 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
International Journal of Environment Science and Technology, Vol. 7, No. 4, 2010, pp. 705-716 Noise pollution and its effects on medical care workers and patients in hospitals 1* D. F. Juang; 1C. H. Lee; 1T. Yang; 2M. C. Chang 1Department of Health Business Administration, Meiho University,
24F, 230, Ming-Chuan Second Road, Kaohsiung
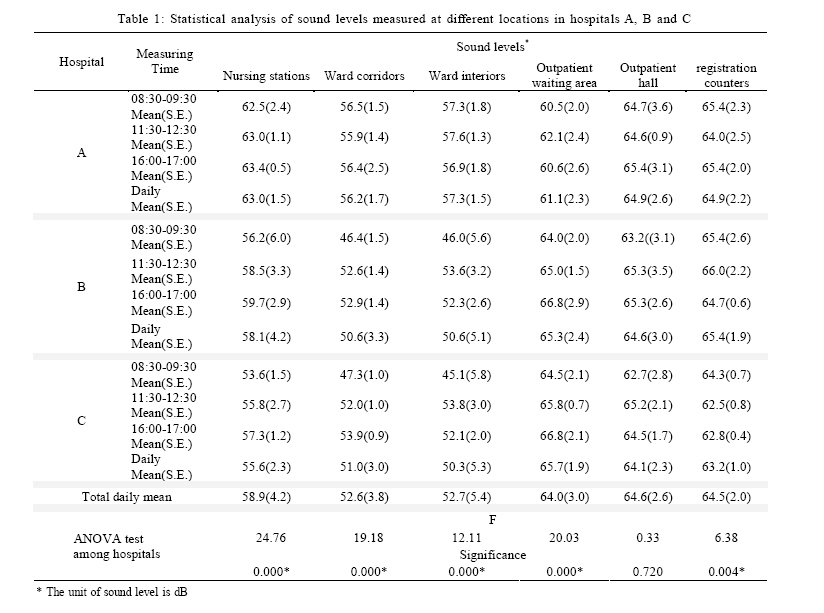
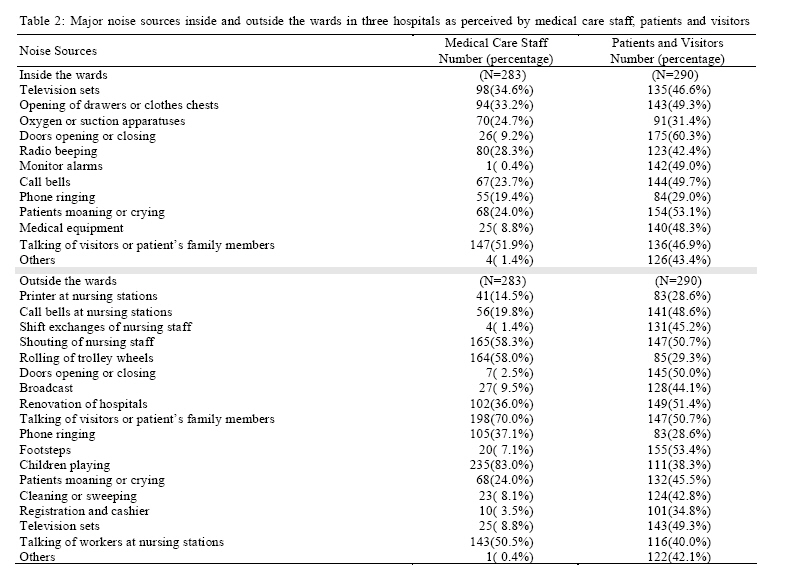
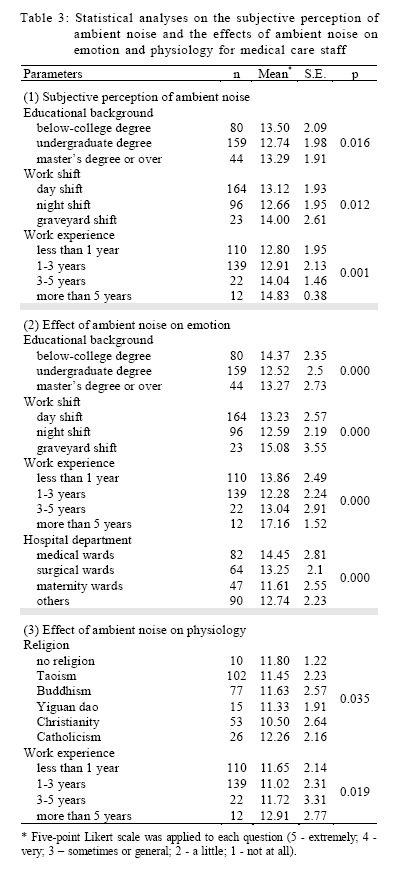
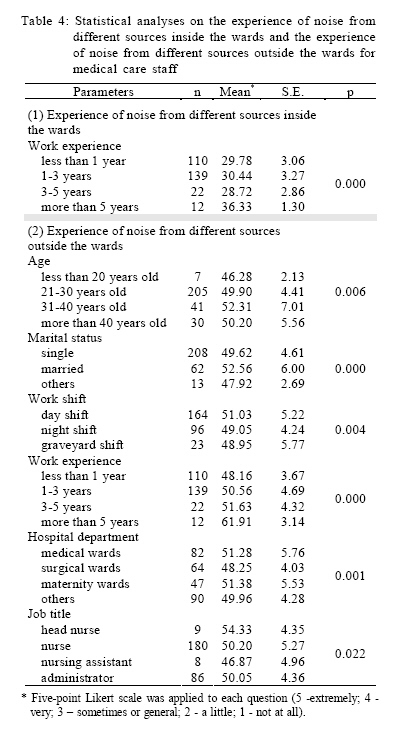
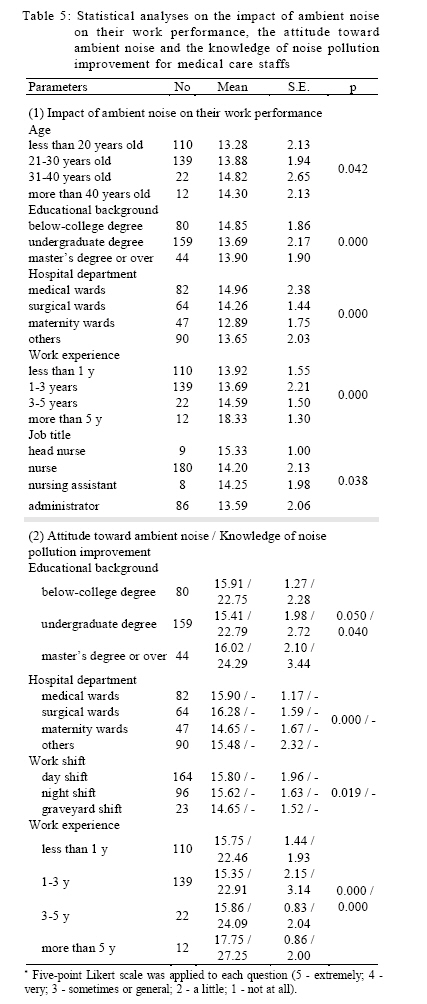
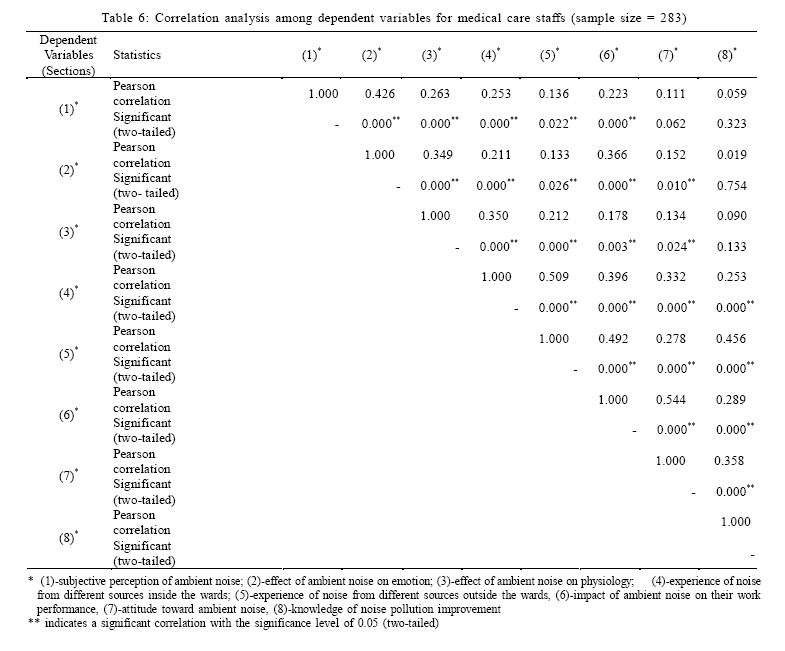
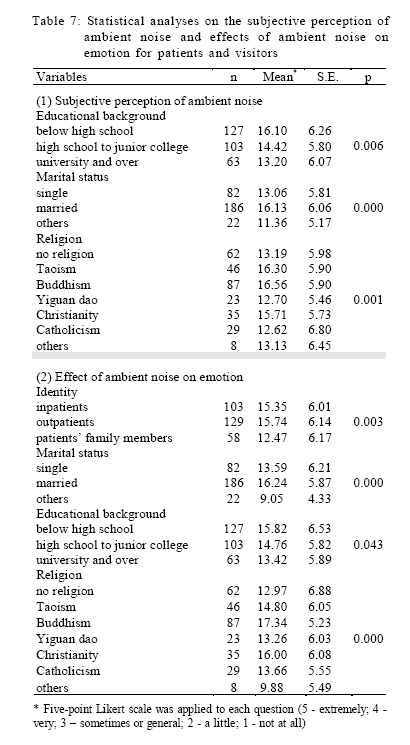
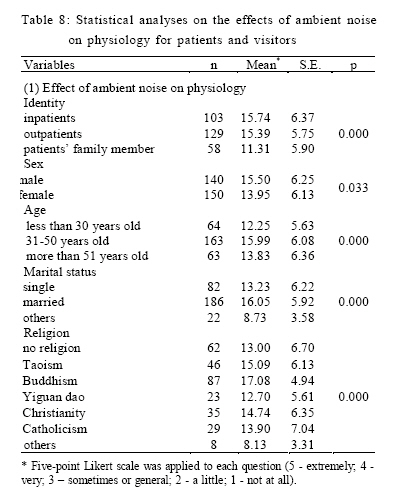
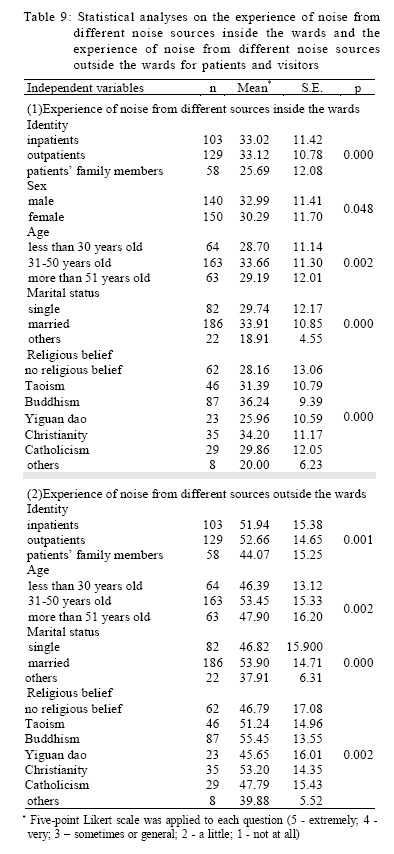
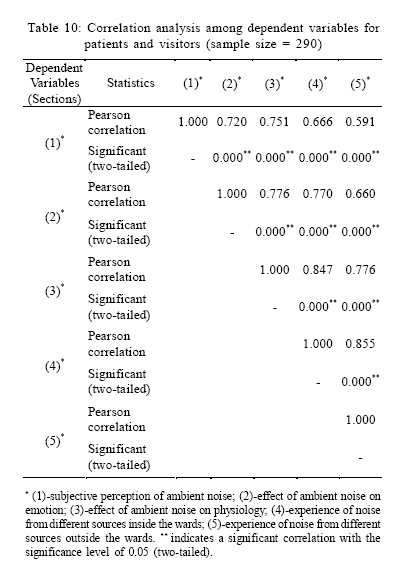
806, Taiwan *Corresponding Author Email: x00002060@email.meiho.edu.tw Tel.: +886 8779 9821; Fax: +886 8778 0673 Received 24 May 2010; revised 17 June 2010; accepted 25 July 2010 Code Number: st10070 ABSTRACT: The objectives of this study are to investigate the levels of noise pollution in some hospitals in Taiwan and to study the effects of noise pollution on the physiological and psychological reactions and annoyance response of medical care staff, patients and visitors in these hospitals. An instrument for the measurement of sound level was used and a self-answered survey questionnaire on noise pollution was administered. Results showed that the daily average sound levels measured inside these hospitals during daytime were between 52.6 and 64.6 decibels. These are higher than the current daytime environmental noise limit of 50 decibels in Taiwan. Most nursing staff members expressed that "talking of visitors or patient's family members" is the major source of noise inside the wards, whereas "talking of visitors or patient's family members" and "children playing" are the two major noise sources outside the wards. However, most patients or visitors claimed that "doors opening or closing" and "patients moaning or crying" are the two major sources of noise inside the wards. "Footsteps," "renovation of hospitals," "talking of visitors or patient's family members," "shouting of nursing staff" and "doors opening or closing" are the five major noise sources outside the wards. To conclude, noise pollution inside and outside the wards either directly or indirectly affects, in a simultaneous manner, the subjective perception of noise, emotions, physiology and experience of noise inside and outside the wards of both the medical care staff and the patients and visitors. Keywords: Ambient noise; Annoyance response; Sound levels; Subjective perception INTRODUCTION The health effects of noise pollution have been studied by many researchers in recent years. Some researchers studied the impact of environmental noise on exposed population (Ising and Kruppa, 2004; Piccolo et al., 2005; Tang and Wang, 2007; Banerjee, 2008; Banerjee, et al., 2009; Monazzam and Nassiri, 2009; Omidvari and Nouri, 2009), while some others investigated the risk of workers exposed to noise pollution in different working places (Nassiri and Golbabai, 1993; Giardino and Durkt, 1996; Morrison et al., 2003; Yildirim et al., 2007; Roozbahani et al., 2009). Many studies have revealed that extended exposure to noise pollution may cause auditory and non-auditory disorders, such as temporary or permanent hearing loss (Selfe, 1982; Willett, 1991; Nassiri and Golbabai, 1993; Yildirim et al., 2007; Keipert, 2008), sleep disruption (Freedman et al., 1999; Freedman et al., 2001), vertigo, agitation, weariness, hypertension, gastrointestinal system problems (including gastric and duodenal ulcer), cardiac arrhythmia, nervous and psychic disorders (Nicholas et al., 1993; Buemi et al.,1995; Job, 1996; Holmberg and Coon, 1999; Van Kempen et al., 