 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
International Journal of Enviornmental Science and Technology, Vol. 5, No. 4, Autumn 2008, pp. 509-516 Effects of industrial air pollution on the respiratory health of children 1 *E. E. Nkwocha; 2 R. O. Egejuru 1 Department of Environmental Technology, Federal University of Technology Owerri and Research Fellow at the Imo
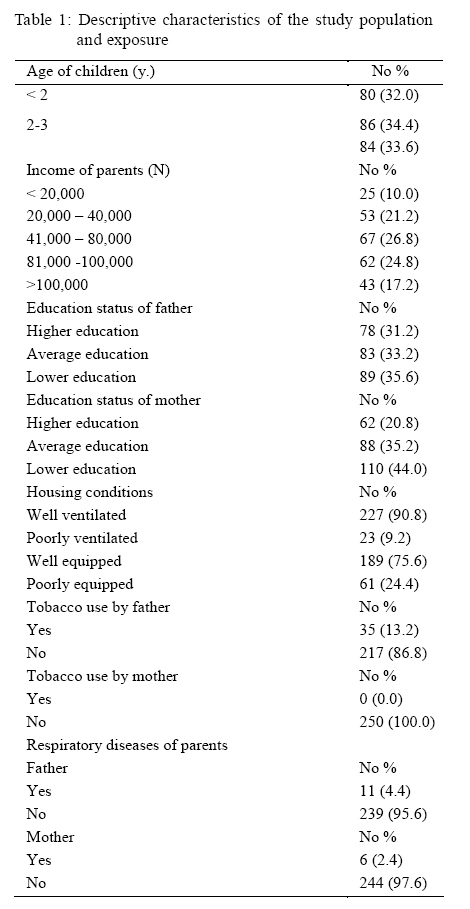
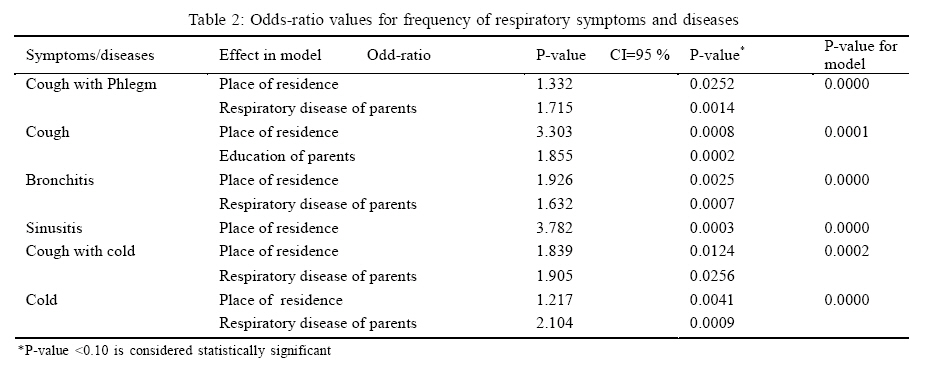
State University Owerri, Imo State, Nigeria Received 15 April 2008; revised 29 May 2008; accepted 17 June 2008 Code Number: st08057 ABSTRACT There is growing concern regarding to the possible effects of air pollution on respiratory health of children in Eleme industrial area of Port-Harcourt Nigeria. A total of 250 children were sampled from six primary schools with pre-nursery facilities for a period of 18 months. Subjects were divided into two zones (A and B), monitored and examined on weekly basis. The effects of four criteria pollutants (nitrogen dioxide, sulfur dioxide, particulate matter and carbon monoxide) on the respiratory health of the children were examined with reference to symptoms and diseases such as cough, cold, bronchitis, sinusitis and phlegm. Data were obtained from surveys of socioeconomic status of parents of subjects, three air monitoring stations and on-the-spot measurements of these pollutants and their association with symptoms and diseases analyzed. Results showed that there was a strong association between air pollution and symptoms and diseases among children. The effect was strongest among children below 2 years of age (adjusted OR = 3.5, 95%, CI 1.7-8.3) in the highly polluted zone than in the less polluted area. The higher the age of children, the lesser the susceptibility to these pollutants. These general results constitute a starting point for further research on long-term exposure to industrial air pollution and call for an urgent enforcement of regulatory standards to protect the most vulnerable groups in most of the growing metropolises of the country. Key words: Emissions, diseases, distance, pollution gradient, symptoms, vulnerability INTRODUCTION The problem of air pollution is a serious threat to environmental health in many cities of the world (Khitoliya, 2004; Schneider, 1998;WRI, 1996; North, 1994; Frior, 1990). High concentration levels of pollutants have been shown to have adverse impact on respiratory systems (Pope and Dockery, 2006; Ward and Ayres, 2004), cardiovascular and neurological systems in humans (Metzger et al., 2004; Cramer, 2002; Peters et al., 2000; Katsouyanni, 1996; Schwartz and Dockery, 1992). It has been associated with a wide range of symptoms (de Hartog et al., 2003; Janssen et al., 2003), low birth weight (Ashdown-Lambert, 2005; Mirshra et al., 2004; Chen et al., 2002; Bobak, 2000), increased hospitalization, sudden infant death and high mortality (Ostro et al., 2006; Dales et al., 2004; Liu et al., 2003; Wong et al., 2001; Schwartz, 1992). However, the exact mechanisms linking the inhalation of ambient air particles to an acute exacerbation of diseases are not completely understood (Brook et al., 2004). In Nigeria, increasing trends in population, urbanization and most especially industrialization have exacerbated the problem of air pollution and have diversified its sources. Although the concentration of major pollutants vary from city to city, the most important sources include fuel consumption for power generation, gas flaring (especially in the Niger-Delta region) motorized vehicles, incineration of solid waste and industrial processes (Monahan, 1997; Evoh, 2002; Obadina, 2002). Most researchers on the issue focused on the measurement of ambient concentration levels of criteria pollutants from vehicular emissions in major cities (Holland et al., 2003; Bernard and McGeehin, 2004; Hertz Picciitto et al., 2003) and impact of emissions on farmlands and agricultural production (Clarkson, 2007; Tenenbaum, 2008). A retinue of these studies were funded by oil-related companies which produced conflicting results to satisfy specific interests. Despite their spurious findings, the increased concentration levels of some criteria pollutants within the industrial zones of the fast growing metropolises has not been examined in the context of their association with the respiratory health of the local populations, especially among the most vulnerable groups such as children and the elderly. Most recent investigations