 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Nigerian Journal of Surgical Research, Vol. 8, No. 1-2 , 2006, pp. 49-53 Arterial trauma of the extremities. An Ivorian surgical experience(Côte d’Ivoire) 1H .Yangni-Angate, 1G .Ayegnon, 1C.H. Meneas, 2 Y. Yapobi and 2M. Kangah 1Department of Thoracic and Cardio-vasculary surgery University
Hospital Center of Bouake And Institut de Cardiologie d’Abidjan 2Department of Cardio-vasculary Institut de
Cardiologie d’Abidjan 3Department f
Anesthesia and Intensive Care Institut de Cardiologie d’Abidjan Code Number: sr06008 Abstract Objective: The goal of this retrospective study
is to present our epidemiological , clinical and surgical experience of the
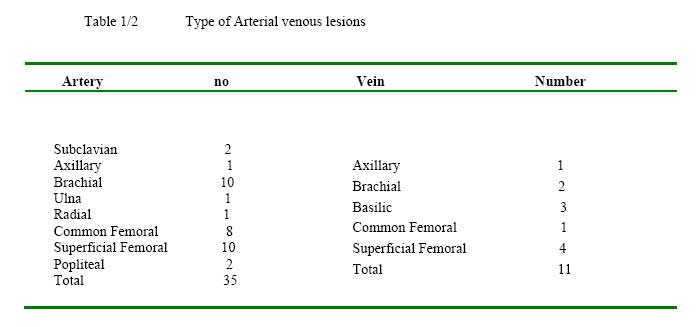
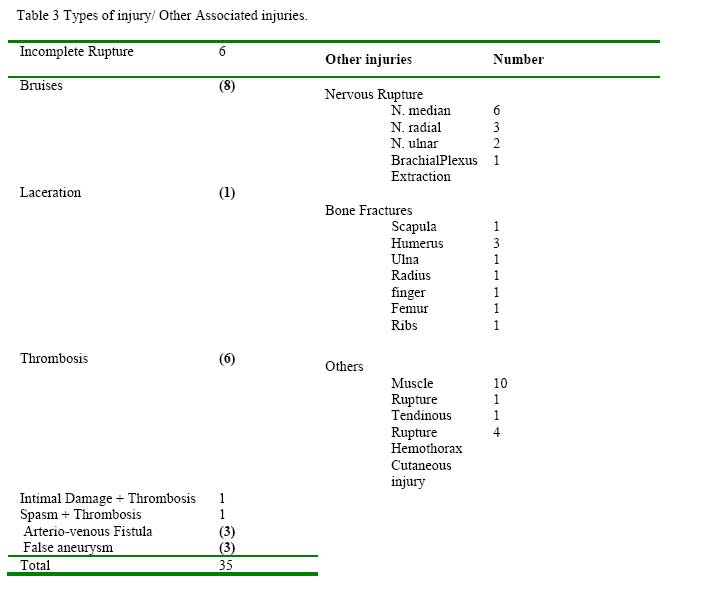
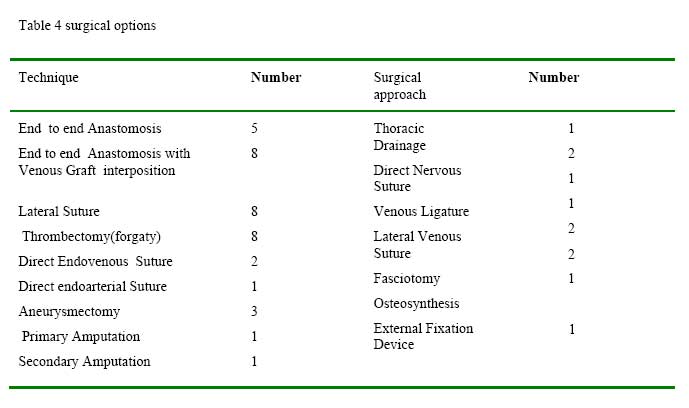
arterial injuries of extremities for 23 years(1977 to 2000). Key Words: Limbs ,Arterial trauma , Surgery. Introduction Arterial injuries are true surgical emergensies.During their acute phase, signs of arterial trauma of the limb may be lacerations and bruises. Unrecognised at the initial stage, these traumas can evolve chronic injuries with a clinical setting where false aneurysms and artero venous fistulas are predominant.According to Aulong1 , if “the diagnosis is sometimes obvious, it is generally debatable or misleading”. Indeed, errors or delays in the diagnosis have been reported by Jacob2 with a rate estimated at 12 %. As a consequence, there is need for a good clinical assessment when encountered with any suggestion of arterial trauma of the limbs. The treatment is above all surgical3 4 5 6 and the various surgical techniques have well codified indicators7 . In Sub- Saharan Africa the characteristics of arterial trauma are still unknown due to the unavailability of studies related to this subject. In order to better understand the characteristics in Africa, we report a group of 35 Ivorian cases managed by us over a period of 23 years. Material and Methods Thirty five cases were managed within the 23 year period 1977 – 2000. Data was retrieved from their case files and anlysed retrospectively. ResultsTwenty nine presented in the acute phase following trauma and 6 presented late. Thirty of the patients were male and 5 female with a ra tio of 6:1. The age range was 14 months - 63 years with a mean of 25.4 years. The etiology of arterial traumawere: I, knives (n = 15) ii, guns (n = 5), iii, occupational accidents (n = 3) iv, road traffic accidents (n = 3) and v, iatrogenic following cardiac catheterisation (n = 8) and at blood transfusion (n = 1). The types of arterial lesions, were different in the arteries and veins (tables 1-2, 3, 4). Of the 29 patients presenting with acute arterial injury, 28 had complete ischemia.14 were incomplete and 14 had complete ischemia. There was total absence or clear diminution of the distal pulse of the affected artery . In one case, the distal arterial pulse was present despite the existence of a clinically demonstrable proximal lesion. Modes of presentation are varied as shown in (table 5) There was limb edema in 4 patients, Haemorrage in 9, hypovolemic shock in 4. Of 6 patients with Limb hematoma one did not have ischemia . Among patients presenting late 3, had false aneurysms and 3 had artero-venous fistulae . Two of the 3 false aneurysms, were compressive. The three artero -venous fistulae presented with arterial thrills and continuous systolic murmurs . One of them was complicated by a right cardiac deficiency; in a patient harboring an A-V fistula for a period of 25 years involving the left femoral artery and common femoral vein following a knife stab injury. There was no need