2002; Ising and Kruppa, 2004; Penney and Earl, 2004; Roozbahani et al., 2009) and so on. Therefore, it is very important that medicare givers should provide a quite environment for the patients since unwanted sound could have a negative impact on patient outcomes. However, Meyer-Falcke et al. (1994) depicted that the maximum sound level of the technical equipment was even surpassed by avoidable background noise caused by the staff in the surgical intensive care unit and the anaesthetic and recovery room. They also concluded that sound level was low in dangerous situations and high during routine work. Allaouchiche et al. (2002) found staff conversation caused 56 % of sounds greater than 65 dB and other noise sources (alarm, telephone, nursing care) were each less than 10 % of these sounds. Ulrich and Zimring (2004) indicated that many studies have reported high noise levels in most hospitals in USA. They reviewed these articles and summarized two general sources of noise in hospitals. First one is the noises from paging systems, alarms, bedrails, telephones, staff voices, ice machines, pneumatic tubes, carts and roommates. Second one includes the surfaces of the floors, walls and ceilings hospitals which usually are hard and reflect sound rather than absorb it. Cmiel et al. (2004) reported noise is a primary cause of sleep deprivation and disturbance among patients and it increases their anxiety and decreases their confidence in the clinical competence of the staff. They believed prolonged exposure to environmental noise can increase anxiety and stress, ultimately impacting patient safety. Blomkvist et al. (2005) also studied the effects of noise pollution on the patients in a coronary critical care unit and found that the patients judged healthcare worker attitudes and care to be much better during the lower acoustical periods. Therefore, it is very important to keep the noise levels down in medical institutions. Medicare givers should provide a quite environment for the patients and the staffs, since unwanted sound could have a negative impact on patient outcomes and caregiver effectiveness. However, Allaouchiche et al. (2002) found staff conversation caused 56 % of sounds greater than 65 dB and other noise sources (alarm, telephone, nursing care) were each less than 10 % of these sounds. A review article reported by Ulrich and Zimring (2004) indicated that many studies have shown that noise levels in most hospitals in USA are much higher. They pointed out two general sources of noise in hospitals. The first one includes paging systems, alarms, bedrails, telephones, staff voices, ice machines, pneumatic tubes, carts, and noises generated by roommates. The second source includes the surfaces of the floors, walls, and ceilings which usually are hard and reflect sound rather than absorb it. Blomkvist et al. (2005) studying a coronary critical care unit found that healthcare workers exposed to different levels of noise over the workday reported higher levels of stress and tension. Conversely, the patients judged staff attitudes and care to be much better during the lower acoustical periods. Therefore, it is very important to keep the noise levels down in medical institutions. The United States Environmental Protection Agency (USEPA) recommended guideline values for continuous background noise are 45 dB during the day and 35 dB at night in patient rooms. World Health Organization (WHO) also recommended guideline values for continuous background noise in hospital patient rooms are 35 dB, with nighttime peaks in wards not to exceed 40 dB ( Berglund et al., 1999 ). According to the Noise Control Act of Taiwan, the background noise limit for a medical institution is 50 dB at daytime and 40 dB at nighttime. However, the limit only applies to areas surrounding the institution, rather