 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Nigerian Journal of Surgical Research, Vol. 8, No. 3-4, Jul-Dec, 2006, pp. 103-110 Mini Review Current concepts in the management of anterior urethral strictures 1I. A. Mungadi and 2N. H. Mbibu 1Urology
Unit Department of Surgery Usmanu Danfodiyo University Teaching Hospital,
Sokoto and 2Ahmadu Bello University Teaching Hospital, Zaria
Nigeria
Code Number: sr06025 Abstract Objectives:
This review paper presents the current trends in the evaluation and treatment
of anterior urethral strictures. Stricture disease is recorded as one of the
oldest afflictions of mankind and even in the millennium; it is the one disease
associated with rapid turn over in treatment options and continuous evolution
of new options. The stricture is still a significant burden on the urologist
workload right from initiation of treatment and follows up. It may be
associated with significant morbidity and deteriorating quality of life and may
be frustrating to treat. Current trends are to discover a long lasting
satisfactory treatment suitable in most cases ‘the gold standard’.
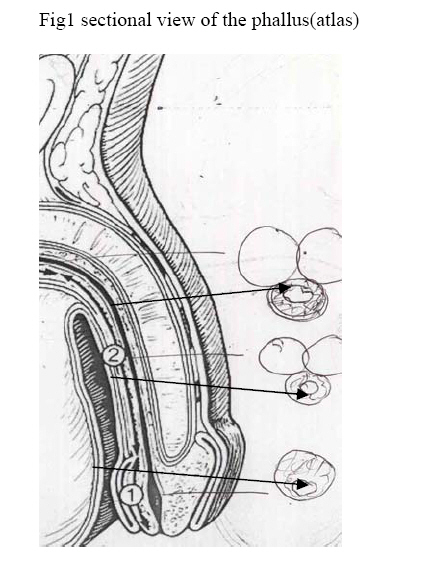
Introduction The anterior urethral stricture is an organic narrowing of the urethra caused by scarring of the urethral epithelium and the spongy erectile tissue of corpus spongiosum. Infection is still an important cause of most inflammation of the male urethra in the developing world and is most commonly due to Neisseria gonorrhea and infrequently caused by Chlamydia, lymphogranuloma venerum, tuberculosis and shistosomiasis1. The traumatic strictures are becoming increasingly important due to increase in civil violence and injury following road traffic accidents.The inflammatory reaction following trauma is limited and so the fibrosis that is responsible for stricture formation is localized and the stricture is short and formed within a short time from injury. Catheter induced strictures are not uncommon and pathophysiologically resemble trauma induced stricture. Malignant strictures are not common but may be formed in association with urethral and penile tumours. Stricture disease represents a significant part of the workload of the urologist. A multitude of methods have evolved aiming to cure these patients but non has proven to be suitable for all types of strictures. In the last decade advances in imaging and endoscopy and experience with oral mucosa (buccal, lip and lingual) have observed satisfactory reconstruction and outcome in the treatment of all types of anterior strictures on prolonged follow up. The versatility of the buccal mucosal graft represents an emerging threat to many available urethroplasty techniques1.This paper reviews the current trends in the management of the anterior urethral strictures. Anatomic definition The anterior urethra is that part of the urethra below the genitourinary membrane. It is about 15cm long in the adult and is divided into proximal bulbar and distal penile portions at the level of peno-scrotal junction 2. The urethra runs a central course through the corpus spongiosum in pendulous part of the phallus(fig 1(label2)but lies ventrally at the level of the glans penis fig 1(label1) in the expanded portion of the corpus spongiosus. In the bulbous region the urethra is displaced dorsally fig 1(label3) with the spongiosus thin dorsally and thick ventrally, fig 1. A dorsal stricturotomy/urethrotomy at this level as in the Barbagli technique is attended with minimal haemorrhage3. The urethra has a multiple supply of blood; proximally from the bulbar and urethral branches of pudendal artery and distally from the aborization of dorsal arteries of the penis in the glans penis 4.There are perforators and multiple circumflex arteries arising from corpus carvenosous. This rich blood supply allows safe division and mobilization of urethra during urethroplasty and relatively good survival of free grafts used on the urethra. The skin derives its blood from the external pudendal artery and the scrotal skin is supplied by both external and internal pudendal. These two sites have for a long time been scavenged for tissue to repair the stricture using very ingenious procedures. Fig 1. Urethra runs centrally (arrow 2) through the corpus spongiosus in the penile region but lies ventrally at the level of the glans (arrow1) in the expanded portion of the corpus spongiosus. In the bulbous region the urethra is displaced dorsally arrow 3) and the spongiosus is notably thin dorsally and thick ventrally. The cushion of the ventral part takes the first impact of a fall stride injury and may ameliorate the outcome.The bulbous urethra is richly populated by urethral glands which are sparsely distributed in the rest of the distal/anterior urethra. They are lined by columnar epithelium and are often described as looking flask like. They are more susceptible to infection compared to the more resilient urothelium or squamous over epithelial urethral lining. Niesseria gonorrhea appears to have an affinity for columnar epithelium where it brings about infective strictures. Aetio-pathogenesis Inflammation of the urethra and perineal trauma are the commonest cause of anterior urethral strictures. The so called congenital strictures occur in teenage boys and young adults with no history of trauma or infection 5. These short strictures occur between the middle and the proximal thirds of the bulbar urethra and are related to the Cobb’s Collar and are often difficult to distinguish from type 111 posterior valves. 