for additional tests after bedside evaluation in 27 patients. It was necessary to conduct further tests in 3 patients presenting late with i, an artero-venous fistula, ii , a false aneurysm and an iii, obstructive arterial thrombosis. The study of pressures through external compression, a non invasive method, was never applicable. An arteriography was useful in 8 patients because of doubt in the anatomic definition of the injury in 7 patients and because of the necessity to make a precise diagnosis in one patient. The time interval from injury to surgical intervention was different: In 17 the patients surgery was within 10th hour:; 5 had surgery between 10 and 24 hours of injury: 7 were treated after 24th hours. All the patients had surgery. The surgical procedures carried out are listed on tables 6, 7. Arterial patency was established after surgery in 33 patients. Amputation was indicated in two patients with complete ischemia (primary and secondary).Outcome: Significant morbidity was encountered in a five patients with two deaths. In one patient each there was Renal insufficiency , Persistent limb disability and Persistent radial nerve paralysis. Two patients had wound infection and two patients died from I, biliary peritonitis and ii, late revascularization syndrome after arterial reconstruction in late presentation ( 24 hours after injury). Discussion Within 23 years, 35 cases were managed for arterial trauma of limbs with an annual frequency of 1.5 %. Arterial injuries appear not to be frequent in civil practice, as is suggested in this study and an earlier Ivorian arterographical report 8. Other authors have reported annual frequencies ranging from 1.73 - 4.62 % 9,10There is a male preponderance and the young and active are affected ( 23 to 36 years) in most reports 11 12 13.The mean age in our study is 25.4 years . The commonest etiologic agent differ among regions and reporting from Nigeria Igun, reported road traffic accidents as the most frequent cause in his study 14 ; with iatrogenic causes less often , compared to our experience.( 21 % of cases against 25.7 %).Knife cuts were the commonest cause of limb injuries in our study similar to findings in another report by Olusanya Adeyemi Duro 15 and Eren16. In USA the commonest cause of arterial injury is gunshot11 this may be due to easier assess to firearms in USA.The commonest injured vessels were the brachial ,femoral and popliteal vessels and the lower limbs were most commonly injured as reported in other studies. 8 3 7 14 16 17We do not have any reason to this preferential localization to the lower limb.The predominance of knives causing arterial lesions in our study , could explain also the dominance of the arterial rupture (57 %) in our sudy. This type of injuries encountered has previously been reported by Igun14 and Drapanas 18 . Late presentation is not frequent in our experience and 90% of our patients to presented early as in other studies.9,20,21 Late lesions, (false aneurysms and arter-ovenous fistulae) account for 17 % of all our injuries but this is conspicuously absent in the experience of Igun 14), though Olusanya Adéyemi’s Duro15 working in the same region as Igun has reported true aneurysms in his study.Lower limb aneurysms are not identical in presentation and late lesions seem less numerous in civil practice. Associated nervous injuries were encountered in the upper limb Also noted were long bone fractures in 0.2% of injuries and were most usually seen in the multiply injured patients following road traffic accidents.In the patients we managed suspicion of an arterial lesion was th presence of lacerations and bruises with limb ischemia. Initial clinical