 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Nigerian Journal of Surgical Research, Vol. 6, No. 1-2, Jan-June, 2004,
pp. 7-10
Cancrum oris among Nigerian children D. S. Adeola, S. A. Eguma and C. N. Ononiwu Departments of Oral and Maxillo-facial Surgery
and Anaesthesia, Ahmadu Bello University
Teaching Hospital, Kaduna Code Number: sr04003 ABSTRACT Background: Cancrum oris
is a serious health and social problem in developing societies. A retrospective
review of Cancrum Oris patients seen in ABUTH over a ten- year period was done
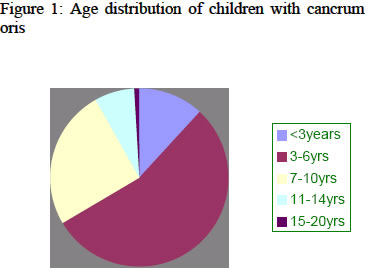
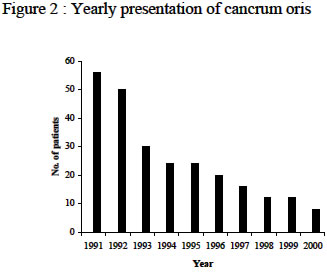
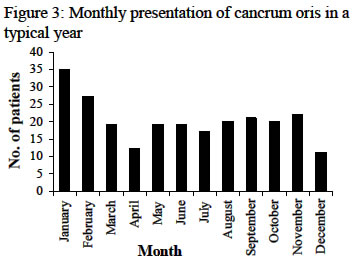
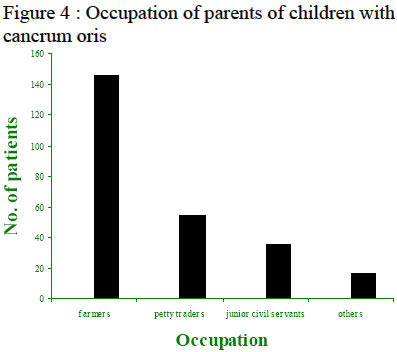
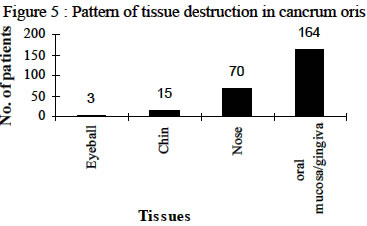
to determine the predisposing factors and management. Key words: Cancrum oris, children, malnutrition, oral hygiene INTRODUCTION Cancrum oris was first described by Tourdes 1 as a gangrenous affectation of the mouth especially attacking children in whom the constitution is altered by poor oral hygiene and serious illnesses especially the exanthematous fevers. It was known as early as the time of Hippocrates. 2 Most of the cases described in the literature 3 - 6 were seen mainly in the West African Sub-region by Tempest 6 and Enwonwu 5 in Western Nigeria and Adekeye 4 in Northern Nigeria. MATERIAL AND METHODS A ten -year retrospective study of two hundred and fifty-two children infected with cancrum oris seen and managed at the Maxillo-Facial Unit, Ahmadu Bello University Teaching Hospital Kaduna was undertaken. Data was obtained from patients’ case notes, theatre records and clinic notes. Parameters recorded included: name of patient, hospital number, sex, age, tribe, routine immunization; occupation of patients’ father, and the number of wives he had. The complaint presented with, the age at onset of disease, treatment received before attending the clinic, the site of the disease and tissues destroyed were also noted. The period of the year when the disease occurred, the mode of presentation of the disease, the number of defects caused in the oro-facial region as well as the nutritional status of patients were also recorded. Other parameters studied were genotype, haemoglobin levels, body weight, serum protein levels and any associated medical conditions. Oral hygiene assessment and whether or not patient had routine immunization before the onset of the disease were documented. Mortality and residual defects persisting after treatment were noted. RESULTS The youngest patient seen was 9 months old while the oldest was 18 years. Majority of the patients with cancrum oris who presented to hospital were between 3 and 6 years of age (Figure 1). There was no significant difference in sex distribution. The M: F ratio was 1.08: 1. A steady decline was noticed in the yearly presentation of from 1991 to 2001 (Figure 2). In a typical year, monthly presentation at the clinic was as shown in figure 3. There appeared to be a seasonal relationship in the pattern of presentation. One hundred and forty four (57.1 %) patients were seen during the dry season (October-March) while 108 (42.9 %) were seen during the rainy season (April-September). Cancrum oris seemed to affect the Hausa-Fulani more than the other tribes in Northern Nigeria. 175 (69.4%) were Hausa-Fulani, 17 (6.7%) were Yorubas, 10 (4%) were Ibos and 50 (19.8%) were from other Nigerian tribes. The disease was found to occur significantly in the children of low- income earners such as farmers (58%), petty traders (22%) and junior civil- servants (14%) than in other professions (6%) (Figure 4). Analysis of the marital status of patients’ fathers and their family size showed that 66.6% of patients were from polygamous homes. 36 (14%) of patients came from homes with less than 5 children while 216 (86%) were from families with more than 5 children. Thirty five (13.9%) of patients had had routine immunization between birth and one year of age, 210 (83.3%) had no immunization while 7 (2.8 %) were not sure of their immunization status. Majority of the lesions seen in this study occurred on the right side of the face. Only 70 (27.8 %) of lesions were bilateral. Twenty percent of lesions occurred on the mandible, thirty- six on the maxilla and forty-four involved both mandible and maxilla. The pattern of tissue destruction is shown in figure 5. The specific tissues involved were eyeball (3), chin (15), nose (70) and oral mucosa and gingiva (164). The predisposing factors to cancrum oris found in this study are shown in Table 1. Some patients had more than one predisposing factor. One patient developed cancrum oris two weeks after commencement of cytotoxic drug therapy for Burkitts lymphoma. Two patients were found to be HIV sero-positive. Table 1 : Predisposing factors to cancrum oris in 252 children