6-9 . Failed hypospadias repair is an important cause of anterior strictures in children’. These strictures may be located at the external meatus or may be complex and long involving the whole anterior urethra. Repeated failed repair has previously been the commonest cause of ‘stricture cripples 10. Balanitis Xerotica obliterans (BXO) the genital forms of Lichen Sclerosis initially affect the prepuce and glans, but can extend to involve the anterior urethra up to the bulbar is not a common encounter in Africans 11,12. This disease is not simply an obliterating balanitis and Lichen Sclerosis is the preferred description. Evaluation Thoughtful evaluation is important in the outcome of urethroplasty and has to planned and done meticulously . The first occasion of urethroplasty is commonly the best and the aim is to elect the best option for the situation. Patients initial evaluation should aim at the total assessment to estimate the magnitude of the disease. Some present with peri-urethral abscess, perineal sepsis or Watering Can Perineum. Some may present in retention of urine from other causes likeacute prostatitis, and stone disease. There may be history of poorly treated chronic urethritis ,urinary tracttrauma and instrumentation or surgery. Initial assessment may reveal purulent urethral discharge, induration of the multiple urethrocutaneous fistulous perineal tracts draining pus and urine. Rarely these tracts may be malignant fistulae. Its common to see these patients presenting after a long time with a superpubic catheter to divert urine previously due to retained urine or for a fistula ridden perineum. They would have defaulted or are in the waiting list. Urethrogram, urethroscopy and ultrasonography are employed to determine the location length and density of spongiofibrosis. Static urethrogram are commonly used but a dynamic study gives a better definition 16. A retrograde and voiding urethrograms in lateral oblique position give good definition of anterior strictures. It is best to delay urethrography in patients with markedly inflamed urethra and acute Watering Can Perineum to avoid extravasations of contrast. With flexible urethroscopy the stricture can be visualised and its distensibility assessed. A flexible pediatric cystoscope can negotiate narrowstrictures without the need for dilatation. Ultrasonography and Magnetic Resonance Imaging (MRI) are increasing being employed to determine the degree of spongiofibrosis. A lubricating jelly or saline is used to distend the urethra and real time sonographic scanning performed. Morey and McAninch found that ultrasonography more accurately defines the extent of spongiofibrosis in bulbar urethra 17. Spongiofibrosis manifest as lack of urethral distensibility. Sonographic staging before treatment of complex or reoperative anterior strictures was found useful in elucidating complicating features such as calculi, urethral hair and stent encrustation which may be useful in guiding reconstruction 18. MRI may also provide adjunct information about spongiofibrosis, diverticular formation, tumour and pelvic anatomy that may not be obtainable with other modalities 19. At present, MRI is more relevant in patients with traumatic posterior urethral stricture to determine the extent of prostato-membranous and pelvic distortion 20. The final evaluation of stricture can only be made during surgery assisted by endoscopy and bougienage 16. A proximal involved segment may appear deceptively normal due to hydro dilation during high pressure voiding. This segment constrict if not included in repairs. Jordan and Schlossberg found it useful to place a suprapubic tube for 6 to 8 weeks to determine the tendency for such hydro dilated segment to constrict 16. Treatment Role of Dilatation The aim of dilatation is to dynamically stretch the scar and if scaring is limited to epithelium, then dilatation could cure the patient. Inflammatory strictures are still common in developing countries 21-24. In these patients, there is always some degree of spongiofibrosis limiting cure by dilations. Dilatation is not a procedure to be relegated to the inexperienced. It should not lead