 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Nigerian Journal of Surgical Research, Vol. 8, No. 3-4, Jul-Dec, 2006, pp. 151-154 Wound dressing where there is limitation of choice 1G. A. Rahman, 2I. A. Adigun, 1I. F. Yusuf, and1 C. K. P. Ofoegbu 1Division Of General Surgery Division Of 2Plastic
And Reconstructive Surgery, Department Of Surgery, University Of Ilorin Teaching Hospital, Ilorin Code Number: sr06036 Abstract Background
Many sophisticated dressings are available to the wound care practitioner in
the developed countries. These materials are made from a wide range of products
like polyurethane, salts of alginic acid and other gelable polysaccharides. The
situation is different in the developing countries where what is commonly available
to wound care provider are traditional agents such as sodium hypochlorite,
hydrogen-peroxide, cetrimide solution, chlorhexidine and others. The aim of
this study is to reappraise the problem of limitation of wound dressing
selection in the developing countries and to sensitize the wound care
practitioner on the use of the commonly available products based on the needs
of a different wound or even the same wound throughout its healing course.
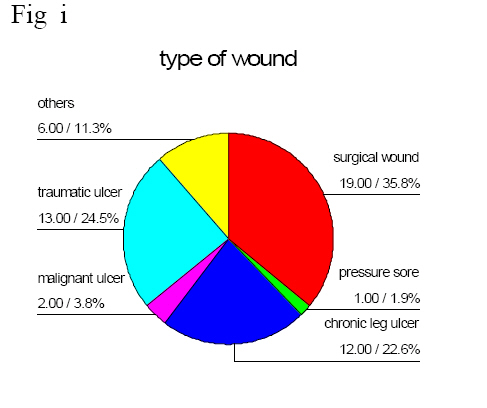
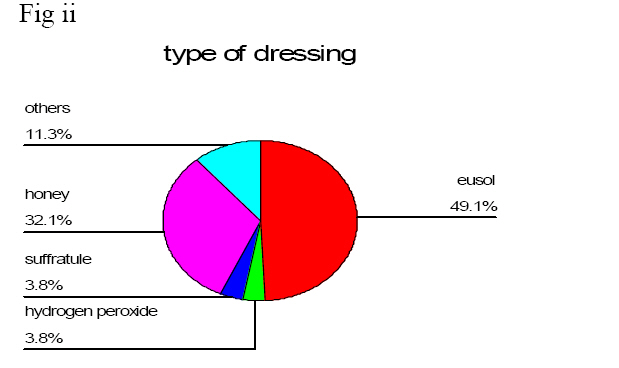
Key words: wound, dressing, types, developing countries. Introduction No one dressing agent is suitable for the management of all types of wounds, and few are ideally suited for the treatment of a single wound during all stages of the healing cycle. Successful wound management therefore depends upon a flexible approach to the selection and use of products based upon an understanding of the healing process combined with knowledge of the properties of the various dressings available. The process of dressing selection is determined by a number of factors which includes the nature and location of the wound, and the range of materials available. In most situations the cost of treatment is also a major factor1. In the developed countries, many sophisticated dressings are available to the wound care practitioner which are made from a wide range of materials including polyurethane, salts of alginic acid and other gelable polysaccharides such as starch and carboxymethylcellulose. These materials are combined to form products as diverse as films, foams, fibrous products, beads, hydro gels and hydrocolloid dressings2. The situation is totally different in the developing countries like ours where what is still commonly available to wound care provider are traditional agents such as sodium hypochlorite, hydrogen peroxide, cetrimide solution, chlorhexidine and others. These agents have been proven to be of limited efficacy and may also have an adverse effect upon the healing process3and therefore get out of favour4. Wound healing is a dynamic process and the performance requirement of a dressing can change as the wound progresses towards healing. The aim of this study is to re-appraise the problem of limitation of wound dressing selection in the developing countries. This is with the aim of sensitizing the wound care practitioner on the use of the commonly little available products based on the needs of a different wound or even the same wound throughout its healing course. Methods: This study took place in a tertiary health institution located in the North Central Zone of Nigeria. Patients attending the General Outpatient Department (GOPD) of the hospital for wound dressing of different aetiologies were used for the study. The authors who are surgeons familiar with wound care management visited the dressing unit of the GOPD daily for a whole week in October 2005. A proforma was designed where information on each of the patient was recorded. Information collected included: the age, sex, occupation, type of wounds, frequency of dressing, type of dressing, cost of care, and the cost bearer among others. The data were entered into the SPSS 11.0 software for analysis. Results: Fifty-three patients attended the dressing unit of our GOPD during the six days of study. The age range was between 1 year and 84 years The mean age was 38.7 years (SD-23.0). There were thirty-four males and nineteen females with a male to female ratio of 1.8:1. Sixteen patients (30.2%) were traders, twelve patients (22.6%) were students, eleven patients (20.8%) were farmers and nine patients (17.0%) were civil servants. For the purpose of this study, wound managed were classified into six types as shown in Fig. 1. Nineteen patients (35.8%) had surgical wounds (from surgical operations) of different etiology while thirteen patients (24.5%) were being managed for traumatic wounds resulting from poorly managed traumatic injuries. There were twelve patients (22.6%) with chronic leg ulcer while only one patient (1.9%) was being dressed for pressure sore. Fig. 2 shows various dressing agents available for use in our