 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Nigerian Journal of Surgical Research, Vol. 8, No. 1-2 , 2006, pp. 69-73 Waiting time among acute abdominal emergencies in a Nigerian teaching hospital: causes of delay and consequences N .Mbah, W. Ek. Opara and N. P. Agwu Department of
surgery, Usmanu Danfodiyo University Teaching Hospital, Sokoto,Nigeria. Code Number: sr06013 Abstract Background-In
many patients presenting with an acute surgical abdomen, the outcome of
management is determined by the promptness of the appropriate surgical
intervention. The average interval the patient has to spent waiting for
treatment at first presentation to hospital with an acute abdominal
emergency is unknown in our center. This study was designed to evaluate the
waiting time between hospital presentation and operation,to highlight causes of
the delay and outcome of treatment among patients admitted with emergency
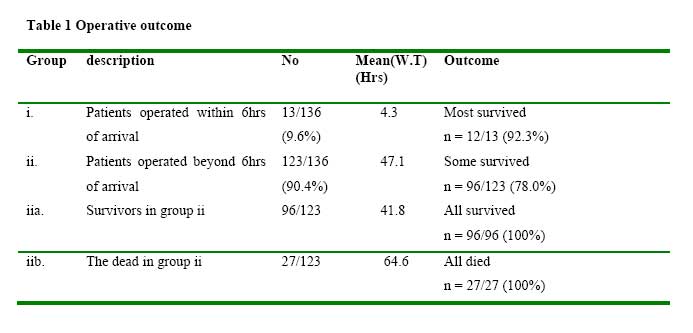
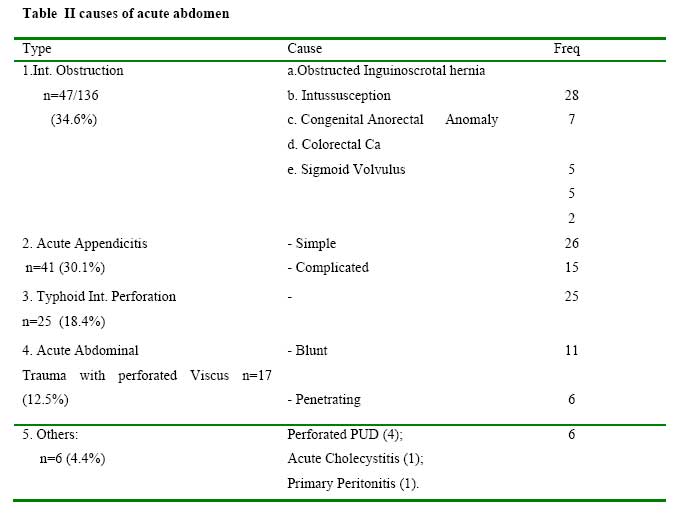
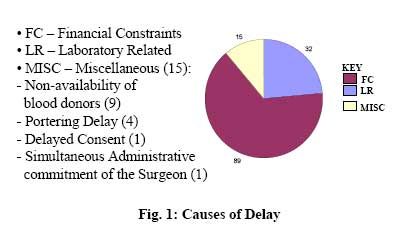
abdominal events in a Nigerian tertiary health Centre. Key words: Waiting time, Acute abdominal emergencies; Outcome Introduction Acute surgical abdomen are life-threatening emergencies. Early presentation of cases to the hospital and prompt surgical treatment of the clinically stabilized patient are imperative to the post-operative survival of the individual1. Delayed hospital presentation is common in most developing countries such as Nigeria2-7. In addition delay may caused by several factors in the hospital prior to emergency laparotomy. Factors often listed are; patients’ factors and institutional inadequacies 8,9. These delays contribute to further physiological deterioration of the sick, which is inimical to a satisfactory post-surgical outcome . Therefore the identification of these specific factors, and their elimination or control, will not only shorten the waiting time beforeemergency operations in communities similar to ours, but will also diminish the adverse outcome that associated with the management of acute surgical abdomen in our sub region. Materials and Method Usmanu Danfodiyo University Teaching Hospital [UDUTH], Sokoto is a 500-bed tertiary health institution situated in the northwestern part of Nigeria. It is a regional referral center for the numerous private, general and primary health institutions within this zone. Patients in our care were responsible for their upkeep financially for all categories( elective and emergency) of surgical care delivered. Method Over an 8-month period [March to October 2005], all 136 consecutive patients admitted into the emergency wing of the hospital with a clinical diagnosis of acute surgical abdomen were enrolled into study. The “waiting time” was defined as the interval between the time of presentation in the hospital and the actual time of operative treatment. Emergency surgery was considered delayed if the appropriate surgical procedure was not performed within 6-hours of arrival into the hospital. Within this period, the patients were fully resuscitated and clinically stable.Upon admission into the casualty unit of the hospital, the time of presentation was documented inside the patient’s case file. The scheduled time for operation was then calculated to fall within 6- hours from this time. Cases not operated outside this period were considered delayed. Subsequently, the actual time the patients arrived the operation room [O.R] was documented as the time of surgery. The vital signs were taken at the emergency department and monitored serially until operation. Blood and urine samples were sent for investigations. Emergency ultrasound scanning, electrocardiography and plain radiographs were done for some patients as relevant . All the patients were resuscitated on intravenous infusion and preoperative antibiotics commenced impirically. Blood was transfused to correct anaemia Urethral catheter was inserted to monitor hourly urine output. Nasogastric intubation was introduced in all patients with abdominal distention or were vomiting. Following the initial resuscitation, the patients were reviewed once in the casualty department by the anaesthetists for fitness for anesthesia and qualified by an ASA