 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Nigerian Journal of Surgical Research, Vol. 6, No. 1-2, Jan-June, 2004, pp. 67-68 Case Report Middle ear effusion from metastatic carcinoma of the breast N. C. Okpala and A. Nigam Otorhinolaryngology Department, Salisbury District Hospital, Odstock Road,
Salisbury SP2 8BJ, UK Code Number: sr04020 ABSTRACT Carcinoma of the breast can metastasise to many organs. Metastasis to the temporal bone is rare and even when it does, it would usually spread to other parts of the body. This is a report of isolated metastasis to the temporal bone with middle ear effusion. Key words: Carcinoma, breast, metastasis, temporal bone, middle ear effusion INTRODUCTION Carcinoma of the breast can metastasise to many organs including the skull and brain. Metastasis to the temporal bone is extremely rare. 1 An unusual presentation of isolated metastasis with middle ear effusion is reported.
CASE REPORT
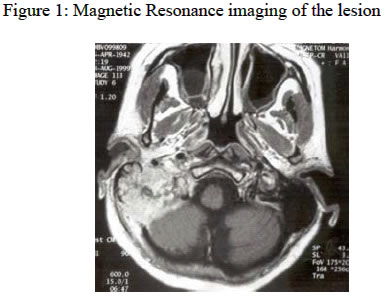
A 45 year old woman presented with a short history of blockage and pain in the right ear. She also complained of a feeling of pulsation in the ear and increasing post-nasal catarrh with some blood. This followed an episode of cold and persisted despite treatment with antibiotics and nasal steroid drops. She was a known patient of carcinoma of the breast, having had wide excision and axillary clearance 2 years earlier. She subsequently had adjuvant chemotherapy and radiotherapy to the right breast due to positive right axillary lymph nodes. Physical examination showed tenderness in the mastoid region. Fluid was also found in the middle ear. A right grommet was inserte4d under local anaesthesia. The symptoms persisted despite treatment. Bone scan showed a hot spot in the right mastoid. Magnetic resonance imaging of the petrous ridges showed an irregular enhancing mass eroding and occupying the middle and inferior aspects of the right petrous temporal bone. This extended into the adjacent occipital bone, occipital condyle and the posterior cranial fossa where it was causing a slight mass shift on the right cerebellar hemisphere. There was some dural enhancement indicating dural inflammation. Fluid was also seen within the middle ear and external auditory canal (Figure 1). DISCUSSION Carcinoma of the breast is known to metastasise to many organs. 2, 3 Studies of patients with stages I and II disease indicated that only a few (<5%) exhibited signs of skeletal involvement at the time of diagnosis. Bone metastasis are found in 28 - 75%) of patients with stage III disease 4 and 50 – 80% in autopsy studies. 4, 5 Metastasis to the temporal bone is rare, usually asymptomatic and diagnosed mostly at autopsy. 1, 6 Tumours of the temporal bone arise mainly from the epithelium of the Eustachian tube. 7 Metastasis to the bone is by haematogenous, meningeal, leptomeningeal and direct spread. Depending on the mode of spread, the bone may be involved in various locations. Most haematogenous spread are to the petrous apex, 6, 8 – 10 which is marrow rich. The petrous apex was involved in this patient. Tumours in this region are asymptomatic until they cause otologic dysfunction or pain. Hearing loss, otalgia, preauricular swelling and facial nerve paralysis, 6, 8 – 10 have been reported. In this patient, an unusual presentation of middle ear effusion resulted in diagnostic delay. Persistent of symptoms aroused suspicion.
Copyright 2004 - Nigerian Journal of Surgical Research The following images related to this document are available:Photo images[sr04020f1.jpg] |
| |||||||||

{kind=link}