to epithelial injury and unless undertaken with gentleness can lead to additional spongiofibrosis. Stretching destroys muscular fibers leading to haemorrhage and more scaring 25, 26. The ancient Egyptians used wooden tubes to dilate strictures 27. But now catheters, metal bougies and balloons are employed. Dilatation should be stopped at 24 Fr 27.Balloon dilatation is preferable to bougienage especially when strictures are eccentric because of the differences in physical properties of the strictures28. Balloon dilatation is performed under local anaesthesia. With the help of a guide wire placed in the bladder the balloon is positioned in the stricture region, filled with contrast and inflated under radiologic guidance 29. The success rates of balloon dilatation at 12 months are 40% to 60% 30. Longitudinal forces applied during dilatation with metals or catheter can lead to mucous membrane trauma. The eccentrically active forces of balloon dilatation are less traumatic 31. Visual Internal Urethrotomy Urethrotomy is a full thickness incision through the scar performed at 12 O’clock position using an optical direct vision urethrotome. A 12 o’clock urethrotomy avoids damage to the cavernous nerves which are at 5 and 7 o’clock to the prostatic urethra, 3 and 9 o’clock to the membranous and 11 and 1 o’clock to the bulbar urethra 29. The penile urethra is not related to cavernous nerves. Following adequate urethrotomy the urethra should admit size 24 Fr catheter easily. The urethral catheter should be removed after 3 days. Using pack of 15ml/s as the lower limit of treatment failure, Pansadoro and Emiliozzi found a recurrence rate of 58% in bulbar, 84% in penile and an overall recurrence rate of 68% on 1st urethrotomy. These were a long term follow-up of a large series of 225 patients. They suggested that single strictures, less than 1 cure and in the bulbar region which had a success rate of 77% are the optimal strictures for urethrotomy as the first line. Several studies have shown that urethrotomy offers no advantage over dilatation33-35.A single recurrence following urethrotomy should be treated with other procedures since a second urethrotomy is of limited value even for palliation and a third repeated urethrotomy of no value 34,36. Intralesional corticosteroid injection in combination with urethrotomy has been tried to reduce recurrence but there are no randomized study to support the practice 37. Clean intermittent self catheterization once a week could reduce recurrence rate from 68% to 19% following internal urethrotomy37.Being subjected to intermittent self catheterization is far from satisfactory when cure is the goal. Laser can be employed to effect urethrotomy. The advantage of laser is clean cutting combined with haemostasis. Neodymium-YAG, Argon, Holmium and Calcium-Titanyl-Phosphate(KTP) lasers are in current usage 39-42. Given the high cost of lasers they have no clinical advantage over conventional urethrotomy at the moment 31. Stents Stents were first used in vascular surgery to reduce endoluminal restricturing after balloon dilatation 43. Metal stents were first used in the urethra by Fabian 44. Essentially, stents are self expanding meshwork from biocompatible materials like stainless steel, nitinol or titan 31. Non metallic materials such as polyurethane are used for temporary stenting 45.Stents are placed endoscopically at least 0.5cm from the external sphincter to avoid incontinence. In the anterior urethra the use of stents is limited to but strictures. The mobility of the pendulous urethra makes it unsuitable for stenting. Studies reporting 90% success for stenting have short follow-up 46-48. However, Milroy and Allen reported that 84% of their 50 patients had open urethral lumen 5 years after implantation 49. The complications of stenting are displacement, perineal pain, incontinence, recurrent urinary tract infection, encrustation haematuria and stimulation of spongiofibrosis 48 . Urethroplasty Dilatation, urethrotomy and stenting have limited results and largely palliative outcome .Therefore, urethroplasty is the standard curative treatment for most urethral strictures.Repair may be effected by excision and end to end anastomosis or by urethral substitution The choice of procedure depends on the type and location of stricture. In general, strictures in the bulbar urethra of 2cm or less are treated by excision and spatulated end to end anastomosis 50. End to end anastomosis of penile strictures or bulbar strictures of more than 3cm may lead to shortening of the urethra and penile curvature at erection 51. These strictures are treated by substitution urethroplasty using vacularised genital skin or free grafts. Augmented anastomotic repair should be considered when a 2-3cm bulbar stricture excision is necessary 52.In this technique, the stricture is excised