centre. The result showed that twenty-six patients (49.1%) had their wounds dressed with hypochlorite solution (Eusol), seventeen patients (32.1%) had their wounds dressed with honey, two patients’ wound were being dressed with hydrogen peroxide, two patients also had sufratulle gauze dressing. The remaining six patients (11.3%) had other agents such as cetrimide and chorhexidine solution used for their dressing. The frequency of wound dressing shows that of these fifty-three patients; Twenty-three patients (43.4%) had a daily wound dressing while twenty-eight patients (52.8%) had an alternate day dressing of their wounds. The cost of care of these patients’ wound dressing per week excluding transportation to hospital, showed that twenty patients (37.7%) spent an average of five-hundred Naira (N500.00) per week while thirty-one patients (58.5%) spent an average of six hundred Naira (N600.00) per week. The remaining two patients were being exempted from payment Discussion Effective wound management requires an understanding of the process of tissue repair and a knowledge of the properties of the dressing materials available. It is when these factors are considered that the process of choice of wound dressing can be undertaken in a logical and informed fashion. A single dressing cannot address or correct the underlying pathology of a wound, rather, it should be selected based on the needs of the wound. This can be achieved by thorough assessment of the wound in terms of its dimension, the type of tissue present in the wound bed, the quality and quantity of exudates, condition of the surrounding skin and the microbial status. This assessment should be performed on all wounds before they are dressed. This study shows that we are still using the traditional wound dressing agents for dressing. Twenty-six patients (49.1%) had their wounds dressed with Eusol, while 3.8% were dressed with hydrogen peroxide. Seventeen patients (32.1%) were dressed with honey .In 23 (43.4%) patients wounds were dressed daily which can be regarded as high frequency dressing. High frequency dressing is expensive, uncomfortable to the patients and stressful to manpower. It is safer to choose dressings that require changing less frequently, thereby reducing risk of nosocomial infection, cost of care, further tissue damage and patient discomfort 5 . Majority of our patients spent between five-hundred Naira (N500.00)($4 USD) and six-hundred Naira (N600.00)($5 USD) per week on wound dressing. The unavailability of varieties of wound dressing in our environment has led those who must care for wounds to resort to the use of traditional agents such as sodium hypochlorite, hydrogen peroxide, cetrimide ,chlorhexidine and honey. Usually there may be no room for choice of agent depends and the most readily available agent is used . In the developed countries, several modern wound dressing materials are available to the practitioners and the choice of dressing materials take into consideration the needs of the wound at a particular stage in the healing process1. These dressing materials are grouped according to their performance. Some of these agents include hydrocolloid, hydrogel, alginate, and polyurethane foam. They are indicated for selected wounds or the same wound for different roles at different phases of wound healing. Some characteristics that distinguish these recent products are fluid status, conformability, nice scent, absorbing characteristics, handling and adhesive properties, and the presence of antibacterial and haemostatic activity . Others include the ease of application and removal and the interval between dress changes6. Before a clinician chooses a wound dressing agent it is necessary to identify the purpose or principal aim of that particular treatment. In most cases, it will be to facilitate cosmetically acceptable healing in the shortest possible time. Occasionally, however, priorities can change and the speed and quality of healing may not be of primary importance. For example, a patient with a large malignant wound, it may be more important to concentrate on removal or containment of both the odor and the copious exudates produced by the discharging lesion. This will improve the patient’s quality of life remakably7, 8. Dressing agents may be chosen for 4 purposes. Remove sloughy necrotic tissue, promote granulation and epitheliasition of the wound, Bring about autolytic debridement of dead skin over some wounds. In our environment, we commonly use gauze pads soaked in saline or other solutions such as sodium hypochlorite (Eusol) or hydrogen peroxide which may be time consuming. Honey is another agent that is readily available to us in the developing countries. It is a good debriding agent and it is commonly used by clinicians in necrotic wounds9, but the problem of frequent dressing and pain associated with its use is a major disadvantage. The use of hydrogel