have been focused on children, a population believed to have enhanced vulnerability with respect to air pollution (Hwang et al., 2005; Bateson and Schwartz, 2004; Fischer et al., 2002; Katsouyanni et al., 2001). This study examined an aspect of this problem: air pollution in Eleme Industrial Area of Port Harcourt. The working hypothesis therefore is that there is a strong association between air pollution and incidence of symptoms and diseases among children living in the area. MATERIALS AND METHODS Geographically, Port Harcourt is located in the South-Eastern coastline of Nigeria between latitude 400 5N and Longitude 700 5E. Eleme is the industrial area located at 30 km. from the main town. This area is highly industrialized, ecologically diversified, with rich farmlands. These have made her population to grow from 32731 in 1991 to 51228 in 2006. Much of the growth was due to migration from other neighbouring states (Imo, Abia, Cross-River), but natural increase has contributed significantly. Since the industrialization of the area, air quality standards have not been imposed by either the state or federal authorities to mitigate industrial emission levels. Major industries include the Port-Harcourt refinery established in 1965; National Fertilizer Company (NAFCON), operational since 1987 (produces ammonia, fertilizer) and Eleme Petrochemical Company, established in 1985 which produces polyethylene materials. In addition to serious water pollution and land degradation problems, these mega-industries continuously emit known and unknown gases into the environment with impunity. Data for the study were obtained from two sources. The first group was obtained from the three air monitoring stations in the area for a period of three years. (January 2003 to December 2005). In this regard, four criteria pollutants were examined: nitrogen dioxide (NO2), sulphur dioxide (SO2) carbon monoxide (CO) and small particulate matter (PM10). The choice of these four pollutants was predicated on the fact that data from these stations indicated high concentrations of these gases with NO2 exceeding 88µg/m3, being six times more severe than in neighboring towns (Calabar, Owerri, Enugu) with exceedances of half-hour standards occurring hundreds of times each year. SO2 levels exceeded 50 ug/m3 especially around the industrial sites with high concentrations for short periods. Particulate matter levels exceeded 70 µg/m3 annually. For CO, the annual averages ranged between 1.3 µg/m3 to 1.83 µg/m3. Although exceedances of the Federal Environmental Protection Agency (FEPA) standards were not recorded, the high concentrations of CO were not recorded during rainy season due to unstable meteorological conditions.The second source was data from on-the-spot measurements at each of the six schools and residential area locations with portable air monitors (Multi Gas Analyzer MRU-Model 2002) to compare with values obtained from local monitoring stations. Measurements were carried out 8 h. and with 1 h. and half-hour intervals on daily basis during the survey period.This helped to identify the sampling locations with the highest and lowest concentration levels at any given time. The frequency of measurements and number of monitors were the same for each of the pollutants during the entire survey period. The sampling was carried out during the two seasons of the year (rainy and dry seasons) to enable the assessment of the influence of humidity and dry atmosphere on ground level concentrations of measured pollutants. The values obtained from on-the-spot assessment showed that those obtained from monitoring stations were consistent and reliable. The dominant wind direction was mainly towards south-west in the rainy season and north east in the dry season while the wind speed averaged between 0.4 m/s and 3.4 m/s. This means that pollutants emitted from the industries were driven by gentle breeze along major wind corridors (roads, streets). These results indicate that the local population is exposed to high levels of these pollutants for quite some time. The population of six primary schools with pre-nursery facilities were used for the study. Four of these schools are located within 3 km radius from the emitting industries, while the other two were about 5km apart. Children in the former (labeled zone A) are those more exposed to industrial emissions while the latter (labeled zone B) are in the less exposed area. Distance from sources of emissions was therefore