assessment is sufficient to localize with precision an arterial injury. The predictive value of the clinical assessment is 100 %22. Additional diagnostic test were not necessary in 77 % of our patients. The reliability of the clinical assessment has been reported by Frykberg’s22. Arteriographical investigations to improve anatomical description of the lesion and enhance certainty of clinical assessment could negatively lengthen the ischemic period and delay the surgical operation and may be avoided in this circumstances7 Arteriographical tests are useful in keeping permanent reference of uncertain cases, and in the detection of lesions with many stages, in the appreciation of the arterial network permeability below the trauma and in the precision of the levels of arterial pathology.As demonstrated by Drapanas18 and Perry 23 the palpation of a distal pulse does not prove with certainty the absence of proximal arterial lesions . We start to suspect arterial injury if there is a large post traumatic hematoma on an arterial course as it was the case with on of our patients. The beating characteristics of the hematoma though described in classical ways37 may not be observed in case of recent arterial trauma. Its more complex in the patient with a hematoma that is non beating as seen in 6 of our patients. In our initial evaluation of recent arterial limb injuries we must look for the beating hematoma as aptly described in literature 37 though sometimes it may not beat as encountered in this study.The diagnosis of late lesions was not difficult. The three artero-venous fistulae were presented with the classical characteristics, and the false aneurysms were discovered through accidentally while investigating a swelling located on an arterial course.In some situations arteriography is needed.In the treatment of the patients there are several options to choose from: i Surgical correction to establish the flow of blood is the ultimate goal. ii, In the treatment of recent lesions options are, direct end to end anastomosis without tension, this was done in 8-patients iii, Anastomosis with interposition of a venous graft, using the reverted internal lower limb vein where there is a long segment of vessel wall lost at injury. iv, For the combined injury including bone fractures and arterial injuries, the arterial injury is given top priority to avoid acute ischemia .We have not recorded vascular complications following manipulation of fractures after initial vascular repair. An aponerotomy incision was carried out twice before the ischemic hour (the 10th hour), to restore arterial flow and avoid acute ischemia, edema and muscle destruction. The shorter the interval between injury and surgery , the better the results and the lower the amputation rate24 . All of our 17 patients that were operated within 10 hours were spared an amputation and had an uneventful post-operative period.. On the contrary, there was significant morbidity, amputation and death among patients presenting beyond 24 hours after trauma. Only 2 of our patients presenting within ischemicperiod 10 hours, had some post-operative complications. As similarly reported by Lena and d’Allaines 25 , we noticed that the risk of surgery, amputation and complications was higher after the 24th hour of ischemia. Conclusion Arterial injuries are not frequent in civil practice. The ischemic limb should be operated as soon as possible to avoid limb loss and other morbidity. References :
Copyright 2006 - Nigerian Journal of Surgical Research The following images related to this document are available:Photo images[sr06008t1-2.jpg] [sr06008t3.jpg] [sr06008t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}