 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Nigerian Journal of Surgical Research, Vol. 8, No. 1-2 , 2006, pp. 44-48 Outcome of traditional bone setting in the Middle belt of Nigeria 1H.C. Nwadiaro,2P.O. Nwadiaro ,3A.T. Kidmas and 3K.N. Ozoilo Departments
of 1,3Surgery and 2Zoology, University of Jos. Code Number: sr06007 Abstract Background:
This hospital based study was designed to
elucidate the outcome of Traditional Bone Setting (TBS) practice in four states
of the middle belt of Nigeria, via complications presenting in select
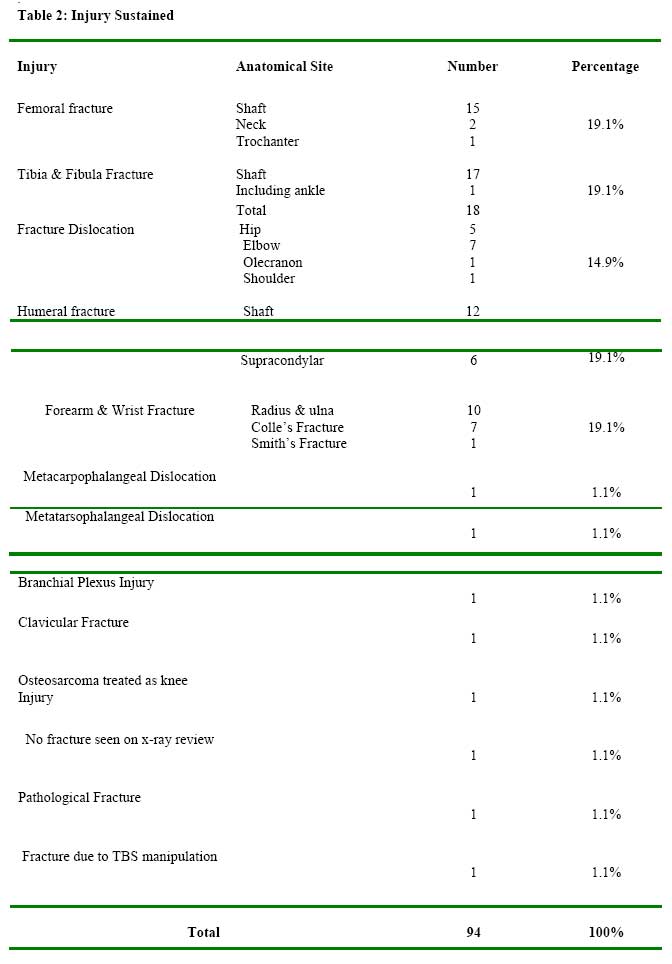
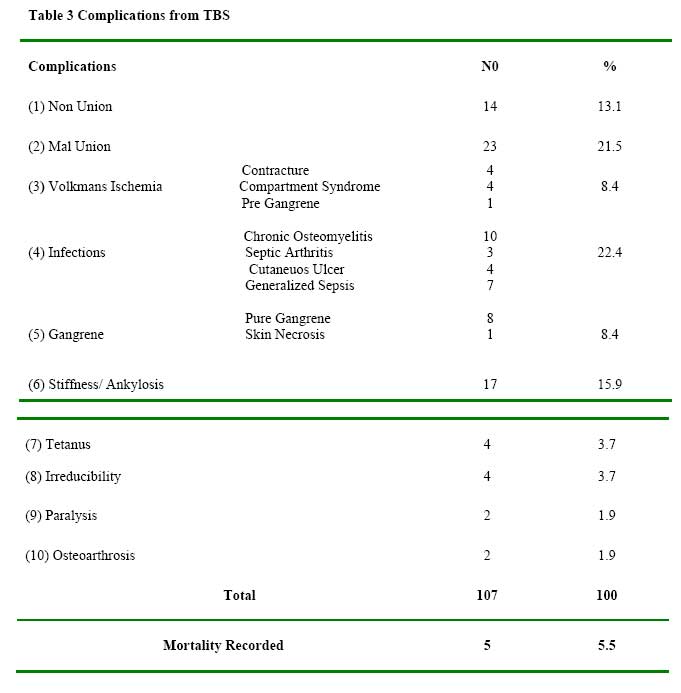
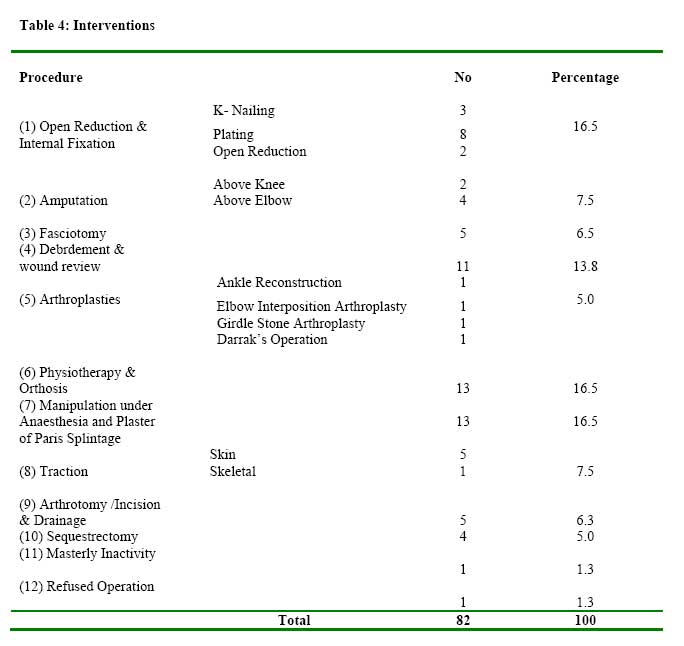
hospitals. Key words: Traditional bone setting, Complications middle belt, Hospital based. Introduction Complications arising from the practice of Traditional bone setting contribute significantly to the challenges of orthodox orthopaedic practice.1 Various non scientific observations give conflicting estimates of the impact of such practice in our environment. Moreover, various studies have concentrated on different aspects of the practice (TBS). Adegbule, G.T. working in Lagos has classified stiffness of the elbow arising from TBS practice from grades 1-6 in increasing difficulty of reconstruction and termed it Bone Setters’ Elbow.2 Katchy A.U. et al at Enugu studied Traditional bone setters’ treatment of femoral fractures and found an unacceptably high rate of complications.3 Eze C.B. in Enugu and Onumiya J.E. in Jos documented gangrene of limbs arising from traditional sources 4,5, while Garba E.S. and Deshi P.J. in Zaria asserted that the major pathology leading to amputations was trauma and gangrene due to inappropriate splinting of fractures by traditional bone setters. Ogini L.M. in Ile-Ife studied use of traditional fracture splints for bone setting in 25 patients and concluded that there was a high incidence of mal-union and non-union in long bone and patellar fractures with the exception of the humerus .7 Nwadiaro H.C. et al found that 75% of amputations in children below 16 years of age resulted from activity of bone setters in Jos.1 Alonge et al studying traditional bone setters in south western Nigeria concluded that the complications that accompany their practice are unacceptable. 8This hospital based study was undertaken as part of a “Three-phased” study to elucidate the actual outcome of TBS in the Middle Belt of Nigeria. It is specifically geared toward obtaining a scientific and statistical basis for assessing the practice of TBS. Patients And Methods This is a combined retrospective and prospective study of outcome of TBS practice in the Middle belt. It covers four referral hospitals with the study area, consisting of