 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Nigerian Journal of Surgical Research, Vol. 8, No. 1-2 , 2006, pp. 74-76 A clinicopathological study of Dermatofibrosarcoma Protuberans in Maiduguri, Northeastern Nigeria 1H.A. Nggada B.M. 2Gali and 2H.U. Na’aya 1Department Of Histopathology And 2Surgery
Universityof Maiduguri Teaching Hospital, Maiduguri. Code Number: sr06014 Abstract Background: Dermatofibrosarcoma
protuberans (dfsp) is a rare tumour originating from the dermis, it is slow
growing, nodular, polypoid neoplasm that invade the subcutaneous tissue and does
not usually metastasis.Clinical presentation is not uniform and may mimic
common tropical benign skin lesions.We intend to study the behaviour of this tumour
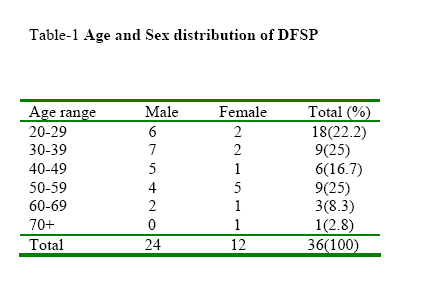
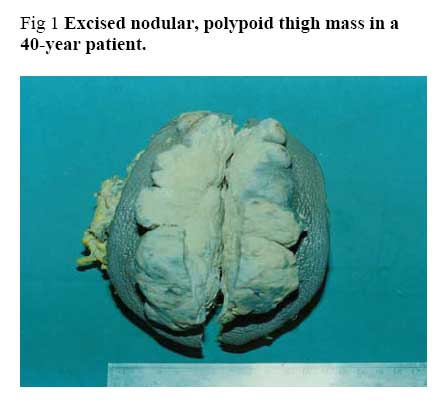
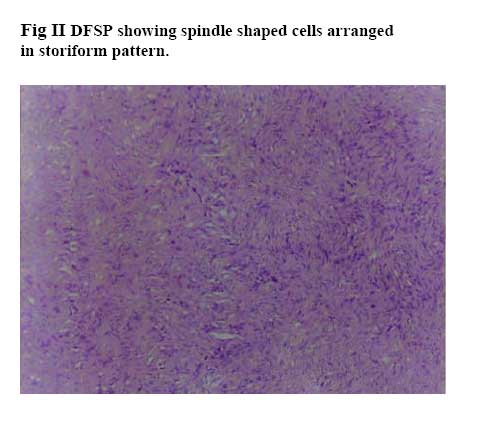
in our environment . Key Words: Dermatofibrosarcoma protuberans; Clinicopathology Introduction Dermatofibrosarcoma protuberans (DFSP) is not a common in most reports and originates from the dermis, it is a slow growing, nodular, polypoid neoplasm that invade the subcutaneous tissue and rarely metastasis.1, The aetiology of dfsp is not well known but antecedent trauma has been implicated as a predisposing factor in the development of malignancy.4 DFSP can undergo transformation to fibrosarcoma, although it is not clear whether this morphologic change reflects a more aggressive clinical form.5,6 Occasionally, DFSP may progression to a malignant fibrous histiocytoma8The diagnosis of DFSP is clinically difficult because it resembles a keloid or a hypertrophic scar, which are common in Africans8 It has been reported as a presentation in the breast as a primary breast lesion9.therefore, biopsy of the lesion is needed to make a diagnosis. however, the diagnosis can be made or at least suspected on the basis of fine needle aspiration material.10The tumour is radioresistant and therefore the acceptable management is wide excision and skin grafting.7 This study aims at identifying their age, sex, anatomical site distribution and compare with other skin malignancies in our environment. it is hope that this will form a baseline data and compare with other similar studies elsewhere. Materials and Methods This is a retrospective study of 36 diagnosed cases of dermatofibrosarcoma protuberans in the University of Maiduguri Teaching Hospital (UMTH), Nigeria between the periods of January 1993 and December 2002 . The case notes were retrieved and information about the age, sex, anatomical site and histological diagnosis were extracted. The duplicate copies of all histological reports and their corresponding original slides were retrieved and reviewed. Fresh sections were prepared in cases where the original slides could not be retrieved and stained with Haematoxyline and Eosin [H&E] and examined by light microscopy. The histological criteria used in the inclusion of cases as dermatofibrosarcoma protuberans was: spindle cells arranged in storiform pattern; high cellularity; monomorphic appearance and moderate to high mitotic activity. gross picture and photomicrograph were taken to demonstrate the lesion. the data were analysed in simple statistical tables. Results A total of 1177 cases of malignant tumours were recorded within the study period. There were 353 cases of skin cancers with 36(10.2%) histologically diagnosed as DFSP, which accounted for 3.05% of all cases of malignant tumours seen at the UMTH. Table 1 shows the age and sex distribution of DFSP.The peak age incidence is the 4th and 6th decades of life and it is rare before the 3rd and after the 7th decades of life. The age range was 20-73 years with a median of 37.6 years. The male female ratio was 2:1. In this report the trunk is the commonest site affected