 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Nigerian Journal of Surgical Research, Vol. 8, No. 3-4, Jul-Dec, 2006, pp. 128-131 Pattern of skeletal metastases from breast cancer in an Asian population 1 S.A Adewuyi, 2N.D Chom, 3M Humera and 4M.O.A Samaila 1. Radiotherapy and Oncology Center, A. B. U. Teaching
Hospital, Zaria Code Number: sr06030 Abstract Objectives:: To evaluate the pattern of
skeletal metastases from breast carcinoma in an Asian population. To study the
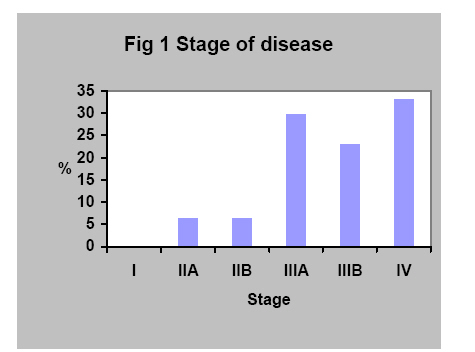
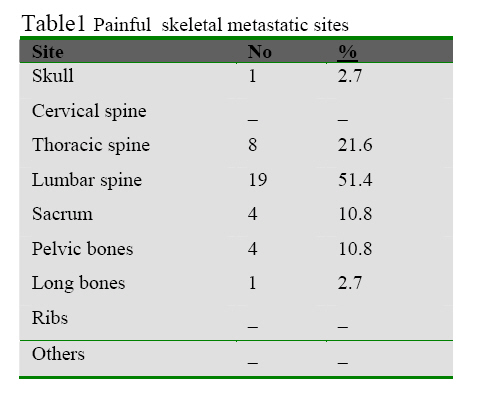
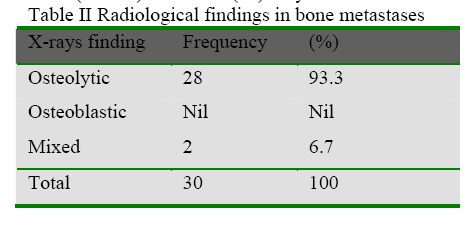
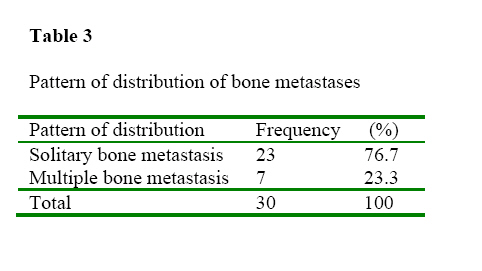
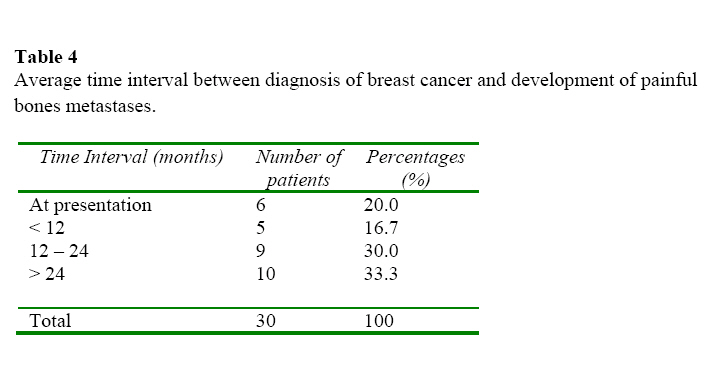
radiological pattern and distribution of bone metastases from breast cancer . Key word:Breast cancer ,Bone metastases, skeletal, osteolytic, Introduction Primary bone cancer is rare and occurs predominantly among children and adolescents. By contrast, secondary bone cancer is common and may arise from carcinomas of the breast, lung, prostate, kidney, and thyroid. The most frequently encountered metastases during evolution of cancer are bone metastases, which involve painful syndromes and affects the patients quality of life greatly.1 Bone metastases is commonly painful and in two thirds of patients it is agonising. The skeleton is the most commonly affected bony site by metastasis from breast cancer and the site of first distant relapse in almost one half of the patients with breast cancer. Metastasis to bone is a significant cause of morbidity and reason for referrals from both specialist physicians and Surgeons.2, 3 Management is multifaceted involving radiation therapy, and graduated use of opiate analgesics, hormone therapy and chemotherapy. Bone-seeking radio pharmaceuticals have provided a new option to these management strategies more popularly in advanced countries.4 Methods A total of 30 patients fulfilling the study criteria were included for the study. Patients with histologically proven carcinoma of the breast either attending the follow-up clinic or at the time of first presentation, having painful bone metastases were included in the study, irrespective of age, sex and performance status. Questionnaires were used to collect the patients’ personal data and all ongoing treatments received. Evidence of pathology like local recurrence and visceral metastases were documented. Informed consent was obtained from all patients included in the study. Evidence of bone metastases was obtained from plain x-rays and bone scan of the affected area. MRI and /or CT scan were done to rule out degenerative bone diseases in a few patients where bone scan was positive and plain radiographs were negative,for example in osteoporosis, and Paget’s disease. The choice of chemotherapy was anthracyclines based FAC regime and tamoxifen as the first line on hormonal therapy. For patients with bone metastases, radiotherapy was given to sites of skeletal metastases in addition to controlling local disease. All patients received analgesics, chemotherapy and tamoxifen usually before irradiation to the bone with local field irradiation( LFI). In this study, no patients presented or developed pathologic fracture. Results Of the 30 patients recruited into the study, those patients without evidence of distant metastases initially at the time of surgery for breast cancer accounts for 66.7% (stages IIA, IIB, IIIA & IIIB), and this group of patients developed metastases first in the skeletal system (figure 1), and 33.3% were stage IV at presentation. 51.4% of skeletal metastases involved the lumbar spine and 21.6% affects thoracic spine, i.e. 73% of cases were having involvement of the thoraco-lumbar region (table i). The predominant radiological finding in bone metastases from breast cancer was osteolytic bone lesions accounting for 93.3% of the x-rays findings. Mixed pattern, which is features of osteolytic and osteoblastic lesions were seen in only 6.7% (table ii). In 76.7% (23) only one bone was involved in the patients and in 23.3% (7), multiple, noncontiguous bones were involved (table iii). Majority of patients developed painful bone metastases after at least 12 months (63.3%) of diagnosing breast cancer (table iv) and 20% of thepatients had painful bone metastases at presentation. 