 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
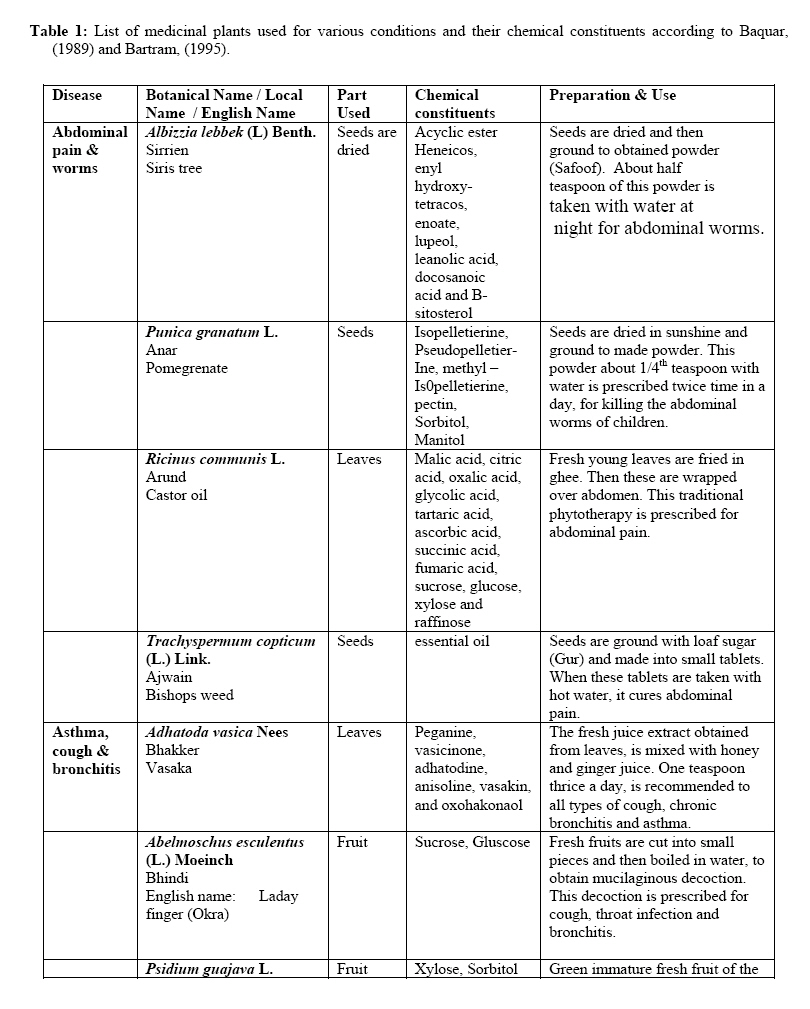
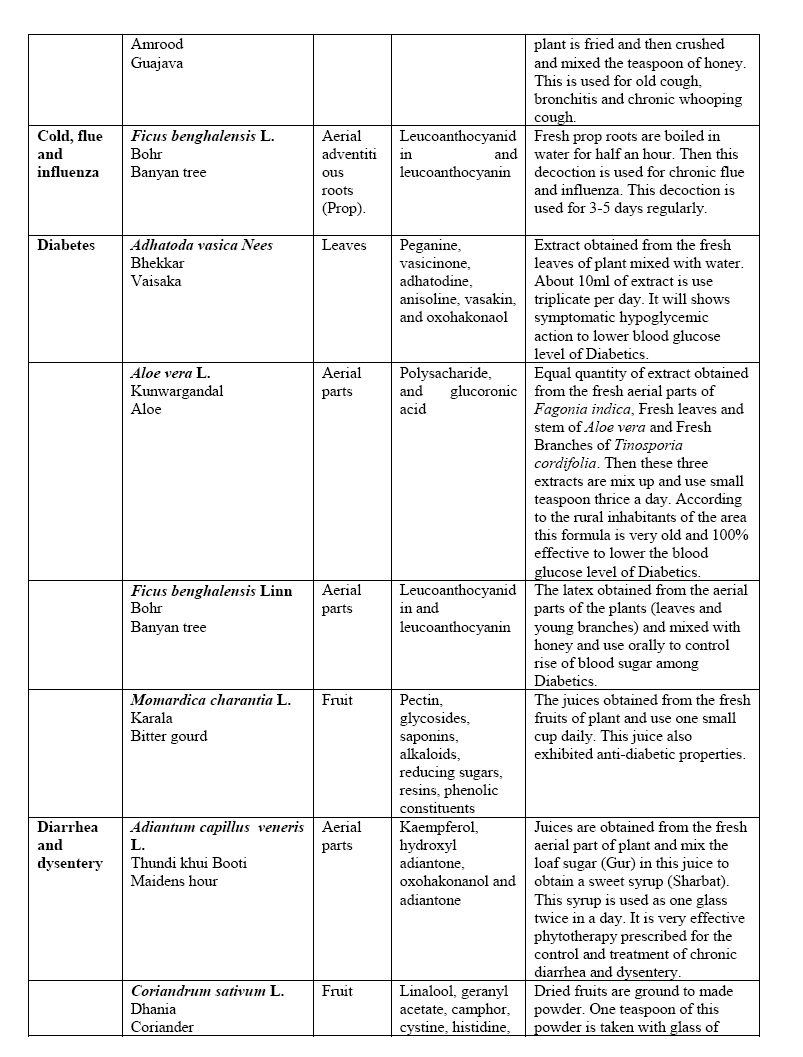
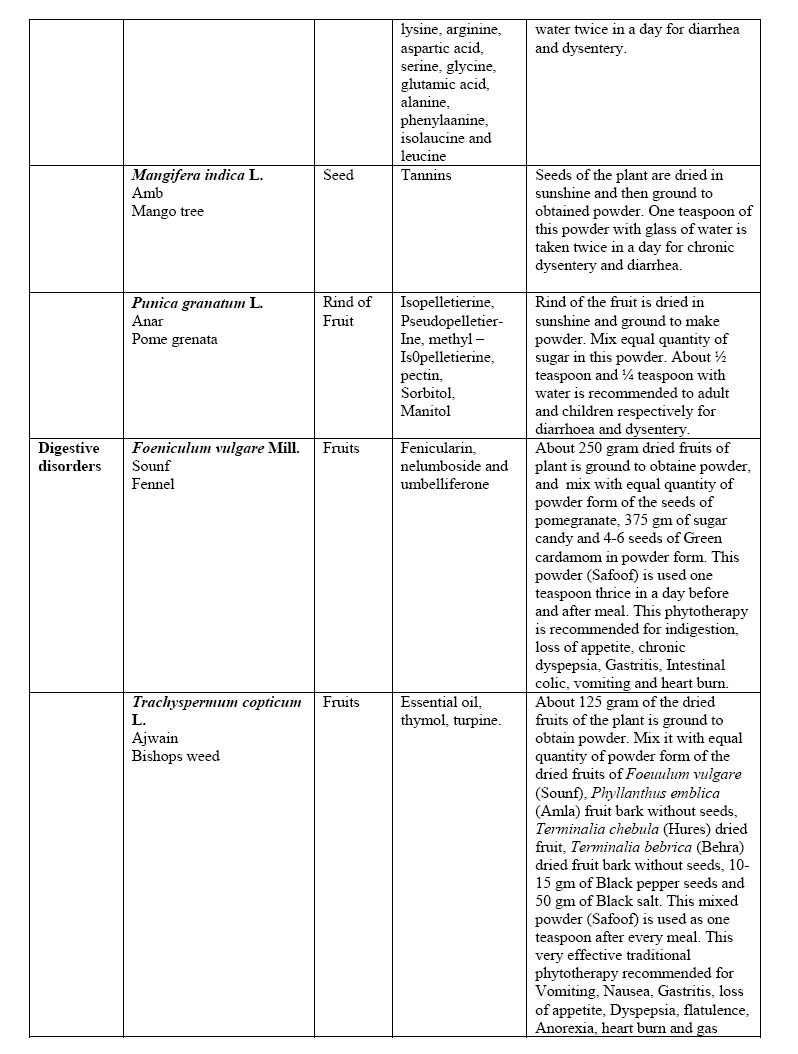