score. Informed consent for surgery was obtained from all the patients. Anypatients whose ASA score remained above ASA III E after the initial 6hours of arrival and resuscitation were excluded from this study. Results One hundred and thirty six consecutive cases of acute surgical abdomen were enrolled into the study. There were 95 males (69.9%) and 41(30.1%) females. The median age of the patients was 25 years (range 3 days to 75 years). All were Nigerians. The commonest clinical diagnosis was intestinal obstruction in 34.6% (n = 47/136). Acute appendicitis was a close second in 30% (n = 41/136) of cases (table 1). The waiting time prior to the emergency abdominal surgery was less than 6 hours in 13 (9.6%) and above 6 hours in 123 (90.4%) patients (table 2). The average waiting time was 44 hours. All factors that delayed the emergency operations beyond the 6-hour target after hospital presentation are shown in fig.1 Financial inabilities were in the majority (65.4%) an such patients were not able to purchase prescribed materials or pay for surgery. Some delays were multi factorial. One patient presently early but was operated after 9 hours due to the non-availability of the attending surgeon who was trapped by other urgent duties administrative in nature. The commonest post-operative complication was wound infection in 23.8% (n = 31/136), the majority of whom belonged to the group whose emergency operations were delayed (n=23/31).There were 28 deaths with a mortality rate of 20.6%. Of those who died 27/28 (96.4%) were in the group who were operated after 6 hours. Based on the waiting time versus outcome of management, the patients were distributed into 4 groups for the purposes of a clearer discussion (table 2) Discussion Previous studies from the developing countries are replete with reports of delayed presentation to hospital among all categories of patients. Explanations offered included ignorance, poor access roads, long distances to suitably equipped hospitals, poverty, among others 2-7. Upon arrival in the hospital, further delay was encountered before the definitive treatment could be provided due to a number of other factors. In order to differentiate between cases of acute surgical abdomen whom we considered had early emergency operation after arrival into the hospital, and those who did not, we chose an arbitrary period of 6-hours. This choice was predicated on the need to significantly shorten any further delay before the definitive treatment in these dire emergencies. Besides, previous reports indicated that adequate resuscitation of patients planned for emergency surgeries could be accomplished under 6-hours 1. Our study revealed that a significant majority (>90%) of emergency laparotomies in our center was delayed beyond 6-hours after the patients had arrived the hospital. No age or gender was exempt. A similar observation had been documented in other centers in the developing world 5,7. Majority of the delay in our own circumstance were for economic reasons. Income poverty is still rife in Nigeria. Many are jobless or under-employed10. The situation became aggravated since the economic recession in the 1980’s till date. The slump in the national economy led to the withdrawal of all government subsidies to healthcare and the introduction of user fees in all public hospitals in Nigeria irrespective of the patients’ age or their ability to pay. This situation is in sharp contrast with observations in developed nations where all surgical emergencies are conducted within the initial 6-hour period of patients’ admission into the hospital 1. Time is of a high premium in the surgical treatment of acute abdomen. Agreed, the surgeon may not influence the usually long delays before patients with acute abdominal emergencies in our sub region present to the hospital. However, once they arrive, almost all cases could be physiologically stabilized within the first 6 hours by aggressive resuscitative approach in order to facilitate the safe conduct of both anaesthesia and surgery. In a series of 251 children, workers in Ilorin, Nigeria, reported a median delay of 24 hours in the hospital before emergency laparotomies were performed6. Ours was more than 24 hours. In both studies however, the delay