an important factor in the exposure assessment (Hochadel et al., 2006). A total of 250 children participated in the study; they were in three groupings: less than 2 y, 2 to 3 years, and 4 to 5 y. Of this total, 200 were drawn from zone A and 50 from zone B. The socioeconomic status of the children such as income levels of parents, housing density, feeding habits, area of residence, respiratory diseases of parents, smoking habits and education level of parents etc, were all recorded and included in the analysis. For a period of 18 months (February 2005 to July 2006) with the collaboration of school authorities and Ministry of Health Officials, these subjects were thoroughly monitored and clinically examined (pulmonary function test, body temperature, presence or absence of cough, etc) by the medical team. Each child had a folder for recording all respiratory symptoms and diseases suffered such as cough, cold, sinusitis, bronchitis, and cough with phlegm. Subjects were examined on weekly basis between 11H and 13H when gaseous emissions were highest. Those enrolled for the study were granted permission by their parents, who completed a questionnaire bothering on their socio-economic status and disease history. Examinations were carried out according to World Medical Association standards. Data were analyzed using mixed-effect models with random subject effects accounting for repeated measures. Covariates were chosen based on previous literature identifying potential risk factors for diseases and symptoms exposure. In the first level of analyses, linear and logistic models were applied for the four pollutant gases combined to estimate whether associations exist. Similar models were also applied for diseases and symptoms exposure including all potential covariates but excluding pollution variables to verify whether associations exist (e.g. whether children's residence or school locations associated with symptoms and diseases). The four air pollutants were then incorporated into the models to investigate their effects on children's health with regards to symptoms and diseases. After the zone-specific data were analyzed, the heterogeneity between the two zones (A and B) was assessed. Also, the effect of distance from sources of pollution emissions and age of subjects were examined as to whether they modified the effects of the four air pollutants on the diseases and symptoms of subjects. For categorical exposure variables, odds-ratios (ORs) were used to assess the associations between pollutants, symptoms and diseases, and adjustments for other potential confounders. Linear models analyzing exposure for each of the two seasons of the year were also applied. Sensitivity analyses were performed to explore the robustness of the models by using a more parsimonious and extended models. Data were analyzed using the statistical package SAS version 9.1 (SAS Institute Inc, Cary, NC, USA). RESULTS AND DISCUSSIONResults of the socio-economic status of the children showed notable disparities as shown in Table 1. While the highest monthly income of parents was largely above N 100,000, the least paid parent earned around N 20,000. The highest paid parents lived within zone A, the highly exposed area while the most poorly paid ones lived in zone B. Similar differences were observed in the housing conditions of parents. Most houses within zone A were well ventilated, dispose of potable water, electricity and conveniences, quite unlike those in zone B; who live in poorly ventilated houses, lacking in most of the facilities mentioned above. In addition, 80 % of parents in zone A had post-secondary education, while in zone B, only 30 % of them attained to this level with the majority having only elementary education especially the mothers. However, 95 % of all the parents were working in the industries in the area. There were significant differences in the frequency of symptoms and diseases observed among children in the two zones. Out of a sample of 250 subjects, a total of 88 cases of various symptoms and diseases of cold, sinusitis, bronchitis, cough, cold or phlegm was recorded during the survey period. Among the victims 93.2 % or (82 cases) were children schooling in zone A while the remaining 6.8 % (6) were in zone B. Table 2 shows that children manifested different symptoms and diseases at variable rates in the two zones. For example, children residing in zone A are 1.3 times more likely to suffer from cough with phlegm than those in zone