20.0% of patients had painful bone metastases for < 3 months prior to LFI; 46.7% had pain for 4 – 6 months; 6.7% had pain for 7 – 9 months; 10.0% had pain for 10 – 12 months; and 16.7% had pain for more 12 months prior to treatment with LFI (table iv). Discussion The incidence of bone metastases from breast cancer in Pakistan is not known. In Nigeria, 1 in every 14 women is expected to develop breast cancer in their life time2 but the incidence and prevalence of bone metastases is not known . More than 100,000 new patients develop bone metastases each year in the United States and the , the prevalence of patients with bone metastases is estimated to be twice the number of new cases, owing to the prolonged survival of many patients with bone metastases.10 Approximately 20% of breast cancer patients have either predominantly bone or bone-only metastases.2, 10 Metastases to bone are in many ways similar to metastases to other organs and tissues in that tumour cells are deposited and grow to form a tumour that can progress to cause symptoms. However, metastases to bone are unique because of the special characteristics of bone anatomy and physiology. Batson’s plexus of veins serves as a unique pathway for tumour to colonize bone because it is a wide collection of thin – walled, valveless veins with low intraluminal pressure that lies outside the thoraco-abdominal cavity and therefore is not subjected to the changes in pressure in the thoraco-abdominal cavity. It connects with veins inside the spinal canal and with those around the vertebral column. The presence of tumour cells in bone causes reactions of both bone destruction and new bone formation.11 There is no good explanation for the variation in the magnitude of increased bone resorption or deposition in various malignancies. It is widely accepted that osteoclasts are responsible for the majority of bone destruction and complications seen in bone metastases. Bone destruction is by an osteoclasts-mediated osteolysis in response to humoral factors in the presence of tumour cells or tumour mediated osteolysis. Osteoclasts always precede tumour cells in resorption. The Osteoclasts-mediated phase is quantitatively the more important of the two. Bone destruction can also occur from bone necrosis caused by vascular compromise from tumour involvement.9 Bone formation may result from more than one mechanism. The tumour cells can induce ossification of the fibrous stroma.Tumours with abundant stroma, cause osteoblastic metastases, and bring about the formation of abundant new woven bone, whereas highly cellular tumours such as myeloma are not associated with new bone formation. Reactive bone formation, which is also the response of the bone to injury (fracture) (micro fracture or macro fracture), is the more frequent phenomenon of healing in the presence of metastases.14 The new bone, irrespective of the mechanism of formation, lacks the strength of normal lamellar bone. 14The radiographic appearance of bone metastases depends on which process (bone destruction or bone formation) predominates, although usually both are present. In breast cancer, the predominant feature often is osteolytic bone lesion (bone destruction)15,. Other antecedent or coexisting conditions may also have adverse effects on the bone integrity; these include bone loss secondary to menopause, therapeutic castration, senility, prolonged immobilization, and medications (e.g. Corticosteroids).9Plain X-rays of bone(s) is the fastest, least expensive, and the most readily available technique to diagnose bone metastases. It gives the best integration of overall bone structure and alignment. The destruction of bone presents has several patterns on radiographs, which appear to be related to variations in the growth rate of the tumour.There are 3 typical radiographic patterns of Metastatic disease: Osteolytic, Osteoblastic and Mixed. Because of variation in the bone microenvironment and clonal differentiation of tumours, different patterns may exist throughout the skeleton or within one bone.. 16Technetium diphosphonate bone scans are extremely valuable in identifying occult lesion and in diagnosing metastatic disease. Where as nearly 30%-50% of bone mineral must be lost for a lesion to appear on plain radiograph, bone scans show disease much earlier.17 i,
It is an essential part of cancer staging for skeletal metastases.
