 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Nigerian Journal of Surgical Research, Vol. 8, No. 3-4, Jul-Dec, 2006, pp. 123-127 Human Bites of the Face with Tissue Losses in Cosmopolitan Northern Nigeria 1M.E Asuku, 2D.S. Adeola , 2A.C Obiadazie and 2C.N. Ononiwu 1Division of Plastic Surgery, Department of Surgery 2Department
of Maxillo-Facial Surgery Ahmadu Bello University Teaching Hospital, Zaria
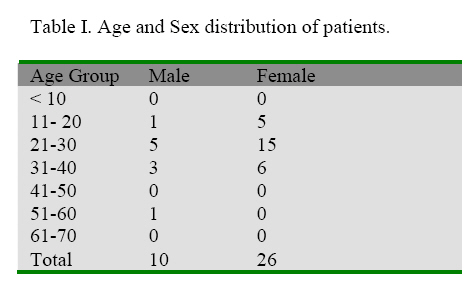
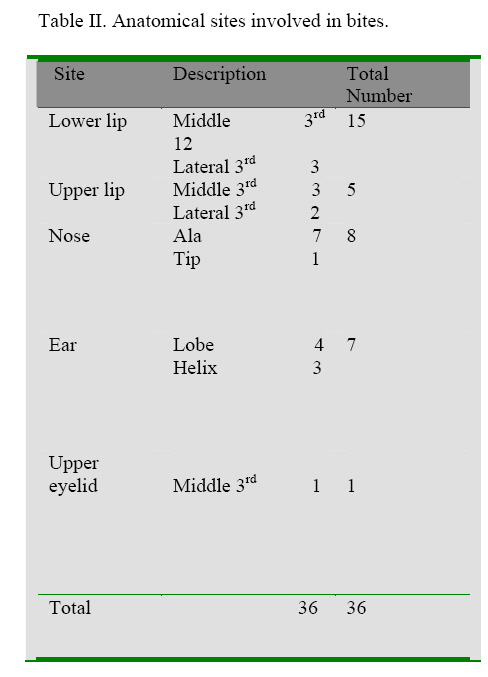
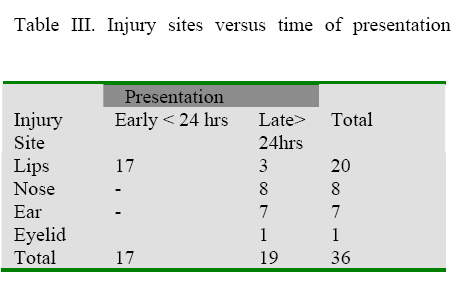
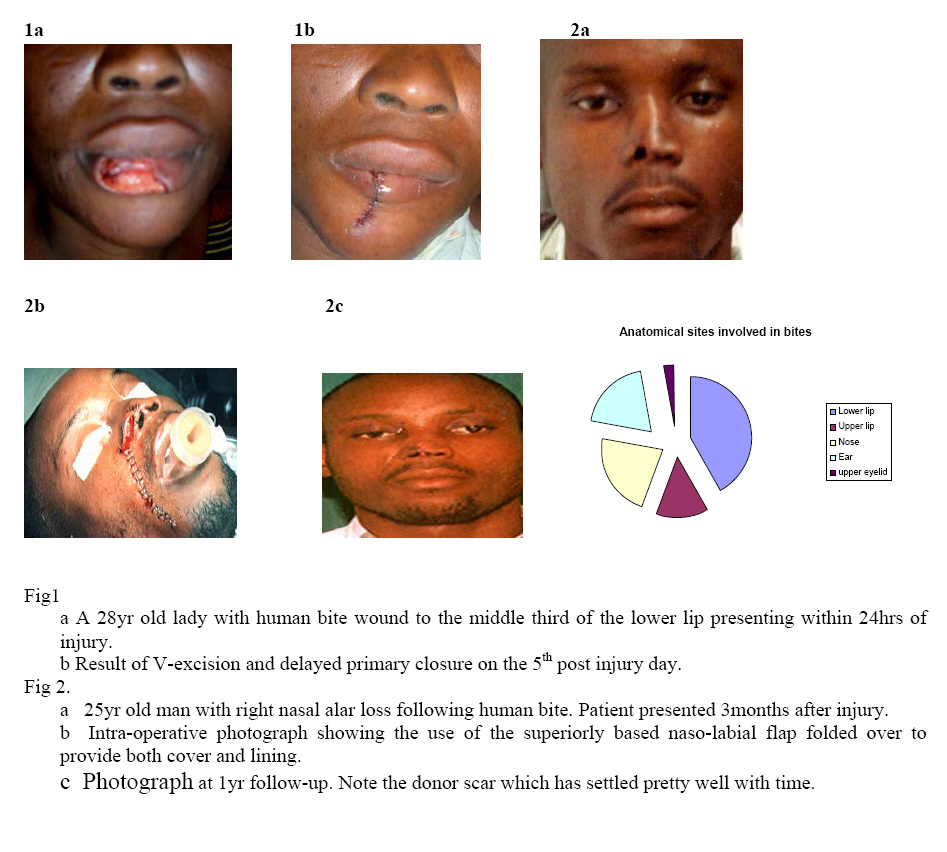
Code Number: sr06029 Abstract A retrospective series of thirty-six cases of human bites to the face with tissue losses requiring reconstruction during a five-year period, January 1999 to December 2003 is presented. The unmarried female in her third decade dominated both as victim and assailant in incidences related to love affairs and love gone sour. The middle third of the lower lip was the most commonly bitten part with a majority of these presenting early. Copious larvage under broad-spectrum systemic antibiotic cover as well as anti-tetanus regimen allowed delayed primary repair in the first week of injury in a majority of the patients. Our reconstructive armamentarium included V-excisions and closure for lip defects, the superiorly based naso-labial flap for nasal ala defects and the retro-auricular tubed flap for helical rim and ear-lobe defects. Outcome was generally satisfactory though a longer follow-up data is desirable. Experience with hypertrophic scarring and keloid formation in our patient population continues to be a major factor in the choice of reconstructive techniques in our regional practice. Key words: Human bite, Tissue loss, Reconstructive armamentarium. Materials and Methods A retrospective study of patients who have suffered human bites with tissue losses requiring reconstruction at the Ahmadu Bello University Teaching Hospital Kaduna from January 1999 to December 2003 was conducted. Thirty-six patients were included while two patients that declined reconstruction for defects they considered acceptable following wound contraction were excluded. The patients were analyzed for age, sex, site, occupation and circumstances of injury including particulars of the assailant where available. The time interval between injury and presentation, surgical management and disposition were also analyzed. Results The male: female ratio was 1: 2.6, with females in the age group 21-30 constituting the majority (41.7%). The oldest patient in the series is a 58yr old man who lost the tip of his nose as a result of a bite by his drunkard son (Table I). The middle third of the lower lip is by far the most commonly bitten (41.7%) followed by bites to the ala of the nose. It is noteworthy that though there were a few cases of multiple bites, none of these had tissue loss in more than one of the bite sites (Table II). All the patients were of poor socio-economic status with all but two of the men receiving their bites from commercial sex workers. Fifty percent of the patients presented within 24hrs of injury, interestingly lip losses constituted the entire bulk of patients that presented within 24hrs of injury (Table III). For those presenting early, our treatment protocol includes copious irrigation with water and normal saline as well as broad spectrum combination systemic antibiotic cover and anti-tetanus regimen. Simple V-excision and closure sufficed as a reconstructive tool in a majority of those who sustained lip injury. Most injuries to complexly contoured structures such as the nose and ear presented late making delayed reconstruction a logical choice. We used the retro-auricular flap for most reconstruction of the ear lobe and helix while the superiorly based naso-labial flap constituted our workhorse in the reconstruction of nasal ala losses. The overall outcome was satisfactory as all the patients expressed satisfaction and had returned to their pre-injury vocations at two years follow-up. Two post-operative complications were recorded. One patient had partial necrosis at the tip of a naso-labial flap, which was folded over to provide lining while the otherr had wound dehiscence following wedge excision and closure of a helical defect. Both complications were managed conservatively. Discussion Human bites are serious