 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Nigerian Journal of Surgical Research, Vol. 8, No. 3-4, Jul-Dec, 2006, pp. 179-181 Malignant transformation in Pre-existing Naevi. A review of two cases M.O.A Samaila and 1A.G Adesiyun Departments of Pathology
and Obstetrics &Gynaecology# Ahmadu Bello University Teaching
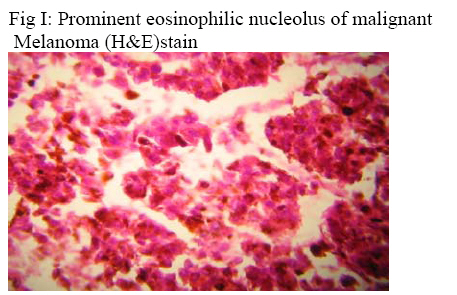
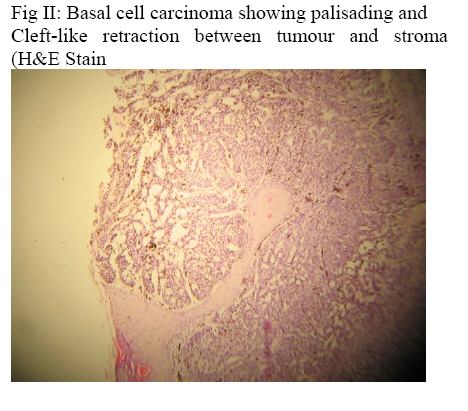
Hospital, Zaria Code Number: sr06045 Abstract Pigmented naevi (melanocytic naevi) are common and are widely distributed all over the body.The average number of naevi seen in a Caucasian is between twenty and thirty. They are either congenital or acquired benign neoplasm of melanocytes. They may occur as giant lesions at birth, and are more prone to malignant transformation. However, the risk of malignant transformation associated with naevi irrespective of size is well established and a variety of malignancies have been reported to arise from a naevus. The incidence of malignant transformation in naevi is 4% to 9%. We present two cases of malignant tumours arising from pre-existing naevus. The first was a 60-year old woman with a malignant melanoma arising in a vulva intradermal naevus. The second was a 51-year old woman with a basal cell carcinoma arising in a facial naevus. Introduction Pigmented naevus (melanocytic naevi) is the commonest tumour in the entire category of neoplastic diseases.1-4 The frequency of its occurrence lulls suspicion and hence favours tolerance by patients and physicians alike.3 The time of appearance of naevi is variable and seems related to exposure to melanin provoking influence.2-4 It has a recognizable and important role in tumour progression as seen in dysplastic naevus and heritable malignant melanoma.2 The risk of malignant degeneration associated with naevus is significant, while the incidence rate of malignant transformation is 4% to 9% .5-7 We present 2 cases of malignant tumours arising in pre-existing naevi. Case Report Case 1 A 60-year old woman presented with a 2-year history of recurrent right vulva swelling which was mobile and non tender. She had a previous biopsy of the same lesion 2years earlier with a histological diagnosis of intradermal naevus. She was examined and the only abnormal finding was a right firm nodular vulva mass measuring 5x4cm. She had an excisional biopsy of the mass, which was sent to the histopathology department for histological assessment. We received the tissue specimen, a nodular mass weighing 15g in 10% formalin. Cut sections of the mass showed solid dark and cream areas. Histologic sections were processed in paraffin wax and stained with Haematoxylin and Eosin (H&E). Histology showed a fairly demarcated tumour with a lobular pattern, composed of oval cells having vesicular nuclei and prominent eosinophilic nucleolus and scanty cytoplasm. It was diagnosed malignant melanoma. Patient 2 A 51-year old woman presented to the surgical outpatient clinic of our hospital with a bleeding facial nodule located on the right temporal region. The pigmented lesion was present from birth and the bleeding was spontaneous. There was associated itching and increase in size of the lesion recently. She was examined and had an excisional biopsy of the lesion, which was sent for histological assessment. We received the tissue in our department in 10% formalin. Macroscopically, a wedge shaped skin biopsy with a central ulcer measuring 2x2cm and weighing 1g was seen. Cut sections showed a central ulcer with gray areas. Histologic sections were processed in paraffin wax and stained with H&E. Histology revealed an ulcerated epidermis overlying an infiltrative tumour growing in nests and cords. This was composed of moderately pleomorphic spindle cells exhibiting peripheral palisading. 3-4 mitotic figures per high power field (PHF) were seen. It was diagnosed basal cell carcinoma. Discussion Pigmented naevi (melanocytic naevi) are common and are widely distributed all over the body.8,9 They are either congenital or acquired benign neoplasm of melanocytes. 10 The incidence of malignant transformation in naevi is 4% to 9%. 5-7, 11, 12 Symptoms such as changes in pigmentation, increasing size, itching and unprovoked bleeding from a preexisting naevus may increase the risk of malignant transformation.Many malignancies have been associated with congenital neavi.5,7,10 The commonest is malignant melanoma.6 The 5-year cumulative table risk for developing malignant melanoma is 2.3% to 5.7%.11, 13, 14 Other reported malignancies include liposarcoma, rhabdomyosarcoma, malignant peripheral nerve sheath tumour and neurocutaneous melanosis.7, 11, 12, 15 Malignant melanoma (MM) is a relatively common neoplasm arising from melanocytes. Its incidence rates show substantial worldwide variations.16 The reasons for this variations are thought to be the degree of exposure to sunlight and the amount of skin pigmentation present. Twenty percent of the world’s melanoma are seen in Black Africans and Asians and may not be clearly associated with sunlight exposure.17 Other predisposing factors include pre-existing naevus, some genetically determined diseases such as xeroderma pigmentosa and Von Recklinghausen’s disease.18 Melanoma in Nigerians appeared to arise from existing epidermal melanocytes and not from preexisting naevus cells.19,20 It was difficult to establish whether the initial naevus was congenital in our patient as she only noticed swelling few months to first presentation in the hospital. Basal cell carcinoma (BCC) is a locally invasive tumour which rarely metastasizes.21 It is not common in our African environment, due to the protective skin pigmentation from ultra violet (UV) radiation. The actual incidence of BCC world wide is not accurate because patients are often treated in Physicians’ consulting rooms.22 However, its incidence depends on phenotype and higher UV levels and increases with immunosuppression and in patients with defective DNA repair genes.21 The sites of predilection are the head and neck which are maximally exposed to sunlight.23 The presence of MM and BCC in preexisting naevus lends credence to their derivation from common histiogenetic origin. Pigmented naevus is a common lesion which has a significant risk of malignant t transformation. Any change in size, pigmentation, itching and unprovoked bleeding should arouse suspicion and be treated promptly. References
Copyright 2006 - Nigerian Journal of Surgical Research The following images related to this document are available:Photo images[sr06045f2.jpg] [sr06045f1.jpg] |
| |||||||||

{kind=link}
{kind=link}