than inside it. Labor safety and sanitation rules in Taiwan stipulate that the amount of time allowed for exposure to noise measuring 90 dB is 8 h daily. It further classifies a working place with noise of above 85 dB as a hazardous working environment. Soutar and Wilson (1986 ) reported that the average noise levels in the psychiatric, general medical and acute admitting wards are 49, 68 and 66 dB(A), respectively. Average noise levels from 07:00 to 23:00 in the general and acute medical wards were almost identical. Bayo et al. ( 1995 ) found most noise equivalent sound levels exceeded 55 dB (A) in one major hospital in Spain. After a self-answered questionnaire on 295 medical care staffs, the results revealed that the most important noise sources were located primarily inside the hospital. Most workers perceived that noise levels are sufficiently high to interfere with their work and affect patients' comfort and recovery. Buemi et al. (1995) also reported during the day time the maximum sound level at the intensive care unit, hemodialysis room and corridor are 76.8 dB (A), 67 dB (A) and 66.8 dB (A), respectively. Ann et al. (1996 ) measured and evaluated the noise levels in hospital environment and claimed that the average noise value was 60 dB (A), which is much higher than those suggested by USEPA (45 dB during the day and 35 dB at night). The results of their questionnaires also showed that 58 % of patients believed their sleep had been interfered by the noise from staff, equipments and other patients. Morrison et al. (2003) measured the average daytime sound level in a pediatric intensive care unit was 61 dB (A), nighttime 59 dB (A). Some researchers reported noise levels in the range of 100 dB to 110 dB from drills, saws and other equipment in operating room were found and this presents a significant risk for noise-induced hearing loss (Love, 2003; Nott and West, 2003). Kracht et al. (2007) analyzed the noise in the operating rooms of Johns Hopkins hospital and found orthopedic surgery has the highest average equivalent sound level of approximately 66 dB (A). They also found neurosurgery, urology, cardiology and gastrointestinal surgery have the average equivalent sound levels ranging from 62 to 65 dB(A). However, the peak levels for neurosurgery and orthopedic surgery exceeded 100 dB over 40% of the time and the highest peak levels routinely seen during surgery were well in excess of 120 dB. Sobotova et al. (2007) conducted a measurement of noise levels in a hospital environment and concluded that equivalent noise levels (LAeq = 71.3 dB; LAeq,8h = 68.3 dB) during orthopedic surgery highly exceeded the limits for a hospital environment; the maximal noise levels reached up to 85 dB (A). In selected hospital wards, equivalent noise levels reached up to 58.7 dB (A). Their questionnaire survey results also showed that 64 % of hospital staff members were annoyed by noise at work and 10 % were highly annoyed. Traffic and stationary sources outside the hospital premises and surgical and other equipment inside the hospital, were altogether considered as the main source of noise. Similar results were obtained by Chen et al. (2009) in a series of measurements on noise levels at the lobbies of 11 comprehensive hospitals in central part of Taiwan. They found that noise levels averaged from 60 to 65 dB (A). A noise level questionnaire was administered as well by the said authors and their results showed that the noise levels derived from the psychological survey correlated well with the cumulative rate of noise. Their findings indicate further that the functioning of the lobby, which is typically designed to have complex functions corresponding to special architectural planning, always results in higher noise in hospitals. These manifest as noise levels, which correlate with the