 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
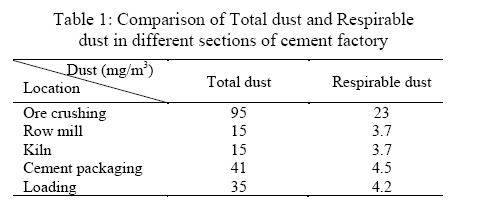
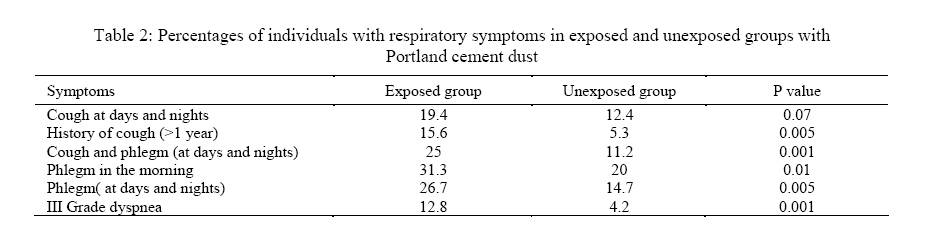
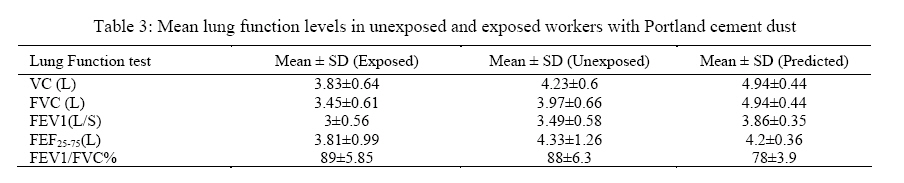
Iranian Journal of Environmental Health Science & Engineering, 2008, Vol. 5, No. 3, pp. 201-206 Effects of Exposure to Portland Cement Dust on Lung Function in Portland Cement Factory Workers in Khash, Iran 1 R. Mirzaee, *2 A. Kebriaei, 3 S. R. Hashemi, 1 M. Sadeghi, 4 M. Shahrakipour 1 Department of Occupational Hygiene, School of Health, Zahedan University of Medical Sciences, Zahedan, Iran Received 15 September 2007; revised 22 December 2007; accepted 10 May 2008 Code Number: se08034 ABSTRACT The present study was done to assess cement dust exposure and its relationship to respiratory health effects, both acute and chronic respiratory symptoms and ventilatory function impairment among Portland cement factory workers in Khash located in the south part of Iran. A cross-sectional study was conducted at Khash Portland cement producing factory in Iran in 2001. A total of 170 exposed and 170 unexposed employees were selected. Air transmitted personal respirable dust and total dust samples were collected in a full-time (8h/day) shift. Dust level was determined by the gravimetric method. An interviewer-administered questionnaire was used to collect information and history of respiratory health among workers (exposed and unexposed to dust) and measurements of lung function were made using a spirometer in both groups. Concentrations of personal respirable dust ranged from 3.7 mg/m3 in the kilns to 23 mg/m3 in the ore crushing area, and total dust ranged from 15 mg/m3 in the kilns to 95 mg/m3. Cough and phlegm, with or without shortness of breath, were significantly related to dust concentration. Measuring pulmonary functions of workers exposed to dust and unexposed group showed a significant decrease in vital capacity, forced vital capacity, FEF25-75 and Forced Expiratory Volume in the first second (P<0.05). Findings suggest that occupational exposure to Portland cement dust may lead to higher prevalence of respiratory symptoms and the reduction of ventilator capacity due to existence of quartz in row material of cement dusts. The study revealed that cement dust exposure is associated with acute as well as chronic respiratory health effects. It is recommended that engineering measures must be taken to reduce the dust level in cement factories, accompanied with health monitoring of exposed employees. Key words: Cement, respiratory symptoms, lung function, dust, Portland cement INTRODUCTION Portland cement is a light grey powder produced by crushing and grinding calcareous materials such as limestone, chalk and argillaceous materials such as; clay and shale, as a wet slurry or in a dry state. The mixture is calcined in a rotary kiln and the resulting clinker is finely ground. The product is composed largely of calcium silicates, calcium aluminates, calcium sulfates, oxides of sodium and potassium and calcium-alumino-iron compounds (Burgess, 1981). Other constituents are then added, depending on the desired concrete properties. Hexavalent chromium may also be present in the cement. Exposure to Portland cement dust has long been associated with the prevalence of respiratory symptoms and varying degrees of airway obstruction in man. Apart from respiratory diseases, it was also found to be a cause of lung and laryngeal cancer, gastrointestinal tumors and dermatitis (Vestbo and Rasmussen, 1990; Rasmussen et al., 1990; Jakobsson et al., 1993; Yang et al., 1996; AbuDhaise et al., 1997; Noor et al., 2000; Algranti et al., 2001; Al-Neaimi et al., 2001; Laraqui et al., 2001; Stern et al., 2001). Exposure to cement dust is likely to vary in the different stages of the production process (ILO, 1999; Alvear-Galindo et al., 1999). Workers who are in close contact with the production processes have been reported to have high exposure to total dust (11-230 mg/m3) and respirable dust (2-46 mg/m3) (Abrons et al., 1988). Respirable particulate mass consist of those particles with a median aerodynamic diameter of 3.5µm±0.3µm (Hering, 1989). However, most studies have been done in developed countries in recent years (Abrons et al., 1988; Rasmussen