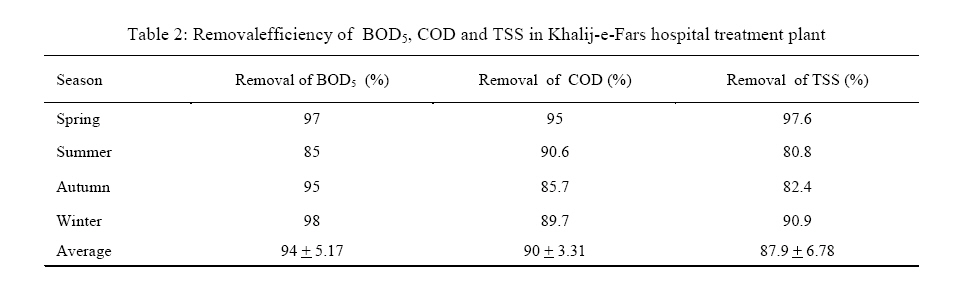
Iranian Journal of Environmental Health Science & Engineering,Vol. 4, No. 1, 2007, pp. 43-50 QUALITY AND QUANTITY SURVEY OF HOSPITAL WASTEWATERS IN HORMOZGAN PROVINCE *1 Sh. Sarafraz, 2M. R. Khani, 3K. Yaghmaeian 1Department of the Environmental Engineering, Islamic Azad University, Bandar Abass Branch, Bandar Abass, Iran *Corresponding author-Email: sarafraz_sh@yahoo.com Telefax: +98 21 6695 4227 Received 2 October 2006; revised 18 November 2006; accepted 29 December 2006 Code Number: se07007 ABSTRACT Hospital wastewaters are one of the most contaminating wastewaters and need to be paid more attention due to containing infectious agents. In this study, which had been conducted in a period of one year, 7 public hospitals were selected out of 12 public hospitals in Hormozgan Province of Iran. For studying quality of wastewater in hospitals, both influent and effluent wastewaters of treatment plant, if any, were sampled once in each season and totally 30 mixed samples were obtained. In order to determine the quality of hospital wastewaters in all samples, parameters such as pH, BOD5, COD, TSS and temperature were measured. Results of investigation on annual water consumption indicated that average water consumption in hospitals of the province was 194m3/d., considering water-to-wastewater conversion ratio of 0.8 and green yard ratio of 0.3. Wastewater production rate had been estimated to be 47m3/d and 0.362 m3/d.bed. Results indicated that in 7 hospitals of Hormozgan province, mean values of BOD5 ,COD ,TSS in raw wastewater were 242.25 mg/L, 628.1 mg/L and 231.25 mg/L, respectively, pH=7.42 and temperature=30.17 ºC. In Khalij-e-Fars hospital which had wastewater treatment plant, values of these parameters in effluent were 12.53 mg/L and 51.7 mg/L, 19.68 mg/L, respectively, with pH=7.39 and temperature=26.1 ºC. Comparison between values of influent and effluent wastewaters indicated that in understudy cases, contamination rate was higher than determined limits, as compared to environmental standards of the country and it was necessary to establish appropriate treatment plants in these units. Key words: Hospital wastewaters, quantity and qualitaty parameters, wastewater treatment, Hormozgan. INTRODUCTION Nowadays in many societies, access to healthy water and the amount of water consumption are considered as aspects of sanitation situation and development of societies. The consumed water in daily life is recycled to primary source in some ways, but it is in the form of a liquid containing the consumed water and different contaminants that are entered during consumption. One of the important environmental problems which are increased by population growth is the spread of wastewater contaminants, for example hospital wastewater which results in surface and underground water contaminations. Specifications of hospital wastewaters, have made these kind of wastewaters special in environmental contaminations control issue(Jolibois and Guerbet, 2005). Hormozgan province, located in south part of the country has two climates: One of them is mountain region that has semi moderate climate and other areas located in hot and dry climates. In general, Hormozgan province is affected by the desert climate and has got long and hot summers and short and moderate winters (Anonymous, 2005). The consumed water of province's hospitals is supplied through public network which is followed by hospital wastewater production. In wastewater classification, hospital wastewaters are considered as domestic wastewaters class, but their specifications are somehow different with domestic wastewaters as the amount and variety of hospital wastewaters are more than domestic wastewaters. Quality and quantity of wastewater produced in every hospital depends on different factors. Some of these factors are: bed number, accessibility to water, kind of services, number of units, climate situation, people's culture and geographical situation which result in variety of hospital wastewater production and defines that necessary treatments should be carried-out on them before their entrance into urban wastewater network (Sabzali and Shivaii, 2006). Because of potentially dangerous materials contained in hospital and care-center wastewaters, such as heavy metals, different detergents, solvents, microbiological pathogens, toxic organic, mineral chemical materials, pharmaceutical compounds such as antibiotics, hormones, arasthetic agents, cytotoxocological compounds and radioactive isotopes, It is necessary to be investigated (Pruss et al., 1999). Concentration of bacteria flora from 2.4× 103/100 mL to 3×105/100 mL are deducted for hospital effluent. These concentrations are lower than that of the 108/100 mL generally present in the municipal sewage system was deducted for hospital wastewater. Marker of viral pollution such as enter virus and other viruses such adenovirus, has identified in hospital effluents. Besides, the HIV, causal agent of the AIDS also represents in hospital wastewaters (Emmanuel et al., 2002). Results from Germany presented show that the concentration of platinum from hospitals from platinum containing anti-neoplastics if of only minor importance compared to other inputs. Compared to platinum emissions from other sources the effluents of hospitals are not the most