cumulative rate of noise. Therefore, in order to gain better understanding of the sound levels in the different hospital units in Taiwan, as well as to determine how noise affects patients, visitors and the medical care workers, three hospitals were selected in central and southern part of Taiwan. Measurements on sound levels were employed. A self-answered survey questionnaire on the experiences of noise was administered as well. MATERIALS AND METHODS Hospital samples One regional hospital (Hospital A) was identified in the central part of Taiwan and two regional hospitals (Hospital B and Hospital C) in the southern part of Taiwan, with 960, 645 and 498 ward beds, respectively. Medical care personnel (including nurses and administrators), patients and visitors (including patients' family members) were selected randomly and asked to participate in the noise survey. Measurement of sound levels Sound levels were measured using the Lutron sound level meter (Model 4030), with the measuring height fixed at about 1.5 m above ground surface. This measuring device was calibrated every time before use. Several locations in each hospital were selected for sound level measurements, including nursing stations, ward corridors, ward interiors, registration counters, outpatient waiting area and outpatient hall. Measurements were taken in triplicate (i.e., at time intervals of 0830-0930 h, 1130-1230 h and 1600-1700 h) on a daily basis. From the triplicate measurements of each time interval, the average was computed. The obtained averaged values were then used for further analysis. Measurement of sound levels were carried on a daily basis, from August 18 to August 22, 2007 in Hospital A; August 11 to August 15, 2007 in Hospital B and July 21 to July 25, 2007 in Hospital C. Questionnaire survey on noise experience A structured questionnaire was prepared to obtain the physiological and psychological reactions and annoyance responses of the medical care staff and the patients and visitors (including inpatients, outpatients, and patients' family members) to the noise pollution in hospitals. The independent variables (demographic characteristics) for both the medical care staff and the patients/visitors included the following: identity (nursing staff, administrator, inpatient, outpatient, and patient's family), sex, age, marital status, religion, and educational background. However, in the questionnaire, four independent variables, namely, hospital department, work shift, work experience, and job title, were applicable only to medical care staff. The dependent variables for medical care staff included 62 questions and divided into nine sections: (a) the sources of noise (Section 1: two questions involving the noise sources from inside the wards and outside the wards); (b) subjective perception of ambient noise (Section 2: five questions involving distress, inattention, inability to sleep, fright, and dizziness caused by ambient noise); (c) effect of ambient noise on emotion (Section 3: five questions involving communication difficulty, scalp tingling, bad temper, irritable mood and increase in pressure); (d) effect of ambient noise on physiology (Section 4: five questions involving tachycardia, tinnitus, headache, susceptibility to fatigue and loss of appetite); (e) experience of noise from different sources inside the wards (Section 5: eleven questions involving sources, such as television sets, opening of drawers or clothes chests, oxygen or suction apparatuses, doors opening or closing, radios beeping, monitor alarms, call bells, phones ringing, patients moaning or crying, medical equipment and talking of visitors or patient's family members); (f) experience of noise from different sources outside the wards (Section 6: seventeen questions involving noise sources, such as printers at nursing