 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Nigerian Journal of Surgical Research, Vol. 8, No. 3-4, Jul-Dec, 2006, pp. 111-114 The incidence of cancer in women presenting with bloody nipple discharge at a specialist breast clinic M Ohene-Yeboah Department of Surgery School of Medical Sciences Kwame
Nkrumah University of Science and Technology University Post Office Kumasi Ghana
West Africa, Code Number: sr06026 Abstract Objectives: To determine the frequency of breast cancer in
patients presenting with bloody nipple discharge at the Komfo Anokye
Teaching Hospital Breast Care Centre (KATH –BCC) Kumasi.
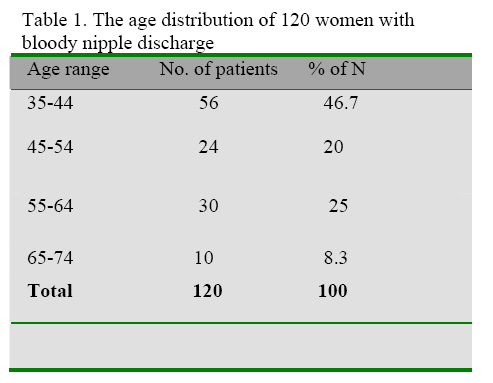
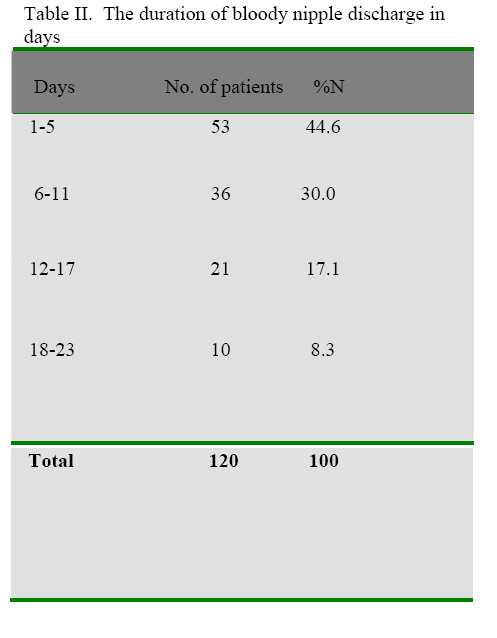
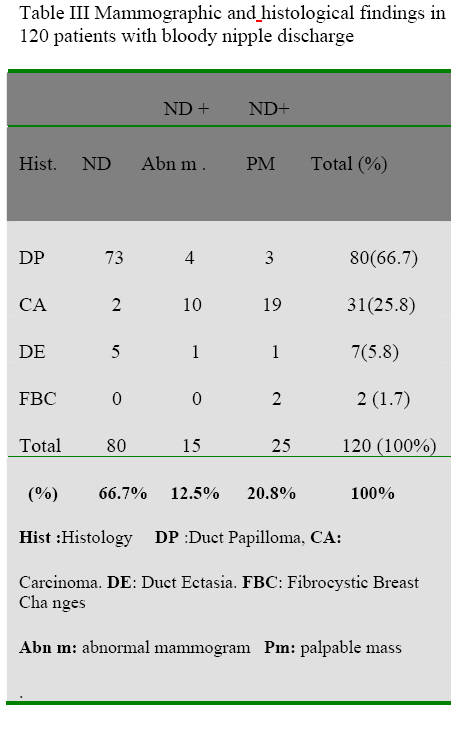
Introduction Nipple discharge (ND) is an important presenting complaint in women attending breast clinics woridwide1-3. It is reported in up to 10% of patients with breast disease.1-5. The surgical importance of the ND is related to the reported association with carcinoma of the breast; which varies between 1.0 – 72.7 percent depending on the series1-6. Until the 1950’s nipple discharges especially when bloody, were regarded as definitely indicative of carcinoma of the breast. Many unnecessary mastectomies were performed without obtaining histological diagnosis6-11. Over the years this attitude has changed and now nipple discharges are investigated with clinical history, physical examination, occult blood studies, cytology of discharges, breast ultrasonography, mammography, ductography, and recently breast MRI scan studies as indicated 1-10 There have been many previous reports on the surgical treatment of the various types of nipple discharges.1-6. This report is on 120 patients who were seen and treated for bloody nipple discharge at the Komfo Anokye Teaching Hospital between January 1998 and July 2005. The aim is to determine the frequency of cancer in this group of Ghanaian women. Patients and Methods At the Komfo Anokye Teaching Hospital all patients with breast complaints were evaluated at the general surgical outpatient until July 2004 when the Komfo Anokye Teaching Hospital Breast Care Centre (KATH – BCC) was established. A review of all patients seen by a single surgical unit and operated on for bloody nipple discharge was done for the period of six and a half years (between January 1998 and June 2004). From July 2004 to December 2005 (18 months), all patients seen at the KATH – BCC complaining of a bloody nipple discharge were prospectively studied. The study inclusion criteria were a bloody nipple discharge (confirmed by the gauze sponge test2) that was unilateral, spontaneous, had been present for 3 days or more and arose from a single easily identifiable duct. All the patients who satisfied the inclusion criteria provided the material for the study. A detailed clinical history was taken from each patient followed with a clinical breast examination (CBE). A mammogram was performed for each patient. All the patients in the study were treated by excising the discharging ducts. The excised ducts provided the material for biopsy and thus the histology of the cause of the bloody nipple discharge. In patients in whom there is a breast mass in addition to the bloody ND the mass was also excised for histological examination. Data recorded included the age of the patients, the duration of the discharge, whether the discharge was spontaneous or provoked and whether it was unilateral or bilateral. In addition the outcome of the clinical examination, noting