and dorsally spatulated. The dorsal spatulation is patched but the ventral circumference is anastomosed. This ensures a wide and tension free anastomosis Anastomotic Urethroplasty The success rate of anastomotic urethroplasty is in excess of 90% which is sustained on the long term 53. The bulbar urethra is elastic and can be mobilized from its attachment within the bulbospongiosus allowing 2-4cm of stretch to overcome a defect, but 1cm of this length is also lost to spatulation 10. The key to successful anastomotic repair are adequate mobilization and tension free spatulated anastomosis, (fig 2). Spatulation is important in overcoming any narrowing that may occur at the repair siteThe lowest re-stricture rate and the lowest complication rate are achieved with anastomotic urethroplasty and this should be performed when ever possible 53-56. Substitution Urethroplasty Substitution urethroplasty can be performed using either vascularised genital skin or free graft. Flaps have been regarded to be more reliable because they carry their blood supply. The comprehensive description of penile microcirculation by Quartey led to the dominance of flap in 1980’s and early 1990’s 57-59. This seemed theoretical since current studies could not establish superiority of flaps over grafts in terms of re-stricture rate 60. Flap reconstruction is time consuming, the dissection extensive and redeployment of dartos tend to cause penile deforming and scarring. With the advent of buccal mucosa there is renaissance of the graft in urethral reconstruction. Flaps are still favoured in some revision surgeries and in any condition that may interfere with the ability of graft take such as radiotherapy, peripheral vascular disease or persistent local infection 61. Therefore, the reconstructive urologist must be familiar with both grafts and various flap repairs. Buccal mucosa graft urethroplasty. Buccal mucosa graft (BMG) gas emerged as reliable urethral substitute with long term results comparable or superior to penile flaps 50,52,62-68. Buccal mucosa graft is easy to harvest and trim, more resistant to infection than skin, flexible and has thick lamina propria and excellent microvasculature favourable for graft inosculation 16. The natural location of BMG in oral environment favours easy adaptability in the urethral passage, thus giving long term results 62,63,69-70. Buccal mucosa is the recommended substitute in patients with lichen sclerosis (BXO) as it is not involved in this provess71. Buccal mucosa is now the established materials of choice for patch repair of the bulbar urethra 68. The technique of BMG repair has, gradually, outmoded the use of bladder mucosa or appendix for anterior urethral repair. Potential Buccal mucosa donor site are the inner check, the lower lip and under surface of the tongue. The graft may be applied ventrally, in an augmented anastomotic fashion (figure 3), dorsally (figure 4) or for staged repair. Dorsal placement (Barbagli technique) has found favor recently 65,67,72-74. This radical change in urethral substitute repositioning ensures adequate graft bed support provided by the corporal bodies and virtually eliminates graft ballooning and biventricular formation The consequent post void dribbling and ejaculatory dysfunction (scanty ejaculation) are therefore avoided. There appears to be no difference in restricture rate between a dorsally and ventrally placed BMG 6 ,75 Endourethroplasty may be performed where urethrotomy alone is inadequate for complex or recurrent strictures. This procedure involves preparation of free graft, endoscopic delivery and fixation in the stricture bed with the aid of balloon catheters or a novel suturing technique described by Naude 87. Endourethroplasty has not gained wide acceptance and the number of studies is still limited. The future of anterior urethral stricture surgery With refinement of techniques, the scope of endoscopic urethroplasty may broaden. This will appeal to patients seeing that no penile dissections are required. Success of endoscopic substitute replacement requires increasing use of MRI and high resolution Ultrasonography to accurately define the extent of spongiofibrosis and to properly select patients.The future of anterior urethral substitutes seems to lie on Tissue Engineering. Currently buccal mucosa can be cultured and seeded to a scaffold for urethral replacement 89 90. This will obviate the need for tissue transfer in patients with long and complex strictures. With tissue engineering we are no longer limited by the quantity or quality of urethral substitutes available in any given patient. References
Copyright 2006 - Nigerian Journal of Surgical Research The following images related to this document are available:Photo images[sr06025f1.jpg] [sr06025f2.jpg] [sr06025f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}