stations, call bells at nursing stations, shift exchanges of nursing staff, shouting of nursing staff, rolling of trolley wheels, doors opening or closing, broadcast, renovation of hospitals, talking of visitors or patient's family members, phones ringing, footsteps, children playing, patients moaning or crying, cleaning or sweeping, registration and cashier, television sets and talking of workers at nursing stations); (g) impact of ambient noise on their work performance (Section 7: five questions involving the impact of noise on work efficiency, thinking, degree of obedience, auditory masking, and inattention); (h) attitude toward ambient noise (Section 8: five questions on patients' feelings about noise, considering the sources of noise and reporting to the superintendent or concerned unit, keeping a stable state of mind, considering noise control or persuading to reduce noise volume, and considering ear hearing check regularly) and (i) knowledge of noise pollution improvement (Section 9: seven questions regarding the requirement of adequate maintenance of equipment for noise control and the requirement of explicit and effective management of noise, improving and promoting the noise prevention knowledge of patients, improving and promoting the noise prevention knowledge of visitors and patient's families, improving the noise pollution problems during the daytime, improving noise pollution problems at night and directly advising persons who make noise to minimize it). The dependent variables in the questionnaire for patients and visitors included only six sections (total: 45 questions), which were exactly the same as Sections 1 to 6 for medical care staff. Except for the Section 1, the five-point Likert scale was applied to each question in all of the sections (5 extremely; 4 very; 3 sometimes or general; 2 a little; and 1 not at all). Statistical analysis The survey commenced on July 7, 2007 and completed on August 2, 2007. A total of 300 questionnaires for medical care staff (with 100 questionnaires for each hospital) and 300 questionnaires for patients and visitors (with 100, 80, and 120 questionnaires for Hospitals A, B, and C, respectively) were distributed. The valid returned questionnaires were 283 (98, 90 and 95 for Hospitals A, B, and C, respectively) for medical care staff, and 290 (95, 79, 116 for Hospitals A, B and C, respectively) for patients and visitors. The questionnaire passed the validity and reliability tests before distribution. The Cronbach's alpha values of the questionnaire for the medical care staff and for the patients and visitors were 0.861 and 0.978, respectively. All statistical data analyses were completed using the SPSS 14.0 software. RESULTS AND DISCUSSION Sound levels in hospitals Table 1 shows the statistical analysis of sound levels measured at different locations in Hospitals A, B, and C. Apparently, the noise was higher in the following locations for all the hospitals: outpatient waiting area, outpatient hall, and registration counter was higher than that at the locations of medical nursing station, medical ward corridor, and medical ward interior. The aforementioned was the general situation, except for the medical nursing station in Hospital A, which had a daily average sound level of 63.0 dB. The sound levels in the medical nursing station, medical ward corridor, and medical ward interior in Hospital A were also higher compared in those in Hospitals B and C. The results from analysis of variance (ANOVA) on the three hospitals showed that the sound levels in the medical nursing station, medical ward corridor, medical ward interior, outpatient waiting area, and registration counter had significant difference (p < 0.05). The average sound levels measured in these hospitals during daytime were between 52.6 and 64.6 dB, a range similar to