 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Nigerian Journal of Surgical Research, Vol. 8, No. 3-4, Jul-Dec, 2006, pp. 171-173 Malignant haemangiopericytoma of the left thigh with metastases to the bones and lungs: A case report 1 O.M Atalabi 1 O.P Ibinaiye 1 M.O Obajimi 1 O.Ogunseyinde and 2Akang E.E.U 1Departments of Radiology and 2Pathology, College of Medicine, University College Hospital, PMB 5116, Ibadan, Nigeria.
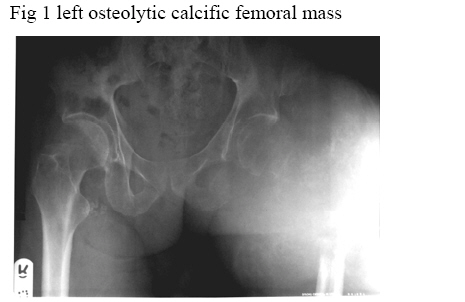
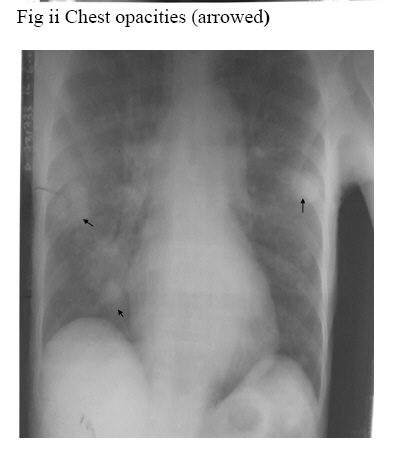
Code Number: sr06042 Abstract Haemangiopericytoma is an uncommon mesenchymal neoplasm. Haemangiopericytoma is believed to arise from the pericytes, contractile spindle cells that surround the capillaries and post-capillary venules. We present an unusual case of histologically confirmed malignant haemangiopericytoma of the left thigh in a 70 year old male with metastasis to the lungs and left femoral bone. Introduction Haemangiopericytoma is an uncommon mesenchymal neoplasm that was first described and named by Stout and Murray in 1942 1, however it was not until 1949, when Stout 2 reported 25 additional cases, that the tumour received widespread recognition. It may occur at any anatomical site. Haemangiopericytoma is believed to arise from the pericytes, contractile spindle cells that surround the capillaries and post-capillary venules 1-4. The tumour typically comprises uniform elongated cells surrounding a rich, branching network of thin-walled vessels of various sizes and shapes 5. However, there are difficulties in the histological diagnosis of haemangiopericytoma because other soft tissue neoplasms may have areas of rich “haemangiopericytoma-like” vascularity 6, 7. It occurs commonly in fourth to fifth decade of life and shows no sex predilection8. Spread is not a common feature of the tumour and reports of spread occur frequently after incomplete surgical resection4. We report our experience in the management of an hemangiopericytoma presenting rarely for the first time with metastasis. Case Report A.H was a 70 year old male patient. He first presented at the surgical out-patient clinic of the University College Hospital, Ibadan in July, 2000 with a large soft tissue swelling on the left thigh which was painless but had been progressively increasing in size. The initial clinical diagnosis was osteogenic sarcoma. An incisional biopsy for histology was done. The histology report revealed a malignant haemangiopericytoma of the left thigh. The patient was getting ready for radiotherapy and surgical excision of the mass but he absconded. He came back two years later in June 2002 with inability to walk and complete loss of mobility of the left lower limb and very limited mobility of the right leg. There was severe pain in both legs, weight loss and persistent cough for six months The mass in the left thigh had increased tremendously in size. On clinical examination, the mass was firm and tender, not attached to the overlying skin and was not mobile. It was neither pulsatile nor warm to touch. The chest was clinically clear and the review of other systems was essentially normal. The plain radiographs of the pelvis and both femoral bones showed a huge soft tissue mass on the upper third of the left thigh with osteolytic destruction of the proximal third of the left femur and the femoral head . Amorphous calcification was also seen within the mass lesion fig. i. There was an associated fracture of the mid shaft of the right femur (fig. iii). The chest X-ray showed multiple cannon ball metastases to both lung fields(fig. ii). The heart and bony thorax were within normal limits. . Abdominal ultrasound done was normal. Doppler ultrasound, Computerised Tomography (CT) and angiography were contemplated to further assess the mass but the patient defaulted the second time . We have not seen him since them. Discussion Haemangiopericytoma accounts for less than 2% of soft tissue sarcomas 9, 10. It may occur at any age but is most common in the fifth and sixth decades 3, 4, 8. In the series of 106 patients reported by Enzinger and Smith 4, 37(35%) cases affected the lower extremity and 26 (25%) were in the pelvis or retroperitoneum, of the other 43 cases in that series, 17 involved the head and neck region, 15 were located in the trunk and 11 were in the upper extremity. Orbital haemangiopericytoma has also been Documented14.Haemangiopericytoma generally presents as a painless mass, but pressure on adjacent viscera may cause symptoms 3,4, and local recurrence implies a poor prognosis 4. In the series of Enzinger and Smith 4, local recurrence preceded metastasis in 11 of 17 patients who developed metastases. The lungs and bone are the most common sites for metastases, as occurred in this patient 4, 10. Various paraneoplastic syndromes have been described in association with haemangiopericytoma, including hypoglycaemia 11, 12, hypophosphataemic osteomalacia 13, 14, which might have accounted for the pathological fracture of the mid shaft of the right femur in this patient, and hypertrophic pulmonary osteoarthropathy 14. The reported frequency of calcification on CT in haemangiopericytoma varies from 0.94%-71.4% 4, 9. Amorphous calcification was seen in this patient. Bone erosion, which was also seen in this patient, has been reported before in one of the 106 cases of Enzinger and Smith 4; seven of the 60 cases described by McMaster et al 3 had similar bone erosion. Haemangiopericytoma is a highly vascular tumour and occasionally may cause clinically significant arteriovenous shunting 17. With Doppler sonography, from the experience of others13, it is likely that arteriovenous shunting would be shown in a hypervascular neoplasm such as haemangiopericytoma. Haemangiopericytoma must be distinguished from the more common sarcomas such as malignant fibrous histiocytoma and liposarcoma, especially when occurring in the thigh. As already mentioned, these commoner tumours and others may be confusing as they contain areas of rich haemangiopericytoma-like vascularity. As with other soft tissue sarcomas, modern imaging techniques allow pre-operative assessment of the size and location of the haemangiopericytoma, the degree of involvement of surrounding structures, and the vascularity of the tumour 5. Haemangiopericytoma should be considered in the differential diagnosis of hypervascular soft tissue masses arising in the retroperitoneum, pelvis or lower extremity 5. References
Copyright 2006 - Nigerian Journal of Surgical Research The following images related to this document are available:Photo images[sr06042f3.jpg] [sr06042f2.jpg] [sr06042f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}