injuries that may result in infection, loss of function and gross disfigurement. Infection from oral contaminants, tissue damage, and difficult surgical reconstruction make the management of human bite injuries a challenge 1.The goals of reconstructive surgery include achieving wound closure, restoring anatomic landmarks and minimizing surgical revisions as well as psychological trauma 2. Accurate assessment of tissue loss and due consideration of reconstructive options are crucial to a successful outcome. The head and neck region is perhaps only second to the hand as a target in acts of deliberate human bites 3. In the traditional African society, the incidence of this act varies widely being strongly influenced by cultural values 3-5. In the rural Hausa-Fulani culture of Northern Nigeria, human bite as a means of assault during conflicts is a rarity as it is considered a disgraceful act of weakness. However, in the cosmopolitan cities, the influence of other cultures is brought to bear and the challenges of having to reconstruct defects resulting from human bites are no longer strange to the reconstructive surgeon practicing in Northern Nigeria. In this series, thirty-six cases of human bites with tissue loss requiring reconstruction during a five-year period were managed. This is a low incidence when compared to similar studies from other parts of Nigeria. Datubo-Brown in 1988 in a similar survey reported a series of 24 patients in a two-year period in Port-Harcourt 3. Iregbulem working in Enugu in 1979 reported 16 cases of human bite with lower lip losses in a two-year period 4 while Uchendu 6 working in the same center a decade later reported a five-year series consisting of 37 cases of human bite to the lip and tissue loss. In the western world human bites are more frequently encountered in institutions for the care of the developmentally disabled individuals as reported by Lindsey and colleagues 7.We noted that unmarried females in the age group 21-30 dominated both as victims and assailant in incidences related to love affairs and love gone sour. This is consistent with the findings by other authors 3, 5The expression ‘snatched lover’ featured prominently in discussions with the patients and the few instances where assailants were available to us as was the case in a pair of ladies who had bitten each other in a scuffle over a common lover. We share Datubo-Brown’s opinion that the high premium placed on marriage makes the average unexposed African lady restless and anxious when she is still single by her third decade. Furthermore, that the sophisticated and exposed African lady must have a more civilized way of dealing with such issues as suggested by Datubo-Brown is borne in the fact that no such lady featured in our series either as a victim or assailant. Our series show that the lower lip was most prone to being bitten; this is consistent with the findings of previous works 8-10. This may be explained simply as a result of the anatomical position of the lower lip. It is therefore no surprise that it is indeed the middle third of the lip which stands out, that is most often bitten. The profusion of lip volume in the African while contributing to its increased risk of getting bitten on the one hand, it on the other hand reduces the challenges of reconstruction when tissue loss is less than 50%. In our series, loss of nasal ala was second in frequency. We observed that the patients that sustained injury to complexly contoured structures such as the nose and ear tended to present relatively later when compared to the patients that suffered lip losses. This trend is accounted for in part by the fact that the victims conceive such injuries as capable of resulting in severe and permanent disfigurement and as such the pursuit of criminal justice is given precedence ahead of presentation at the hospital. Our management protocol for the patients presenting early included copious irrigation with water or isotonic saline, parenteral broad spectrum antibiotic cover usually consisting a third or fourth generation cephalosporin and metronidazole targeted at anaerobes. Tetanus toxoid was routinely given to all the patients as human bite wounds are considered as severely contaminated wounds, moreover the immunization status of most of our patients is usually unavailable. Débridement was undertaken