 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
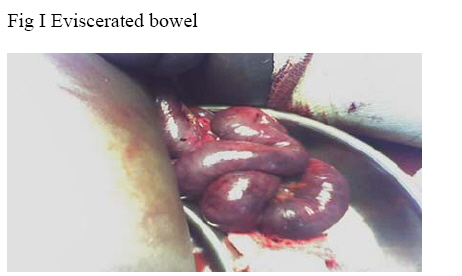
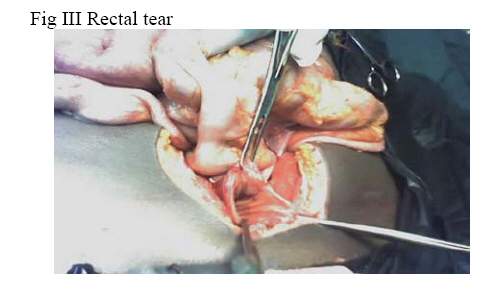
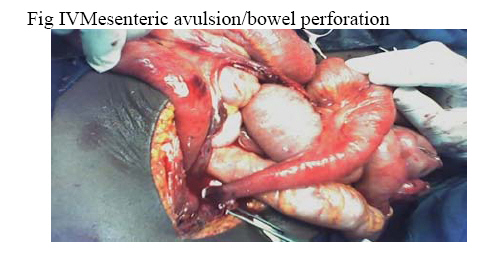
Nigerian Journal of Surgical Research, Vol. 8, No. 3-4, Jul-Dec, 2006, pp. 182-184 Transanal evisceration of the small bowel from blunt abdominal trauma A.C Adisa , C Onyegbule and A.U Mbanaso Department of Surgery Abia State University Teaching Hospital, Aba E mail : adisayinka@yahoo.com. Code Number: sr06046 Abstract Evisceration of the small intestine through the anus has been reported to occur spontaneously and in association with trauma. Small bowel evisceration through a rectal injury caused by blunt abdominal trauma has been documented in association with a variety of injury mechanisms. We report a case of a 19 year old boy who sustained blunt injury to the thigh and pelvic region with a traumatic evisceration of the small bowel through the anus. There were no apparent abdominal injuries on examination. Unlike most cases reported in the medical literature, there was extensive peritoneal soiling with fecal matter as a result of multiple perforations of the small bowel. The disparity between the physical findings at initial examination and the extensive intra-peritoneal injuries seen at laparatomy calls for a high index of suspicion in such cases. Introduction Rectal or Rectosigmoid perforation with transanal small bowel evisceration is a remarkable occurrence because of its rarity and extraordinary presentation. Less than 70 of such cases have been reported in the English literature since the first recorded case in 1827 by Brodie. Majority of the reported cases occur as a spontaneous event in elderly patients. Less than 20 cases have been documented to occur as a result of trauma. The etiology of trauma induced evisceration of the small bowel could be divided into barotraumas from suction injuries and blunt trauma. For this to occur, the degree of blunt trauma is usually very severe with associated injuries to other parts of the body. Case Report A 19 year old boy presented to the accident and emergency department within an hour after he was hit by a vehicle while attempting to cross the road. He sustained a severe crush injury of the left thigh with fracture of the left tibia and fibula. There was no obvious injury to the abdomen. The abdomen was full with no bruising of the skin. It was soft, with no tenderness and guarding. Rectal examination revealed a long loop of non viable small bowel protruding from the anus (fig 1 and 2).There were no injuries to the anus or the perineum. He was in shock with a Glasgow coma scale score was 12.His blood pressure was 90/60mm of mercury, pulse rate was 120beats/minute and respiratory rate was 30/minute.A urethral catheter was passed which drained clear urine. On investigation, his haemogram was 7gm/dl and plain X-rays of the pelvis and the left lower limb showed comminuted fractures of the tibia and fibula and fracture of the pelvic bone. He was resuscitated with intravenous fluids and anemia corrected with four units of packed cells. He was the n deemed fit for exploratory laparatomy. Findings at operation included massive hemoperitoneum, gross fecal contamination, multiple perforations of the small bowel with extensive mesenteric tears, contusion of the anterior urinary bladder wall, fracture of the pelvic bone along the symphysis pubis and a longitudinal tear on the anterior part of the first part of the rectum through which bowel loops had herniated through and were protruding through the anus (fig 3 and 4). The non viable eviscerated small bowel loops were resected and the perforations closed in 2 layers. The tear in the first part of the rectum was repaired in two layers and the repair protected by a proximal sigmoid loop colostomy. Peritoneal lavage was done with warm saline and the abdomen closed in layers. Patient was admitted into the ICU for intensive management. Patient however went into shock and died 6 hours after the surgery. Discussion Evisceration of small bowel loops from the anus was first described by Brodie in 1827(1). A review of the English literature since then showed that less than 70 cases have been reported since then. Of these, the majority are due to spontaneous rupture of the rectum. Spontaneous rupture of the rectum with small bowel evisceration occurred usually in elderly patients after straining with defecation or any Vasalva-type pressure that increase intra-abdominal pressure like vomiting or coughing. . Majority of these patients are women and associated rectal prolapse is a common finding. Other predisposing factors include chronic constipation, congenital malformation of the rectum, narrowing of the rectum, enteroptosis, microscopic diverticula, rectovaginal fistula, previous acute ulceration of the intestinal wall, and nonspecific acute rectal colitis(2;3) Etiology of traumatic transanal small bowel evisceration can be divided into three categories: suction injury, blunt abdominal trauma and iatrogenic injuries.4 Trans-anal small bowel evisceration has been described in children who have sat down on swimming pool drains, which can produce significant suction5. Small bowel evisceration through a rectal injury caused by blunt abdominal trauma has been documented in association with a variety of injury mechanisms6,7 Finally, iatrogenic injuries including reduction of prolapse and incision of ‘hemorrhoids’ have also been documented8,9 Surgical management is mandatory for all patients. The standard treatment reported for this condition to date has been exploratory laparatomy with reduction of small bowel in the abdominal cavity with or without small bowel resection and repair of the rectal/rectosigmoid tear. Only one case has been successfully managed laparoscopically10. Eviscerated bowel should be kept warm and moist by wrapping it in warm moist packs. The bowel should be carefully reduced from the anus and preserved if viable. Resection was necessary in our case as a result of extensive mesenteric stripping leading to bowel gangrene. The rent in the rectum which is usually longitudinal and in the anti mesenteric border should be repaired and other associated injuries repaired. 11 The use of a proximal diverting colostomy to protect the repaired rectum should be selectively performed on the basis of the patient condition, degree of fecal contamination and severity of the rectal injury. In most cases, there is little fecal contamination because the prolapsed loops of small bowel effectively plug the rent in the rectum, thus preventing fecal spillage. In this patient, a proximal sigmoid loop colostomy was necessary due to extensive fecal contamination from multiple small bowel perforations, shock and massive blood transfusions. The severity of the injury and the extensive intraperitoneal injuries with the associated sepsis and shock can explain the poor outcome in this patient. References
Copyright 2006 - Nigerian Journal of Surgical Research The following images related to this document are available:Photo images[sr06046f1.jpg] [sr06046f2.jpg] [sr06046f4.jpg] [sr06046f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}