 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Nigerian Journal of Surgical Research, Vol. 8, No. 1-2 , 2006, pp. 77-80 Nipple-areolar complex (NAC) composite grafts in the Management of macromastia: Review of complications P. Agbenorku Plastic & burns surgery unit, Department of
surgery Komfoanokye Teaching Hospital Code Number: sr06015 Abstract Background:The
free graft of the nipple-areolar complex is almost like a “composite” graft.
This is because the skin of the areola and especially the nipple are usually
thicker than the case is in the usual full-thickness skin grafts (FTSG). In
traditional breast reductions, the nipple-areolar complex is located to its new
position by means of pedicle flaps. This, of course, enhances the proper
healing of the nipple-areolar complex (NAC). However, in the case of gigantic
breast hypertrophies, it is often not possible to carry the NAC on the long pedicle
flap. The NAC is therefore grafted as a free graft. Very often these grafts get
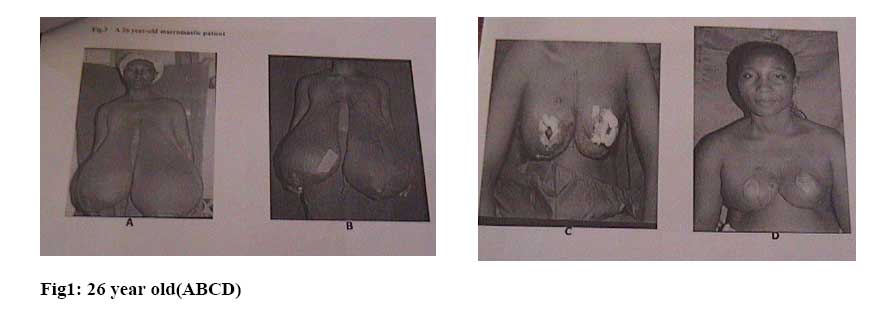
infected or simple become necrotic and part or whole of them may be lost. Key Words Nipple-areolar complex (NAC), Macromastia, Composite graft, Complications Introduction Gigantic breast hypertrophies often referred to as Macromastias are increasingly being seen at the Plastic Surgery Clinic of the Komfo Anokye Teaching Hospital (KATH), Kumasi. From 1997 till 2001 eighteen (18) such cases were recorded. All the patients except 2 had bilateral lesions. The parameters of six of such breasts are listed in Table [1]. In traditional breast reduction the nipple-areolar complex (NAC) is transported to its new “upper” position by a nipple-areolar dermal pedicle flap. Using this method for these “huge” macromastias the pedicled-flaps would be far beyond the recommended 20cm in length. To have a NAC on the new reconstructed breast mould a NAC “composite” free graft therefore has to be done. The survival or otherwise of the NAC full-thickness skin graft (FTSG) is influenced and determined by multiple factors. The NAC graft would require a sufficiently good blood supply in its recipient site for a successful “take”. The complications range from zero “take” to total (100%). In other words the complication/survival rate is determined by how much (%) of the NAC graft survives. Patients and Methods There were 18 patients of Macromastia seen at the KATH Plastic Surgery Clinic during the 5 years period 1997-2001 Eight of them were operated upon for bilateral lesions except one patient. Therefore in 8 patients 15 breasts with their respective NAC were reconstructed using modified subcutaneous mastectomies with immediate breast reconstruction using breast implants. In two of the patients implants were not used rather, the de-epithelized breast skin was folded into a skin envelope forming the new breast mould. For the prevention of recurrence of the lesions in the young girls (juvenile macromastia) all their breast tissues were practically excised. Breast implants were inserted beneath the pectoralis muscle, and covered with a skin envelope.The pre-determined appropriate new position of the NAC was then prepared for the NAC of same diameter, which was harvested at the beginning of the operation, and sutured into place. The technique of “tie over” dressing was used in fixing all the NAC grafts. As traditionally done, the grafts were examined (dressings changed) on the fifth post – operative day (post- op day). The initial results were assessed and recorded. The results were re-assessed on the 10th post OP day and then at day 20, 30 and then 40 posts OP days.. The final results were assessed at day 60 post OP (i.e. 2 months). The dressings were done using Vaseline/Paraffin oil gauze over the respective grafts and cleaning with normal saline solution. Results From January 1997 till December 2001, 18 macromastic patients were managed at the KATH Plastic Surgeryunit. Out of this, 8 were operated upon applying the technique previously described. Both breasts were operated in 7 patients and on one only in one patient. Thus 15 NAC “composite” free grafts were done on 8 patients. The age range of our patients was 12-28 with a median of 16 years. The final graft survival rate is shown in Table 2. The distance of the pathologic sited nipple is described in table1 for three patients for the left and right breasts Table 1 Breast parameters(cm)