is unacceptably high. Reasons for the delay in the Ilorin series were not mentioned. In order to circumvent the usual delay caused by the patient’s inability to promptly pay for emergency surgical operations, some working in environments similar to ours suggested the formulation of a short-term credit facility, which provides immediate and comprehensive emergency services to all classes of patients in the form of a revolving fund 5. To sustain this scheme, it was mandatory for the beneficiaries to repay post-operatively before they could be discharged. This policy, if adopted in our centre, will prevent delayed emergency laparotomies in almost 2/3rds (65.4%) of patients. Besides poverty, institutional problems played an aggregate role in delaying emergency surgical treatment in our center in about 25% of cases. Findings in other published reports from the developed and developing nations however reflected organisational constraints similar to ours 8,9. Suggested remedies in those circumstances included efficient supervision of the process of emergency laboratory investigation and dispatch of the results within a fixed time frame in order to reduce unscrupulous delay. Similarly, the maintenance of a good communication network among hospital staff during emergencies through paging or text messages had equally been found beneficial. It’s however salutary to observe that the lack of a constant power supply, potable water for theatre and other hospital uses, insufficient operation gowns and linens previously reported elsewhere in our sub region as causes of delay were not contributory in our series5. The availability of several functional stand-by electricity generators, borehole facilities and adequate operation outfits in our center obviated these exigencies. It is a well-known fact that the longer the delay between onset of acute abdomen and their surgical treatment, the higher the morbidity and case mortality rates 11,12. The progressive physiological deterioration associated with such delays increased the risks of metabolic, cardiovascular, renal, pulmonary and septic complications before, during and after the surgical operation. Consequently, the post-operative morbidity recorded in the present study was more in those patients operated beyond 6 hours of presentation than in those who had early emergency laparotomy. Although hospital presentation in our sub-region is usually late, it was generally observed in this series that those who were operated within 6 hours of arrival were invariably those who were more likely to report early to the hospital following the onset of their illness, and vice versa. Therefore, while the cumulative delay in the former category of patients between onset of their symptoms and operative treatment was shorter, that of the later group was much higher. It seemed obvious that this clinical scenario was due to the difference in both the socio-economic standards and the level of enlightenment between these two classes of patients. Mortality in this study was predominantly in those whose operations were done after 6 hours even after grouping the patients with common clinical characteristics; ages, clinical diagnosis and ASA grading within the initial 6-hours of hospital admission and resuscitation. Several previous reports had shown a 4- to 9-fold increase in mortality risk when emergency laparotomy for acute surgical abdomen was delayed beyond 12 hours of onset of symptoms in cases of perforated gut 12,13. Conclusion Patients usually present late for treatment in developing countries. In our center, additional delay in the hospital was due to financial constraints in majority of cases. The adverse impact of prolonged waiting time in the hospital before emergency surgery for acute surgical abdomen in our environment has adverse consquences. Hospital based means of getting the patient treated and recovering the cost from a mini rehabilitation loan scheme may help a lot of our patients who immediately cannot afford the hospital bill. References
Copyright 2006 - Nigerian Journal of Surgical Research The following images related to this document are available:Photo images[sr06013t2.jpg] [sr06013t1.jpg] [sr06013f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}