among 36 patients 17(48.8%) followed by the lower limbs 8(22.2%); upper limbs 6(16.7%); Head and Neck 3(8.4%); and 1(2.9%) case in the buttock. Discussion The incidence of DFSP is 10.2% of all cases of skin cancers in this study, which is slightly higher than 8.3% in the Lagos12series and much higher than 1.4% of all skin cancers in the Tanzania11 report. Similarly, DFSP has been reported among the Afro-Americans to constitute 12.1% of all skin cancers.8 DFSP was the 4th (8.8%) commonest skin cancer in Maiduguri which is preceded by squamous cell carcinoma (46.4%), Malignant melanoma (19.7%) and Kaposi`s sarcoma (15.4%) in a previous study from our centre.11 DFSP was observed to be common in the middle age and in this was similar to previous reports where the 4th and 6th decades of life were mostly affected The mean age was age of 37.6 years. Oliveira-Soares also documented similar findings in Portugal12. Some few cases were reported in infancy and childhood and could be as a result of the slow growing nature of the lesion. 10 The decrease in incidence of DFSP observed in late adulthood (7th decade of life) in this and other studies in an African population might due to the low life expectancy rate which swings around 49 years in most African countries. DFSP appears to have a greater preponderance for male in our study but prior reports present different incidences < 4:1 and 1.8:1 .710 The reason for the male preponderance is not clear and repeated minor trauma may be associated with a higher incidence in the more aggressive male counterpart. DFSP can occur at any site of the body. The tumour develops as a protuberant lesion; most often from the skin of the trunk as reported by these authors7 and in our present study it affected the trunk commonly 17(48.8%), followed by the lower limbs 8(22.9%). A comparison of anatomical distribution of DFSP in Americans, Tanzanians and the present study.show that the lower limb was the site most frequently involved in the Tanzania study.9 The head and neck was the 4th most frequently involved site in this study while the Tanzania series the 3rd most frequently involved site. Antecedent trauma has been implicated in the etiology of DFSP. Repeated trauma to the lower limbs and infection in peasant farmers causing DFSP has been suggested by Mbonde.11 Pricks from thorn may predispose to DFSP of the trunk and the hands observed by Mbonde11 Clinically DFSP presents as a slow growing firm plaque on the skin, resembling a keloids or hypertrophic scar at the initial stage, which is a strong clinical differential among the blacks that are prone to keloids or hypertrophic scars. Treatment should involve a wide local excision with skin grafting. local recurrence is a frequent complication if excision in inadequate . Fig.1 shows the excised recurrent lesion in a 40 year old patient and Fig.2 is the typical histological appearance of DFSP with the storiform pattern of the spindle shaped cells. Conclusion In conclusion DFSP is not an uncommon lesion in our environment. It commonly presents at the middle age and the trunk is the commonest site involved. Recurrence is high if the tumour is not completely excised and therefore a meticulous study of histological specimens presumably from wide surgical resection is necessary. Acknowledgement We wish to acknowledge Prof. Khalil and Dr Pindiga, for their contributions in reporting some of the slides, Mr. Simon and James for the technical work. We also thank Mr. Ibrahim of Veterinary Medicine Department, University of Maiduguri for the illustration. References:
Copyright 2006 - Nigerian Journal of Surgical Research The following images related to this document are available:Photo images[sr06014f1.jpg] [sr06014t1.jpg] [sr06014f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}