Plateau, Nasarawa and southern parts of Kaduna and Bauchi States. Presentation of complication of fractures between December 1999 and November 2000 were retrospectively studied. The case notes were obtained from the individual hospitals’ retrieval system3 and cases noted as having had traditional bone setters’ treatment recruited. The prospective study involved recruitment of consecutive presentations of complication of fractures that have had previous TBS treatment in the various study hospitals between Jan-Dec. 2001. Research collaborators were involved outside Jos University Teaching Hospital. Recruitment points were mainly the Accident and Emergency Units and the Orthopaedic out-patient clinics. Deliberate efforts were made to obtain sequence of treatment prior to presentation. Information garnered were entered into a preplanned protocol that included demographic data, educational status, types of injury, presentation of complication and treatments offered in hospitals. Results Fifteen cases from the retrospective aspect of the study and seventy-six from the prospective gave a total study population of ninety-one. Of these there were 56 patients from Plateau State (61.5%), 18 from Nasarawa (19.8%), while 11 (12.1%) and 6 (6.6%) were recruited from Kaduna and Bauchi States respectively. There were 69 males and 22 females giving a M: F ratio of 3.1:1. The age distributions of the patients are as shown in Table 1. Majority of the patients were children in the 1st decade of life (34.1%) while people in the 3rd and 4th decades constituted 20.9% and 18.7% respectively. The patients cut across all educational strata with a preponderance of illiterates, children and primary school certificate holders (74.7%). There were a total of 92 injuries with equal distributions among femoral, tibia and fibular, humeral and forearms and wrist fractures (19.6% each). One patient sustained pathological fracture while in another fracture resulted from the TBS manipulation. In one patient, no fracture was seen on x-ray. The distribution of the injuries is shown in Table 2. The presentations of complications varied widely as depicted in Table 3. The most frequently occurring complications were infection and mal union with 22.4% and 21.5% respectively. These were followed closely by stiffness/ankylosis 15.9% and non union 13.1%. A mortality of 5 patients was recorded giving a mortality rate of 5.5%. There were a total of 82 interventions. The distribution of the interventions is shown in Table 4. Open reduction and internal fixations, physiotherapy and orthosis and manipulation under anesthesia and Plaster of Paris splint were offered to 13 patients each. Six patients had major amputations. A policy of masterly inactivity