those previously reported by other works ( Bayo et al., 1995; Ann et al., 1996; Kracht et al., 2007; Chen et al., 2009 ). However, all of the sound levels measured in the hospitals in the present study were much higher than those suggested by USEPA (i.e., 45 dB during daytime). Although the Noise Control Act in Taiwan has not yet expressed clearly the required noise limits inside hospitals, the measured noise levels in this study were still higher than the noise limits for first-class noise control areas, such as hospitals (i.e., 50 dB during the daytime). Analysis of major noise sources Table 2 shows the major noise sources inside and outside the wards of Hospitals A, B and C as perceived by the medical care staff and by the patients and visitors. The surveyed workers in these hospitals conveyed a similar opinion on the major sources of noise (data not shown). According to the data gathered, 51.9 % of nursing staffs mentioned that "talking of visitors or patient's family members" is the major source of noise inside the wards. Meanwhile, 58.3 %, 58.0 %, 70.0 % and 83.0 % of them expressed "shouting of nursing staff," "rolling of trolley wheels," "talking of visitors or patient's family members," and "children playing," respectively, are the four major sources of noise outside of the wards. More than 50 % of surveyed patients and visitors considered "doors opening or closing" and "patients moaning or crying" as the two major noise sources inside the wards. Outside ward premises, they consider "shouting of nursing staff," "doors opening or closing," "renovation of hospitals," "talking of visitors or patients' family members," and "footsteps" as the major sources of noise. Although these results were not quite similar to those previously observed by Ulrich and Zimring (2004), hospitals in Taiwan should improve their patient visiting programs in order to reduce the noise from "talking of visitors or patient's family members" or "children playing." In addition, publicity materials or warning signs for noise control should be posted in prominent locations and even outside hospital wards. Certainly, hospitals should periodically provide nursing staff with educational courses on noise control in order to reduce the noise from "shouting of nursing staff" and "rolling of trolley wheels." Survey on sound level among nursing staffs Student's t-test and ANOVA were used to determine the relationship between each demographic characteristic (independent variable) and each dependent variable. Table 3 shows the results of statistical analyses on the subjective perception of ambient noise, as well as the effects of ambient noise on emotion and physiology. Medical care staff working on graveyard shift or have longer work experiences displayed more sensitivity to noise. Nursing staff with undergraduate degrees appeared less sensitive to noise compared with those with master degrees or below-college degrees. Staff members with below-college degrees and nurses working in medical wards claim that ambient noise have more significant effects on their emotions while at work. In addition, medical care staff working on graveyard shift or have more than five years work experience expressed that their emotions at work could be affected seriously by ambient noise. Staff members who were Christians claim that ambient noise has less effect on their physiology while at work. Furthermore, medical care staff with more than five years of work experience deemed that ambient noise has more effect on their physiology at work. Results in Table 4 (only the results showing significant differences are listed) show that most of the staff members with more than five years of work experience expressed that noise from different sources inside the wards was very high. However, staff members between 31 and 40 years