the presence of a lump and whether there was a single or multiple duct discharge was recorded. The mammographic findings in all the patients were recorded. The histology of the excised ducts as well as of the excised lumps was also recorded. Cytological examinations of the bloody nipple discharge and ductograms were not done as these services are not available in our institution. Follow up was arranged for between 1 and 3 months. Further treatment was offered as appropriate and according to the histologic diagnosis of the nipple discharge. Results A total of 120 women met the study inclusion criteria. Ninety- six patients were in the retrospective and 24 in the prospective data. The ages ranged from 35 – 65 years. The 10 – year age distribution of the 120 women is shown in Table I. The duration of the discharge in the 120 women is shown in Table II. All the patients studied had unilateral and spontaneous single duct discharges. A palpable mass (within 2cm of the nipple) was detected in 25 women (20.8 %). Of the 120 patients for whom a mammogram was obtained 15 patients (12.5%) revealed mammographic abnormalities. In 105 (87.5%) patients the mammogram was normal. Of the 120 specimens of excised ducts the histology in 80 (60.7%) was Duct Papilloma (DP), 31(25.8%) Carcinoma (CA), 7(5.8%) Duct Ectasia (DE). In 2 specimens the ducts were histologically normal. In these two patients the bloody nipple discharge was associated with breast lumps. The histology of both lumps was fibrocystic breast disease (FBC). Of the 25 lumps that were present in addition to a bloody nipple discharge the histology of 19 was CA, 3 DP, 2 FBC and 1 DE Table III shows the histological distribution of the excised breast ducts in relation to the clinical findings of an associated mass, mammogram abnormalities or bloody discharge only. The mean age of the 80 patients diagnosed with duct Papilloma was 40.2, range 35- 57 years. Of a total of 31 (25.8%) carcinomas diagnosed 19 (61.3%) were found in patients with a palpable mass, 10 (32.2%) in patients with abnormal mammogram and 2 (6.5 %) in patients with bloody nipple discharge only (Table I) The mean age of the 31 patients with cancers was 52.4 range 35 - 65 years. Other histological diagnoses were duct Ectasia in 7 and fibrocystic changes in 2 women. The causes of single duct bloody nipple discharge are shown in Table III Discussion Nearly half (46.7%) of the patients studied for bloody ND were aged between 35 and 44 years (Table I). Previous studies indicate that the largest number of patients with nipple discharges that may be due to cancer is in the fourth decade of life1-3. Majority of the patients we studied (91.7 %) presented within 2 weeks of noticing a bloody nipple discharge (Table II. This is significantly earlier than the 12.5 11 weeks mean presentation time for breast lumps noted at the KATH –BCC (, p < 0. 001.) Many women experience considerable anxiety and distress and are often very alarmed on noticing that the nipple is discharging blood.1-4.This reaction may explain the finding that most of these patients seek medical help much earlier than they do for painless breast lumps. 