important ones, but they should not be disregarded (Kummerer and Helmers, 1997). In the recent years the emphasis was on so-called emerging contaminants including pharmaceuticals such as antibiotics, endocrine disruptors (e.g. steroid hormones, nonylphenol, bisphenol A) and on various additives such as hardeners in foundry sands. Environmental analytical studies show that trace concentrations of antibacterial agents (antibiotics) occur in hospital and municipal wastewaters and in the aquatic environment (Gigar et al., 2003). Antibiotics are an important group of pharmaceuticals in today's medicine. Yet, there is still no comprehensive data about the occurrence of antibiotics. Reports show that the amount of antibiotics emitted, by some European hospital effluents, in total correspond to mean antibiotics concentration in municipal wastewater approaching 50 µg/L. Antibiotic residues in environment are suspected to induce resistance in bacteria strains causing a serious threat for public health (Emmanuel et al., 2002). Enterococci have been involved in nosocomail infections and the spreading of antibiotic resistance through the food chain. The species distribution of enterococci and the presence of resistant strains to vancomycin and erythromycin were analyzed in more than 400 raw and treated urban wastewaters, surface waters receiving these treated wastewaters and hospital wastewaters from some of the European countries. It appears that these bacteria could pass through wastewater treatment plants and be transferred to surface waters (Blanch et al., 2003). Investigations carried-out in Swiss Federal Inc, show that the fluoroquinolones ciprofloxacin and norofloxacin are substantially eliminated in wastewater treatment (80-90%) by sorption transfer to sewage sludge (Gigar et al., 2003). Mean while, concentration of ciprofloxacin in hospital sewages is in the range of 3-84 µg/L which correlated strongly with ciprofloxacin concentration in a logistic dose-dependent manner (Sabzali and Shivaii, 2006; Hartmann et al., 1999). Hospitals represent an incontestable release source of many chemicals compounds in their wastewaters, and which may have an impact on the environment and human health, some of the substances found in wastewaters are genotoxicological and are suspected to be a possible cause of the cancer observed in the last decades (Jolibois and Guerbet, 2005). MATERIALS AND METHODS In this investigation, after librarian studies, sampling from influent and treated wastewaters was conducted at understudy units. Due to lack of appropriate treatment system and wastewater discharge evaluation, to estimate the produced wastewater quantity, the water consumption for one year was defined by issued receipts. To define quality parameter, sampling from out coming sewages was conducted, and the samples were delivered to laboratory for measurements. The investigation periods were 12 months and 7 hospitals but of totally 16 hospitals, available in the province, were selected. Sampling was carried out from 4 hospitals located in province center (Abass-port) and 3 hospitals located in dependent cities. These hospitals are called: Khalij-e-Fars, Mohammadi, Emam-Reza, Mahdieh (these are in Abass-port), Abul-al-Fazl-Minab, Abi-Taleb- Rudan and Beheshti- Lenge port. Public hospitals, since the have different care units, contained variety of contaminants, so 7 out of totally 12 public hospitals available in the province (about 60% of units) have been studied. Samples were then mixed and pH, BOD5, COD, TSS parameters and temperature were tested for each sample. All experiments were carried out on the basis of "standard methods of water and wastewater tests"(APHA, 1998), Because of working limitations of sterilization plant in the laboratory, totally 30 samples were taken and 150 tests were conducted. Analysis of the data and approaches were done by SPSS and Excel software. RESULTS Investigation of annual water consumption shows that the average daily water consumption of province hospitals is 194 m3/d which is equal to 0.362 m3/d.bed. Quantitative amount of daily wastewater production, considering water to wastewater conversion coefficient of 0.8 and green yard ratio of 0.3 was estimated 47 m3/d.bed understudy unit. Qualitatively, as mentioned before, testing of pH, BOD5, COD, TSS and temperature were carriedout and the results are as follow: Due to Fig. 1, which represents the investigation approaches on temperature, minimum temperature was 23.9 ºC, maximum temperature was 40.6 ºC and average annual temperature during the investigation period was measured as 30.17 + 1.53 ºC. Investigation approaches on pH and its variations in the measured samples show that minimum pH was 6.82, maximum pH was 8.38 and annual average pH was measured as 7.42 + 0.42 (Fig. 2). Investigation approaches on BOD5 evaluations, as an important parameter in organic load evaluation, show that minimum BOD5 was 70 mg/L, maximum BOD5 was equal 485 mg/L and the annual average of BOD5 was 242.25 + 56.2 mg/L (Fig. 3). COD measurements show that COD is varied between 124.4 - 1560 mg/L and the annual average of COD was estimated as 628.1+ 244.7 mg/L (Fig. 4). Approaches on TSS show that it varied between 47 479.5 mg/L and the annual average of TSS was measured as 231.25 + 71.18 mg/L (Fig. 5). Since wastewater treatment system was only