et al., 1990; Fell et al., 2003) show indications of improved dust control compared to studies in developing countries. Portland cement dust irritates the mucous membranes of the respiratory airways (ILO, 1999), which might lead to acute post shift reductions in Peak Expiratory Flow (PEF) (Mengesha and Bekele, 1997) and FEV1 (Ali et al., 1998) among exposed workers. Repeated and prolonged inhalation of cement dust is associated with chronic respiratory symptoms (Yang et al., 1996; Al-Neaimi et al., 2001) and impairment of lung function (Yang et al., 1996; Noor et al., 2000; and Oleru 1984). Toxic effects of air-borne pollutants on humans include damage to eyes, respiratory and nervous systems, and a number of teratogenic, carcinogenic and mutagenic effects (Fatima et al., 1974). In spite of the fact that pneumoconiosis was the oldest and best known of the occupational respiratory disease, lung disease from silica exposure has been reported from hundreds of years. The role of cement dust in relation to the development of Chronic Obstructive Pulmonary Disease (COPD) and pneumoconiosis is not clear. Some studies have shown a possible relationship between cement dust exposure and the risk of COPD (Medical Research Council1, 986), but other studies have not found any increase in the prevalence of COPD among cement workers compared to controls (Fell et al., 2003; Oleru, 1984). Exposure to cement dust at the workplace is known to cause chronic respiratory ailments in the form of cough, dyspnea or chronic bronchitis on the exposed workers (Abrons et al. 1988). MATERIALS AND METHODS Study samples The study was conducted on 170 male workers exposed to Portland cement which had no symptom of respiratory diseases prior to work. Also a unexposed group of 170 healthy unexposed male workers in office jobs from a number of companies were selected. The independent variables including; age, height, smoking, smoking history and number of cigarette in day, had not differed in exposed and unexposed workers. Age, height and weight were recorded for each member of exposed and unexposed groups in order to calibrate the spirometer. A detailed questionnaire was completed for two groups, providing information about duration of exposure to cement dust (years), smoking history and clinical symptoms. The exposed workers in the factory were divided into two groups of workers exposed to the dust produced by crushing and grinding calcareous materials (e.g. limestone, chalk) and argillaceous materials e.g. clay, shale (group 1), and exposed workers with cement dust (group 2). The number of samples obtained from each exposure zone was determined in proportion to the number of workers in the area. Table 1 shows the mean concentrations of respirable particles in the ambient air at the factory. The present study was aimed in evaluating occupational cement dust exposure (specially in stages prior to heating operation where workers have contact with the dust of primary substance containing unchanged quartz) and determining the prevalence of respiratory symptoms and its relationship to respiratory health effects, both acute and chronic respiratory symptoms and ventilatory function impairment among factory workers exposed to cement dust in a cement producing factory in Iran. Respiratory symptoms' questionnaire The British Medical Research Council's Medical Research Council (MRC), 1986 questionnaire on respiratory symptoms was used in our study, with revised and additional questions relevant to the objectives of the study. The questionnaire was completed during an interview. Before the interview the objectives of the study were explained to the participants and verbal consent was obtained. According to the MRC questionnaire, Dyspnea was graded into four levels of severity: I, normal (no dyspnea); II, dyspnea on effort hurrying on level ground or walking up a slight hill; III, unable to keep pace with people of own age and body build; IV, unable to walk at own pace without the need to stop to regain breath. Although In our study, there is not fourth grading. Respirable dust sampling and analysis In this study the gravimetric method was used to determine the concentration of respirable dust by drawing a known volume of air