2 Cancer was detected in 25.8% of the patients we studied (Table III). This figure is similar to the finding of Leis who reported that 27.5% of the patients operated upon for bloody nipple discharges had cancer2. Majority of the cancers 19/31 (61.3%) in our series were found in patients who had a palpable breast mass associated with the bloody nipple discharge (Table III). The presence of a palpable lump in addition to a bloody nipple discharge has been noted to be associated with an increased risk of breast cancer1-6,12-,14 In this study a palpable mass was detected in 25 (20.8%) of the patients presenting with a bloody nipple discharge and 19 (76.0%) of these 25 patients were found to have breast cancer (Table III). Practitioners and surgeons evaluating women with bloody nipple discharges need to establish the histology of any associated lump or lumps as many of these may be cancerous. Previous published data indicates the usefulness of the mammogram in diagnosing invasive papillary carcinoma in patients presenting with bloody nipple discharge.3,13-14. In our series mammogram abnormalities, were detected in a third of patients diagnosed with cancer (Table III) Duct Papilloma was the most common (66.7%) histological lesion diagnosed and accounted for 73 or 91.3% of the 80 patients who presented with bloody nipple discharge alone with no palpable mass or abnormal mammographic findings. (Table III). This finding is similar to previously reported series where Duct Papilloma has been found in the majority of patients presenting with a bloody ND1-4. These solitary centrally located papillomas are usually found in the subareolar location within the major ducts and as in this study (Table III) typically present as a bloody nipple discharge7. As noted in previous studies, these solitary central papillomas have no malignant potential7. Duct ectasia and fibrocystic disease of the breast (5.8% and 1.7 % respectively) are other benign diseases of the breast that may present as a bloody nipple discharge (Table III). Duct ectasia presented mainly as a bloody nipple discharge alone and the 2 cases of fibrocystic of the breast presented with a palpable mass (Table III). Mammography is often negative in patients with central papillomas1,7,,12-14. In our series only 5% of the papillomas were found in patients with abnormal mammographic findings. Mammography abnormalities that may be seen suggestive of the diagnosis of duct Papilloma include subareolar nodules and or subareolar amorphous coarse calcifications7 .Ductography is the imaging of choice in the detection of central papillomas5. The involved duct is often dilated and the Papilloma is identified as an intraluminal filling defect7. It is expected that provision of ductography facilities in our institution should provide for the diagnosis of duct papillomas. In 3 (3.8 %) of the 80 patients diagnosed with papillomas in this series, the bloody nipple discharge was associated with the presence of a clinically palpable mass (Table III). This finding compares with published data, in which 1 out of 37 patients with histologically proven central duct Papilloma had a palpable mass7. Many patients with proven central papillomas do not have a palpable mass6-7. However the peripheral Papilloma arising from the terminal duct lobular unit more often presents with a palpable mass12-13 and nipple discharge is less often seen occurring in less than 20% of these patients with peripheral papillomas7,12-13. Conclusion. This paper notes that in Ghanaian women, spontaneous and unilateral single duct bloody nipple discharges are frequently associated with cancer. The presence of a palpable mass and abnormal mammography are useful indicators of carcinoma in these women. References
The following images related to this document are available:Photo images[sr06026t2.jpg] [sr06026t1.jpg] [sr06026t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}