The bone scan has the ability to measure metabolic activity though it does not evaluate the structural integrity of the skeleton.17 All bone scan findings must be evaluated in parallel with plain radiograph, CT scan or both. Computed tomography Scans have been used in the evaluation of bone metastases for the diagnosis of equivocal lesions in patients with abnormal bone scan and normal bone X-rays findings, particularly if the areas of abnormalities are in the spine or other region that are difficult to evaluate by conventional radiographs (e.g. craniovertebral junction, sacrum, sternum).16, 18Magnetic resonance imaging is more sensitive than CT for detecting bone marrow involvement and can be used in early detection of cancellous bone involvement by tumour. MRI in the sagittal plane also allows visualization of the entire spine and can be used as the primary investigation of non-contiguous bone metastases, epidural cord or nerve root compression and gives information about tumour encroachment causing partial cord or root compression at levels between the areas of complete block.16, 17Plain radiography remains the most specific test to diagnose bone metastases. Bone scan is extremely sensitive and practical because it can screen the entire body at one time. Certainly, any abnormality found on bone scan should be assessed with plain radiographs. Only when the diagnosis cannot be discovered from clinical information and these baseline tests should CT scan or / and MRI be obtained. Radiological Findings 15 - 19 1. Vertebrae The pattern of presentation of bone metastases to the vertebrae is variable and diverse. It could be as a collapsed vertebra, solitary or multiple; erosion, destruction or absence of a pedicle; sclerotic lesions either solitary or multiple; generalized increased bone density e.t.c.15, 16 Bone metastases to long bones could present as a lucent bone lesion in the medulla which is well defined, 2. Long bones No marginal sclerosis, and no expansion. The absence of reactive bone formation implies a fast growth rate especially in breast cancer. An aggressive pattern of destruction could present as an ill-defined lucent bone lesion in the medulla. Moth-eaten bone appearance presents with multiple scattered lucencies of variable size with no major central lesion in which coalescence may occur later. This may be a feature of an indolent disease. In long bones, pathologic fracture is a common feature of bone metastases.16, 18 3. Skull In metastases to the skull, there is lucency in the skull vault, with no surrounding sclerosis in adults and it is usually irregular and ill-defined. There is destruction of petrous bone/apex with irregular lytic defect. There may be hair on end skull vault. There may be erosion and osteoporosis of the sella without expansion.16 4. Ribs & Clavicle Lesions may be solitary or multiple. Metastatic lesions are commoner than primary lesions and primary malignant conditions more than benign conditions. The pattern is that of a poorly defined lytic lesions and the sub-articular cortex is usually the last to be destroyed.16 The radiological appearances described above are not pathognomonic of bone metastases alone as similar features may be seen in other primary bone malignancies, degenerative diseases, infections, e.t.c. Conclusion Osteolytic features are the commonest radiological findings, and lumbar region is the commonest site of bone metastases;the reason for this is not well documented. However, any site within the spine is prone to develop symptomatic metastases. In metastatic survey for asymptomatic patients, x-rays of the thoraco-lumbo-sacral region is advised as baseline. In the evaluation of locally advanced and metastatic breast cancer, any bone pain should be considered bone metastases until proven otherwise. This will lead to prompt treatment and eventually improve the quality of life of the patients References
Copyright 2006 - Nigerian Journal of Surgical Research The following images related to this document are available:Photo images[sr06030t4.jpg] [sr06030t3.jpg] [sr06030f4.jpg] [sr06030f1.jpg] [sr06030t3b.jpg] [sr06030t5.jpg] [sr06030t1.jpg] [sr06030t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}