Table II Survival rate of the NAC grafts
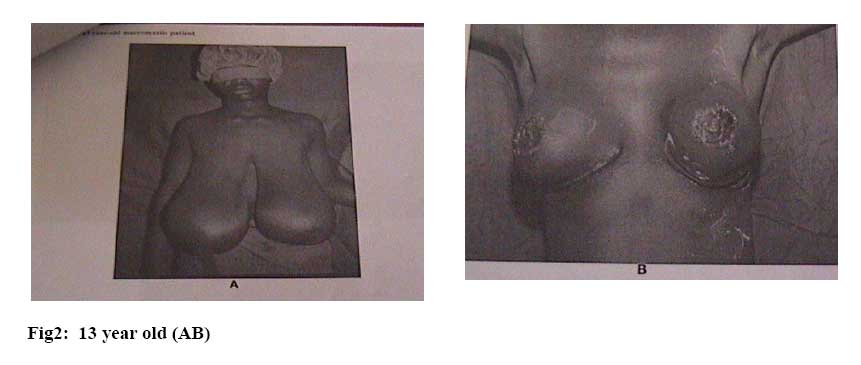
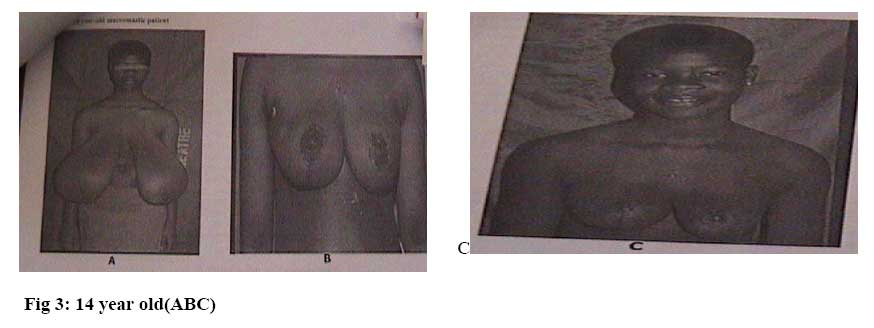
Fig. 1,2, and 3 Macromastic patients at various steps of reconstruction (Notation:ABCD) for each patient and outcome. Discussion Composite grafts generally consist of skin and another “harder” tissue such as cartilage and bone. In strict nomenclature nipple-areolar complex (NAC) belongs to the same tissue (skin) but because of the special “thickness” and structure the nipple could be considered as “hard” while the areolar may be said to be “soft” in comparison to the nipple. Owing to these structural differences between the nipple and areola the NAC could be considered as “composite”. The basic physiologic factors influencing and subsequently determining the survival of the composite graft is the “bridging phenomenon” principle. By this principle a portion of a skin graft overlying a small vascular area may survive by circulation from the greater portion of the graft which is on a well-vascularized bed. This phenomenon in case of the NAC graft is based on the fact that the collateral vessels connect the nipple to the vascularized areola and serves as a network for transporting an initial plasmatic circulation and later in growth of capillary buds. A similar process of bridging phenomenon occurs in the vascularization of skin-cartilage-skin composition grafts. The survival rate of these grafts range from 88 to22% as reported by various authors [3, 4]. Just as in the case of ordinary skin grafts the following are some of the multi-factorial combinations that affect and influence the survival rates of the grafts: [3, 4]. 1. Vascular/avascular recipient bed. A skin graft requires a sufficiently good blood supply in its recipient site for survival. 2. Vascularization of skin grafts 3. i Plasmatic imbibition. A skin graft begins to absorb a plasma-like fluid from the recipient bed almost immediately after a graft comes into contact with the bed. By the phenomenon of capillary action the sponge like structure of the graft capillary network absorbs fluid from the bed. The absorption of plasma-like fluid into the graft is called plasmatic imbibition. This often occurs over the first 48 hours after a graft. Within the early hours of the graft a fibrin network forms between the bed and graft resulting in a good hold of the skin to the bed. ii Inosculation of blood vessels A random inosculation of the vascular buds from the recipient bed with both arteries and veins into the graft. This happens within the first 48 hours after grafting. This process binds the graft to its recipient bed. 4. Contact of the skin graft and the recipient bed This is essential for good vascularization. The contact may be enhanced by compression dressing. 5. Presence of infection This will prevent good vascularization. The rate of complication and hence the survival/failure thus depends on the above listed factors. It was noted that the 3 patients that had complete loss of the NAC grafts had very thin skins. De-epitilization of these skins was almost difficult resulting in almost the skin being excised to the fatty tissue. The fatty tissue generally has poor vascularization and hence poor or zero take of graft. The 100% take grafts were those that had the maximum combination of the good factors. Conclusions The complications resulting in the partial/total take of NAC graft greatly depend on the combination of the multiple factors that influence the graft “take”.For the NAC composite graft the bridging phenomenon is the important factor in the initial survival of the nipple graft. In this series 10 out of the 15 NAC grafts had <50% survival rate Acknowledgement I sincerely thank the theatre staff, the anaesthetists, and all surgical colleagues, Prof. Lawrence Addae-Mensah and Dr. Eric P. Amaning who helped in managing some of these patients.References:
Copyright 2006 - Nigerian Journal of Surgical Research The following images related to this document are available:Photo images[sr06015f3.jpg] [sr06015f2.jpg] [sr06015f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}