Lesions started either as jaw swellings, pimples, rashes, gingival bleeding or frank ulcers. The duration of the acute phase of the disease varied between 3-15 days. One hundred and fifty patients had body weights below the 95th percentile for their age, while 180 had haemoglobin less than 10g/dl. Of the 50 patients who had serum protein estimation, 40 had total serum protein less than 65g/dl. Complications seen during and after treatment included ankylosis (fibrous and bony), scalp and cervico-facial abscesses, facial deformity, speech impairment and micrognathia. Two (0.8%) patients died as a result of septicaemia before the acute phase of the disease was controlled. MANAGEMENTThis consisted of four parts; Chemotherapy, local wound management, general management and surgical treatment of secondary deformities. Chemotherapy consisted of treatment with antibiotics, multivitamins and haematinics. Metronidazole and penicillin were given for one week. Other drugs given were folic acid, iron supplements and Vitamin C. The wound was kept clean by twice daily irrigation with hydrogen peroxide and normal saline. It was dressed with gauze ribbon soaked in Eusol. General patient management involved treatment of existing diseases like malaria, bronchopneumonia, measles etc. Patients were fed high protein diets. The diet used in this series is called “Kwashiorkor Pap” or “Kwashi Pap”. It is constituted by mixing 1g of ground guinea corn, 2g ground soya beans, 1g ground crayfish, 2g roasted ground groundnuts, 20g ground dried fish and some boiling water. Patients were fed with the pap three times a day. Other foods like eggs, beef, casilan and milk were recommended to parents who could afford it. Where the patients had difficulty with mouth opening, a nasogastric tube was used in feeding. Dehydration and electrolyte imbalance were corrected. Some patients had blood transfusion prior to surgery. Surgical treatment was done to remove grossly mobile teeth, sloughing tissues and sequestra and to release ankylosis. Sequestrectomy and release of ankylosis were carried out under general anaesthesia. DISCUSSION Cancrum oris is a highly devastating disease that causes not only physical and aesthetic disability but also a lot of psychological trauma and depression to its victims. The residual defects left behind in these patients can never be fully quantified. Even after treatment such residual defects as gross facial deformity, ankylosis, teeth loss, speech impairment and masticatory defects may cause loss of self- esteem and confidence in the patient. The majority of cancrum oris patients are young people in their pre-teenage years as shown in this study. Every effort should therefore be made to prevent the disease. This study showed the peak incidence of cancrum oris to occur between three and six years. This is in agreement with earlier studies. 7, 8 The youngest patient was nine months old. The two teenagers seen in this study were HIV positive. HIV may well be a predisposing factor to cancrum oris in older people. No significant sex predilection to the disease was observed in this series. There was a seasonal relationship in the presentation of cancrum oris. More cases were seen in the dry season popularly referred to as the “hungry months”. This period also coincides with the peak of the measles and malaria epidemic in this part of the country. The decline noticed in the yearly presentation could be as a result of establishment of more hospitals and health centres across the country where these cases are easily picked up rather than a decline in the number of new attacks. Measles was the most common predisposing disease followed by malaria fever. Other studies had made similar findings. 6, 3 The ground work for the development of cancrum oris seems to be laid by immune deficiency states as is evident in the predisposing factors seen in this study. Parental occupation, marital status and family size are all social factors, which had a negative impact on the children that had cancrum oris. The disease was more common in children from polygamous homes, homes with more than five children and those whose parents were in the low socio-economic group. Earlier reports from Nigeria found cancrum oris to becommon in children of parents in the low socio-economic group. 5 - 8 This is also the section of the population with the lowest level of health awareness, personal hygiene and economic power. Large families with low income result in inability of the man to provide sufficiently for his family. Routine immunization against common childhood communicable diseases should be encouraged as only 13% of the children immunized were affected by the disease. More than half of the lesions occurred on the right side of the face in this study. This finding is different from that of Tempest 6 and Raynaud 9 who found 34% and 100% of the lesions respectively to be bilateral. The mortality has drastically reduced since the advent of antibiotics as only 0.8% was recorded in this series compared with 70 – 80% in the pre-antibiotic era. 1 Morbidity, however, is still high and long lasting. Defects such as ankylosis of the tempero-mandibular joint, osteomyelitis, loss of teeth, speech defects, micrognathia, masticatory defects, cervico-facial abscess and gross facial deformity which persist long after the disease has run its course may render these patients social outcasts for life. Poor oral hygiene, protein energy malnutrition and the presence of debilitating diseases render children susceptible to cancrum oris. Efforts should be made to improve economic empowerment and health education in order to curb the menace of cancrum oris with its devastating effects on young people. REFERENCES
Copyright 2004 - Nigerian Journal of Surgical Research The following images related to this document are available:Photo images[sr04003f3.jpg] [sr04003f2.jpg] [sr04003f1.jpg] [sr04003f5.jpg] [sr04003f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}