through a filter with known weight under controlled conditions (flow rate of pump, time of sampling). The most common personal respirable dust sampling devices were used (the 10 mm nylon cyclone). Respirable dust was collected on PVC filters with a pore size of 0.8 µ placed in a cyclone (Casella, London, UK) connected to a SKC pump (model 22430, SKC) with a flow rate of 1.7 L/min. Total dust was collected on cellulose acetate filters with a pore size 0.8 µ placed in a closed faced 37 mm cassette connected to a SKC pump with a flow rate of 2.0 L/min. Personal sampling was done during the 8 h morning shift. Reweighing of the filter gives a direct measurement of the dust weight. The mean weight for each area in the factory was assigned for each worker in that area, and was used for comparisons within factory areas as well as with the standard limits. Thirty five personal respirable dust and Thirty five personal total dust samples were collected and analyzed. The samples were analysed quantitatively by gravimetric analysis using a microbalance with a detection limit of 0.01 mg. The five respirable dust samples with the highest concentrations (Kiln, ore crushing and raw mills,) were analysed for crystalline silica by X-ray diffraction using National Institute for Occupational Safety and Health (NIOSH method 7500). Statistical Analysis A database file was created in a computer and statistical analysis was done by means of the statistical package for social sciences (SPSS). T-Test was used for comparison among exposed and unexposed groups. One-way variance analysis was used for comparison between groups (Tokey test was applied as a post hoc test for comparison between the groups). Chi-square distributions were done on data symptoms of respiratory. A p-value of<0.05 was taken as the level of significance. RESULTS Respirable dust The concentrations of total dust ranged from 15 mg/m3 in the kilns to 95 mg/m3 in the ore crushing areas and the concentrations of personal respirable dust ranged from 3.7 mg/m3 in the kilns to 23 mg/m3 in the ore crushing areas (Table 1). The percentages of silica measured in raw blend material by X-ray fluorescence (XRF) procedures, ranged from 7 to 7.43% and concentrations of crystalline silica measured by X-ray diffraction in air ranged from 0.01 to 1.76 mg/m3. Respiratory Symptoms 12.8 percentages of the exposed workers had grade III dyspnea, compared with 4.2% of the unexposed. This difference was statistically significant (P<0.05). However, anyone of the exposed workers had not grade IV dyspnea. 8.3% of the exposed workers claimed to have had episodes of acute bronchitis. This rate was higher than those (5.9%) reported by the unexposed workers. This difference was not statistically significant (P=0.37). Since cigarette smoking is a major confounder for respiratory symptoms, particularly cough and phlegm, a logistic regression analysis was undertaken for each of the respiratory symptoms, in addition to chronic bronchitis as outcome variable. Cough and phlegm, with or without shortness of breath, were significantly related to dust concentration (Table 2). Chronic bronchitis was found to be significantly related to dust concentration. Lung function Measuring pulmonary functions of workers exposed to dust and unexposed group showed a significant decrease in vital capacity (VC), forced vital capacity (FVC), FEF25-75 and FEV1 (P<0.05) also in terms of categorization pulmonary diseases patients who were exposed to cement dust more than unexposed group showed the symptoms of restrictive disease (Table 3).The FEV1/FVC% in two groups did not differ significantly (Table 3). Measurements of lung function were made using a Spirometer. All tests were performed in the sitting position and the subject was asked to exhale into the spirometer as forcibly as possible after maximum inspiration. DISCUSSION The concentrations in all samples exceeded the recommended threshold limit value (TLV) adopted by the American Conference of Governmental Industrial Hygienists (ACGIH) for nuisance respirable particulates, which is 10 mg/m3 of air if having contain no asbestos and/or less than 1% silica and for silica TLV is 0.025 mg/m3 (ACGIH, 2007). The mean of respirable dust and percentage of