was adopted in one patient while another refused operation. Discussion We note that in the one year retrospective study, only fifteen patients were identified, in contrast to seventy six recruited in the prospective phase within the same time frame. This underscores the unreliability of retrospective data. From the incidence of 76 cases in one year (averaging 6 per month), from the prospective study the activities of traditional bone setters’ clearly cannot be ignored. More so, since most of the complications are avoidable.1 In this series, all the five mortalities were encountered in the prospective phase of the study. It is not likely that the above figures are representative of the outcome of Traditional Bone Setters practice in the study area. It may indicate the fraction of patients that believe further help could be obtained from orthodox health institution. The preponderance of children in the first decade of life (34.1%) is a further cause for concern. This population is largely dependent on parental decisions. It would appear from this series, that educational status does not influence patronage of traditional bone setters, however, it does appear to be higher among people of lower educational levels. The distribution of injuries that is presented to traditional bone setters is varied. We note a case where treatment was instituted without a fracture and another where fracture was occasioned by traditional bone setters’ manipulation. In one patient, osteosarcoma was treated as a case of traumatic fracture. The above incidences call to question the diagnostic acumen and competence of traditional bone setters.9 This position has been held by a number of studies on traditional bone setting practice from different parts of the country. Out of Eighty-two interventions, thirty-two were major orthopaedic procedures including 6 major amputations, 4 of which were above elbow amputations. This concurs with the already held view that traditional bone setters are a major source of orthopaedic complications.1,5,6,8 In conclusion, we note that despite the findings of various studies, which suggest little to recommend in the practice of traditional bone setting, the practice continues to thrive.9 Ninety one complications with six mortalities largely avoidable in two years is unacceptable. We recommend that other zones undertake similar integral studies of traditional bone setting practice to produce a national picture that would form a bedrock for future policy dialogue. References
Copyright 2006 - Nigerian Journal of Surgical Research The following images related to this document are available:Photo images[sr06007t2.jpg] [sr06007t3.jpg] [sr06007t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}