B; 3.3 times to suffer from cough; 3.7 times to suffer from sinusitis, and 1.8 times to suffer from cough and cold, and 1.9 times to suffer from bronchitis than those in zone B. These results show the role of proximity to sources of emissions and their impact on the respiratory health of the children. There were variations in the symptoms and diseases among subjects over time and space. Zone A, the more exposed area recorded a quantum increase in all these manifestations than zone B. A comparative analysis of the zones show that in February 2005, 12 % of the children in zone A suffered from cold while it progressed to 18 % in March 2006 and then fell to 16 % in July 2006. The same trend was observed for cough which increased from 10 % in February 2005, to 12 % in April 2006; and then to 24 % in July 2006; bronchitis from 8 % in February 2005 to 14% in July 2006, sinusitis from 12% in February 2005 to 18 % in September 2006, while cough with phlegm from 14 % to 20 % within the same period. With the exception of cold that progressed from 8 % in February 2005 to 10 % in May 2006 none of the other symptoms and diseases exceeded 4 % increase in zone B during the period. The calculations therefore revealed that for the 18 month period, zone A recorded the highest increase of 50 % of subjects who suffered from cold, 140 % for sinusitis and 42.8 % for cough with phlegm. Comparatively zone B recorded the following increases: cold 2 %, bronchitis 1%, sinusitis 1.6 %, cough with phlegm 2 % and cough 2.6 %. Also, a trend of lower pulmonary function was noted among children living in zone A the highly exposed area than in zone B, the less exposed area. Results from statistical analyses revealed a high positive correlation between pollution levels and morbidity rate; it was significant at 0.05 level and positive (0.8). This positive coefficient indicates that the area especially the highly exposed zone A, experienced emissions from specific sources, with no regulatory effort to reduce their levels. The correlation between exposure to NO2 and SO2 was 0.63, and between NO2 and PM10 was 0.55. For each of the gases considered, it was observed that SO2 correlated with cough and cold in all seasons (0.86) and NO2 correlated with bronchitis (0.62). PM10 correlated with cough and sinusitis (0.67 and 0.53). Also in the two seasons, the strongest correlation for bronchitis were with NO2 (0.83) and SO2 (0.76). Correlations during seasonal exposures (dry and wet seasons) were 0.72 and 0.66 for NO2, 0.76 and 0.53 for SO2, 0.57 and 0.21 for PM10 and 0.13 and 0.25 for CO. No statistical difference was observed between the effect estimate based on the sex of the children. There was a strong association between air pollution and symptoms and diseases in the overall sample (OR = 3.0, 95%, CI 1.8 7.5). However, this association varied according to the subsets of the subjects based on age and distance from emission sites. It was strongest for children under 2 years (adjusted OR = 3.5, 95 %, CI 1.17 8.3) than those above 3 years in zone A (OR =2.3, 95 %; CI 1.5 -5.2) and those in zone B (OR = 2.1, 95 %, CI 1.3 4.7). Exposure estimates for the four pollutants covaried. At Elemearea, pollutant gases are emitted almost on daily basis from the mega industries, but these emissions quickly dissipate into the surrounding environment. The absence of a strong wind, despite its coastal location led to heavy concentration of pollutants, although with occasional eddies circulating them within the built-up areas along wind corridors. As none of the children showed hematological, renal or central nervous system symptoms, the exposure route was largely suspected to be respiratory inhalation of the pollutant gases which provoked systemic reactions in the children exposed to them. For example 45 children suffered triple episodes of cold, 33 children double episodes of cough and 35 children double episodes of bronchitis. All these episodes were quite similar in their clinical courses with duration of most of these symptoms/diseases between 4 to 9 days. The toxic properties of each of the pollutants examined showed that NO2, SO2 and PM10 were the major pollutants as they matched the criteria for the causative agents in the current cases. As strong oxidizing agents NO2 and SO2 act as irritants that damage delicate tissues in the respiratory passages. The inhallatory response set in motion by these irritants impair lung functioning and trigger the observed symptoms and diseases (Abbasi and Vinthan,1997). It is known that oxides of sulphur especially SO2 affect the ability of respiratory tract to clear out foreign particulate matter and badly damage it. Particulate matter can also aggravate existing respiratory diseases and impair defense system of body causing greater susceptibility to disease (Khitoliya, 2004). However, it is equally possible that the children suffered from the synergistic interactions of complex gaseous emissions, known and unknown, in the area which they are continuously exposed to (Simmons et al., 1994). The phenomenon of clustering children at school over a long period of time (8.30 am to 5.30 pm) within a radius of 5 km. in a highly polluted zone suggest a possible association of the diseases and symptoms with exposure to the pollutants. It is also possible that parents who mainly work in these industries may have continuously brought residues of these pollutants home to further increase exposure levels of children especially among those who have unique susceptibilities to high frequencies of exposure (Curl et al., 2002; Hutzinger, 1992). This study has tried to show the effect of air pollution on the respiratory health of children in Eleme industrial area of Port Harcourt city. Results revealed a strong association between air pollution and respiratory diseases and symptoms among subjects. It showed that the most probable pathway through which the subjects are affected is inhalation. It also showed that NO2, SO2 and PM10 are the most probable air pollutants as they matched the criteria for the causative agents in the considered case. However, further study in the area is necessary for confirmation. Children below 2 years of age are twice likely to be affected by continued exposure, as the higher the age the lesser the susceptibility to the pollutants. The total absence of air quality guidelines in the area increases the risk of continuous exposure to vulnerable groups such as children and the elderly. In fact there was a generally monotonic increase in susceptibility with decreasing age of the children. The results of this research are novel in the area of air pollution in the south eastern Nigeria in general and in Eleme in particular.The scientific and health communities will find them useful especially as they show the important gradients of the impact of air pollutants on children. The results may also be useful to support conclusions on regulatory actions on air standards in a highly polluted area as Eleme where there is absence of extensive large network of monitoring stations that collect data on atmospheric pollution. Finally, these findings therefore suggest that the determination of air quality guidelines designed to protect the general population in the area may be insufficient to protect babies and children. Air pollution data and results of analyses indicate that the levels of concentration of the pollutants will continue to increase to the detriment of the most vulnerable groups including children.The study is not without limitations as alternative explanations should be considered for these general findings.It is possible that confounding socioeconomic variables of parents biased the results. It is also possible that the four criteria pollutants examined are correlated with other known and unknown contaminants emitted from these industries. For example, the study did not consider the possibility of bacterial contamination.The analysis was done only on a subset of the population and thus might not have been representative of the entire population. In spite of these shortcomings, the results obtained from this study should serve, not only as a warning to local and national authorities on the severity of the problem of air pollution in Eleme, but also as a starting point for further research on this growing problem in most metropolises in the country. ACKNOWLEDGMENTS The authors are grateful to the authorities of the Federal University of Technology, Owerri in Nigeria for their contributions, especially in making funds available throughout the period of the research. Many thanks also go to the Dean of the Faculty of Engineering and Engineering Technology of the same university for his encouragements. The authors are also grateful to Miss. Oluchi Nwachukwu for typesetting the document. REFERENCES
© IRSEN, CEERS, IAU The following images related to this document are available:Photo images[st08057t1.jpg] [st08057t2.jpg] |
| |||||||||

{kind=link}
{kind=link}