quarts were more than the ACGIH recommend upper limit in measured areas in the company (ore crushing, raw mills, cement packaging Kilns and Cement mills). This finding is in conformity with other reports for example, Workers who were in close contact with the production processes have been reported to have high exposure to total cement dust (11-230 mg/m3) and respirable cement dust (2-46 mg/m3) (Mwaiselage et al., 2005). Whereas a close look at production line reveals that more than half of the workers in stages prior to heating operation have contact with the dust of primary substance containing unchanged quartz. The dust of free silica is the most detrimental and causes pulmonary fibrosis and lung cancer (ACGIH, 2007). So work environments containing silica dust requires the investigation of the effects due to the dust. This study showed that work environments of cement industry have required more attention on the part of health expert and examination while stages prior to heating operation and post sections must be investigated separately. The findings in the present study showed a high level of dust, with a prevalence of wheezing, shortness of breath, cough, phlegm, dyspnae and higher among the exposed workers than the unexposedsconditions related to cement dust in the workplace. This study has shown that occupational exposure to air transmitted respirable and total cement dust is overexposure relative to occupational exposure limited (OEL) in Khash Portland cement factory. Our study has confirmed that exposure to cement dust is associated with acute respiratory symptoms and chronic ventilatory function impairment. Occupational dust is known to be an important factor in the causation of the symptoms of bronchitis in exposed adults (Becklake, 1989 Prodan, 1989; Mengesha and Bekele, 1998). However, Vestbo (Vestbo, 1993) did not find a clear association between the rate of hospitalization and exposure to cement dust. Prevalence of III-grade dyspnea on effort was 12.8% among the exposed as opposed to 4.2% among the unexposed workers. This difference was statistically significant. The results of respiratory symptoms and lung function in this study showed that exposure to cement dust at the workplace could be resulted to chronic respiratory ailments in the form of cough, dyspnea, or chronic bronchitis on exposed workers. These findings raise a strong possibility that cement dust was the cause of the wheezing, shortness of breath. High rates of bronchial asthma have been previously reported from other parts of the world (AbuDhaise et al., 1997; Al-Neaimi et al., 2001; Laraqui et al., 2001). Abrons et al., reported a high rate of breathlessness among cement workers compared with blue-collar workers (Abrons et al., 1988). The current OEL for total dust (10 mg/m3), which is used in a number of countries, seems to be too high to prevent respiratory health effects of the dust-exposed cement workers. These findings contribute to a scientific basis for further in-depth research on the cement dust exposure (especially in stages prior to heating operation in which there is the dust of primary substance containing unchanged quartz, and setting of a new occupational exposure limit. The decline in pulmonary function (FEV1, FVC, and FVC/PVC) of workers exposed to cement dust depends on the concentrations of respirable dust in the environment and the duration of employment. Thus, we recommend that ventilation systems and use of personal protection devices should be compulsory in the workplace of ore crushing and workers should receive regular screening for lung disease. ACKNOWLEDGMENTS The authors are grateful to the Zahedan University of Medical Science authorities for their support both financially and administratively. The authors are also grateful to the respondents who participated in the study. Also thanks to the Khash Portland Cement Factory management for their cooperation during the data collection and also thanks to Mrs. M. Kebriaei for reviewing the manuscript. REFERENCES
© 2008 Tehran University of Medical Sciences Publications The following images related to this document are available:Photo images[se08034t3.jpg] [se08034t2.jpg] [se08034t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}