available in one hospital (Khalij-e-Fars hospital), BOD5, COD and TSS parameters were measured in raw wastewater and treated sewage as well, which their measurement results are shown in Table 1. In Table 2 the efficiency of above parameters decrease (in percent) in one hospital of the province is shown. DISCUSSION Results of this study showed that the average temperature of hospitals wastewater was 30.17 °C. By the increase of temperature, reactions velocity and bacterial activity for biological degradation of degradable materials are increased 2-3 times per 10 °C (about 50 °C). On the other hand, temperature increases for aerobic biological degradation of organic material of wastewater by the bacteria is followed by more oxygen consumption and soluble oxygen demand which is increased. Since temperature has a diverse relation with DO concentration in distilled water without Cl- lower in partial pressure (760 mmHg), DO amount is decreased. This renges are 0 °C equal to 14.6 mg/L and in 30 °C equal to 7.54 mg/L (Metcalf and Eddy, 2004). Due to client situation of hospitals in Hormozgan province and mean wastewater temperature of 30.17 °C, which reached up to 40.6 °C, it should be considered that oxygen supply required for hospital's wastewater treatment by aerobic methods such as activated sludge is followed by more problems and appropriate development of this system was required. One of the important parameters in biological treatment of hospital wastewater is pH and its variations. Generally, optimum pH for growth and activity of bacteria varies between 6.5-8.5 and most of the bacteria which play main role in wastewater treatment, do not tolerate pH over 9.5(Metcalf and Eddy,2004). In this investigation, the mean measured pH was 7.42 which were appropriate. Depending on pH, the three substances exhibited considerably different adsorption rates in wastewaters. At pH=7, cisplatin was adsorbed by 88%, whereas only 26% of carboplatin and 54% of oxaliplatin were removed. Adsorption by activated sludge was higher, less affected by pH variation and comparable for all investigated CPC (96% for cisplatin,70% for carboplatin and 74 % for oxaliplatin at pH=6.8), whereas activated sludge showed more consistent elimination rates (average values: cisplatin 92%, carboplatin 72% and oxaliplatin 78%) (Lenz et al., 2005). Also, at pH=8, are used chlorides as indicators of hospital wastewater toxicity on daphnia (Emmanuel et al., 2002). The pH effluent standard of the country for evacuation to surface water is 6.5-8.5, for discharging in to absorbent wells is 5-9 and for agricultural application is 6-8.5 (Anonymous, 2000). Variations related to BOD5, had an annual average of 242.25 mg/L. Effluent standards of BOD5 for discharging in to absorbent well and surface waters is 50 mg/L and 100 mg/L in agricultural consumptions. (Metcalf and Eddy, 2004). BOD5 of hospital wastewater are sometimes estimats up to 700 mg/L but it is estimated 603 mg/L for hospital wastewater and 220 mg/L for urban wastewater on average (Emmanuel, 2002). This means that, treatment systems for these kinds of wastewaters should be considered to establish 90% of treatment. For example in Khalij-e-Fars hospital by regarding influent and effluent amounts of treatment plants, 99% efficiency of BOD5 removal which corresponded with standards of discharge to absorbent wells, surface and agricultural wastewaters. While in other hospitals (without treatment plant) in order to reach the standards of discharge to urban network, 80-90% of the treatment should be established. Variations related to COD in hospitals had an average amount of 628.1 mg/L; standard of effluent COD for in dicharge in to surface waters and absorbent wells is 60 mg/L and 100 mg/L and 200 mg/L in agricultural applications (Anonymous, 2000). Based on the standards, which in the hospitalsdid not have treatment plant, COD of the effluents were high, which showed that contaminants were entering into the environments through these units. While in Khalij-e-Fars hospital the efficiency of COD removal was 90% which corresponded with the standards of discharge in to absorbent wells, surface and agricultural waters. Results from a hospital in Nepal has shown that serial operation of two-stage constructed wetland for treating wastewater had strong correlation with the hydraulic loading and the COD influent concentration (Laber et al., 1999). Results of this investigation showed that effluent of TSS in understudy units was very high, 4-6 times of standard amount of wastewater evacuation to environment. While only in Khalij-e-Fars hospital which had wastewater treatment plant, comparing the amount of influent and effluent of the plant, showed a 87.9% efficiency in TSS elimination, which corresponded with available standards. ACKNOWLEDGEMENTS Hereby it is acknowledged for the support of the manager and the staff of Department of Environment of Hormozgan Province, specially Mr. Shamsipour and Mr. Fadakar, Ms. Heidari and Mrs. Salimzadeh who helped in sampling and measuring experiments. REFERENCES
© 2007 Tehran University of Medical Sciences Publications The following images related to this document are available:Photo images[se07007f3.jpg] [se07007f4.jpg] [se07007f2.jpg] [se07007f5.jpg] [se07007t1.jpg] [se07007t2.jpg] [se07007f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}