old, married, worked the day shift, with more than five-year work experience, or were head nurses considered noise levels from different sources outside ward premises as very high. Staff members working in surgical wards claim that the noise levels from different sources outside the wards may not be so high. Most medical care workers perceive noise levels outside the wards as much higher compared to inside ward premises. Results in Table 5 (only the results showing significant differences are listed) show that staff members aged between 31-40 or more than 40 y are more susceptible to the impact of noise on their work performance. Similarly, staff members with below-college degrees, deployed in medical and surgical wards and with more than five-year work experience displayed more susceptibility to the impact of noise on their work performance. In contrast, administrators were less sensitive to the effect of noise on their work performance. Medical care staff with at least a master's degree and who have more than five years of work experience showed better attitude towards ambient noise. However, both staff working in maternity wards and staff working in graveyard shift expressed aversion towards ambient noise. In addition, staff with at least a master's degree and staff who have more than five-year work experience had better knowledge on noise pollution improvement. Correlations for all dependent variables were evaluated (Table 6). Results showed that most of the dependent variables presented significant correlations (p < 0.05), except for the correlations between "subjective perception of ambient noise" and "attitude to ambient noise"; "subjective perception of ambient noise" and "knowledge of noise pollution improvement"; "effects of ambient noise on emotion" and "knowledge of noise pollution improvement" and "effects of ambient noise on physiology" and "knowledge of noise pollution improvement." Findings indicate that noise pollution either directly or indirectly affects, in a simultaneous manner, the subjective perception of noise, emotion, physiology, experience of noise levels inside and outside ward premises, work performance and attitude to ambient noise of the medical care staff. Survey on sound level among patients and visitors Similar to the analysis for medical care staff, results show that patients or visitors who have lower educational attainments displayed more sensitivity to noise (Table 7). Likewise, patients or visitors who are married or who are Taoists or Buddhists appeared more sensitive to noise. Inpatients also displayed stronger reactions on their subjective perception of ambient noise compared with outpatients and visitors. However, both inpatients and outpatients expressed that ambient noise in hospitals has more significant effect on their emotion. Ambient noise in hospitals was also shown to have more significant effects on the emotions of married people and individuals with lower educational levels. Again, patients and visitors who are Buddhists or Christians mentioned that ambient noise has a more significant effect on their emotions. The effects of ambient noise on the emotions of inpatients were also more significant compared with those among outpatients and visitors. Table 8 shows the statistical analyses results of the effects of ambient noise on physiology (only the results showing significant differences are listed). Apparently, ambient noise in hospitals has a more significant effect on the physiology of inpatients and outpatients physiology compared with the visitors. Ambient noise in hospitals also has more significant effects on the physiology of male patients or male visitors compared with their female counterparts. Results also showed that ambient noise in hospitals has a more significant effect on the physiology of patients and visitors aged 