early but closure was delayed for a couple of days during which frequent dressing changes were undertaken. The adequacy of such management protocol have been attested to by several earlier surveys on the management of human bite with tissue losses 3-6, 8, 9. Following extensive bacteriological studies on 36 patients with human bites to the face, Agrawal and colleagues inferred that infections actually arise as a result of secondary colonization of the devitalized bite edge tissue. They therefore recommended the prompt débridement or excision of the bite wound as a prerequisite to managing the bite wound in the same manner as facial wounds of other etiologies 8. Similarly, Earley and colleagues cited the excellent vascularity of the face as well as the use of prophylactic antibiotics as factors that favor delayed primary closure of human bite wounds to the face 9.Our experience with hypertrophic scarring and keloid formation among our patient population continue to govern our choice of reconstructive techniques. We utilized V-excisions in our patients with lip losses as this allows layered closure with satisfactory results. The only patient in our series that had a cheek advancement flap presented late with a 20% lateral third upper lip defect. The challenge continues to be the reconstruction of complexly contoured structures such as the nose and ear. We favor the superiorly based naso-labial flap for the reconstruction of the ala of the nose. Its attributes include the ability to provide both cover and lining and the fact that the donor scar tends to settle pretty well with time even when initially objectionable. A case of partial flap tip loss, which was managed conservatively, was however encountered with the use of this technique. The multi-staged retro-auricular tubed flap was used in reconstructing earlobe losses and one helical loss with satisfactory outcome. This technique, though obsolete, has continued to provide solace to reconstructive surgical practice in regions where microsurgical facilities are yet to find routine use 11-13. Two patients with less extensive helical losses had wedge excision and closure in the fourth and seventh week of injury. One of these developed wound dehiscence probably due to excessive tension suggesting an error in our choice of reconstructive technique. The wound was allowed to heal secondarily and the outcome was just acceptable. Human bite to the eyelid is an extremely rare injury with the upper lid at a slightly higher risk. The challenges of reconstruction depend on the fullness and extent of tissue loss and whether or not the avulsed part is available for reconstruction 14. We encountered one case that had partial upper lid loss resulting in primary ectropion. The outcome following release of the contracted lid and over correction with split-thickness skin graft was satisfactory. Whereas there are sufficient data to substantiate a higher incidence of infection in human bite wounds when compared to other forms of trauma in our regional practice 6, 10our series lends support to the admonition that routine anti-microbial prophylaxis and aggressive surgical intervention are key to satisfactory outcome. We are aware that in some other regions where infection is not an issue, conservative management of human bite wounds has been advocated. Rhee and colleagues observed that healing by secondary intention may produce optimal results particularly in younger patients following significant traumatic avulsion involving delicate anatomic landmarks such as the vermilion and the peri-oral composite soft tissue 15. Despite the fact that the literature is replete with reports on re-implantation of amputated parts, there is as yet scanty mention of re-implantation of small pieces of facial tissue. This is perhaps due to the extremely small size of the arteries as well as a lack of suitable veins for drainage 16. However, as the technique of microsurgery continues to witness milestone technological advancement, the next decade may witness anecdotal reports on re-implantation of bitten facial parts. References.
Copyright 2006 - Nigerian Journal of Surgical Research The following images related to this document are available:Photo images[sr06029t3.jpg] [sr06029t4.jpg] [sr06029f1-2.jpg] [sr06029t2.jpg] [sr06029t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}