and hydrocolloid are advances in developed would. A dressing such as Intrasite Gel, Granugel and Sterigel where available is more attractive and very convenient. The gel is simply placed on the wound and covered with gauze till the next dressing. Hydrocolloids high absorptive capacity that greatly limits the rate of frequency of change of dressing. When the necrotic covering eventually separates, it frequently leaves behind a wound containing yellow, partially liquefied material called slough such as in ,pressure sores , diabetic foot ulcers burns and chronic leg ulcers . It has been shown experimentally that slough and devitalized tissue will predispose a wound to infection by acting as a bacteriological culture medium and inhibiting the action of leucocytes in the wound10, 11. For good healing rate, such wounds should be properly cleansed or debrided. This can be done with some of the recent agents such as Debrisan. Debrisan are polysaccharide beads for dressing was one of the first modern dressings used for wound cleansing. When used on sloughy wounds, the beads absorb fluid and progressively remove bacterial and cellular debris away from the surface of the wound12. Sloughy wounds which also produce a degree of exudates may be dressed with alginate dressings. Other materials which are sometimes used to debride sloughy wounds include enzymatic agents such as Varidase, crab collagenese and krill13. Polysaccharides such as honey and sucrose have also been used to facilitate wound cleansing. Granulated or icing sugar has been used successfully14, 15 interest has just been focused on the use of a sugar paste containing polyethylene glycol 400 and hydrogen peroxide16, 17, 18. A significant development of dressing sloughy wounds is the use of larva therapy (maggots) for the rapid removal of slough and necrotic tissue from wounds such as leg ulcers, pressure sores, and diabetic foot ulcer19. It has been reported that larvae are of value in burns20 and plastic surgery for cleansing wounds prior to grafting21. In a granulating wound there is no single dressing that is suitable for use in all situations. In the developing countries, where there is limitation of materials for wound dressing, these wounds are usually packed with gauze soaked in saline, hypochlorite or proflavine. In some studies, honey is used continuously for dressing in this phase of wound healing thus causing hyper granulation, This may usually slows down the process of epithelisation. In the developed countries such wounds will be dressed with alginate fibre or hydrocolloid dressing if exudate production is not a problem. The production of granulation tissue continues until the base of the original cavity is level with the surrounding skin. At this stage, the process of epithelisation begins around the wound margin. Except on few occasions, superficial or epithelising wounds tend not to produce large quantities of exudates. Traditionally, these wounds have been dressed with paraffin gauze covered with a layer of Gauze and Cotton tissue (“Gamgee”) which is readily available in most centers in developing countries but some centers have reported that the use of both alginates22,23 and hydrocolloids dressings24 offer significant advantages in these situations. The later reducing the time to healing of donor site to about 7 days compared to 10-14 days for comparable wounds dressed with conventional fabric dressings. Wound related factors takes priority when considering choice of dressing for a particular wound. Therefore, we should always ask ourself, what type of wound are we dealing with? Is it a superficial, full thickness or cavity wound? Is the wound necrotic, sloughy, and granulating or epithelising? What about its characteristics, is it dry, moist, heavily exuding, malodorous, excessively painful or liable to bleed? What about the bacterial profile, is it sterile, colonized or infected? For example, a superficial, granulating or epithelising wound with minimal exudate should not be dressed with agents like hypochlorite solution or hydrogen peroxide. Rather, such wound may be dressed with sofra-tulle covered with saline soaked gauze or even dry gauze. In clinical practice, when considering dressings for an acute wound, the emphasis should be on prevention of infection and promotion of healing5 whereas in chronic wound-healing, the control of wound infection is more important25 Conclusion While we are still hoping to acquire newer agents for wound dressing, in the developing countries, we have made an effort to discuss some characteristics needed to make us choose wisely from the limited variety of dressing materials to meet the needs of our wounds for efficient wound care. References
Copyright 2006 - Nigerian Journal of Surgical Research The following images related to this document are available:Photo images[sr06036f1.jpg] [sr06036f2.jpg] |
| |||||||||

{kind=link}
{kind=link}