3150 years or married. Again, ambient noise was expressed to have a more significant effect on patients and visitors who are Buddhists as opposed to those with other religions. The effects of ambient noise on the physiology of inpatients were much higher compared with those of the outpatients and visitors. Table 9 shows the statistical analysis results of the experiences of noise levels from different noise sources inside and outside the wards (only the results showing significant differences are listed). Both inpatients and outpatients experienced higher noise levels from various noise sources inside the wards as opposed to the visitors. Patients and visitors aged 31-50 years, married, and Buddhists or Christians also experienced higher noise levels from the different noise sources inside ward premises. Similarly, both inpatients and outpatients experienced higher noise levels from different noise sources outside the wards compared with the visitors. Patients and visitors aged 31-50 years, married and Buddhists or Christians also experienced higher noise levels from different noise sources outside ward premises. The correlations of the dependent variables for patients and visitors were also evaluated (Table 10). Results showed that all of the dependent variables presented significant correlations (p < 0.05), indicating that noise pollution either directly or indirectly affects, in a simultaneous manner, the subjective perception of noise, emotions, physiology and experience of noise levels inside and outside the wards of the patients and visitors. CONCLUSION In this study, it was found that the average sound levels measured in Hospitals A, B, and C during daytime were between 56.2 and 64.9 dB, between 50.6 and 65.4 dB, and between 50.3 and 65.7 dB, respectively. These values were higher than the environmental daytime noise limit of 50-dB requirement in Taiwan, and certainly surpass the USEPA guideline value of 45 dB at daytime. The results of this study imply that the hospitals in Taiwan should improve their patient visiting programs in order to minimize noise pollution from major sources, such as "talking of visitors or patient's families" and "children playing." In addition, publicity materials or warning signs for noise control should be posted in prominent locations, even outside hospital wards. Hospitals should also provide their respective nursing staff workers periodical educational courses on noise control in order to reduce the noise from "shouting of nursing staff" and "rolling of trolley wheels." As expressed by the medical care staff and by the patients and visitors, significant correlations were found in relation to subjective perception of ambient noise, effect of ambient noise on emotion, effect of ambient noise on physiology, and experience of noise levels from different noise sources inside and outside wards. It can be deduced that noise pollution either directly or indirectly affects, in a simultaneous manner, the subjective perception of noise, emotion, physiology and experience of noise inside and outside the wards of the medical care staff and the patients and visitors. ACKNOWLEDGEMENTS The authors would like to thank the undergraduate students, Yi-Jiun Chen, Jia-Ru Shiau, Shih-Jie Huang, Jung-Chu Lai and Yun-Yu Deng, in the Department of Health Business Administration of Meiho University for helping the sound level measurement and the noise questionnaire survey in this study for helping the sound level measurement and the noise questionnaire survey in this study. REFERENCES
The following images related to this document are available:Photo images[st10070t9.jpg] [st10070t8.jpg] [st10070t6.jpg] [st10070t4.jpg] [st10070t2.jpg] [st10070t1.jpg] [st10070t7.jpg] [st10070t5.jpg] [st10070t10.jpg] [st10070t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}