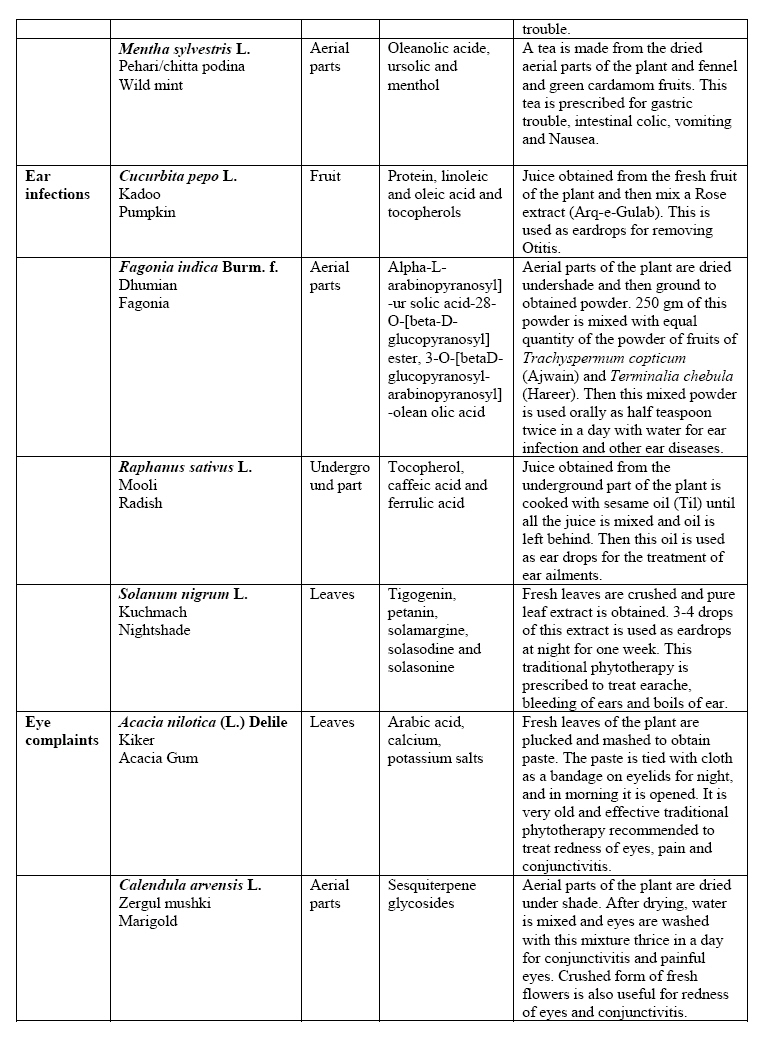
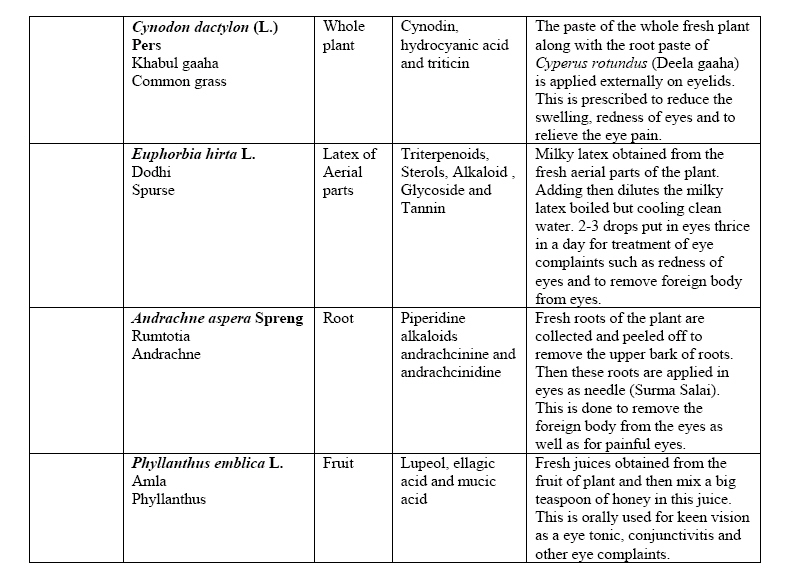
African Journal of Traditional, Complimentary and Alternative Medicines,, Vol.4, No. 1, 2007, pg. 112-120 RESEARCH PAPER TREATMENT OF COMMON AILMENTS BY PLANT-BASED REMEDIES AMONG THE PEOPLE OF DISTRICT ATTOCK (PUNJAB) OF NORTHERN PAKISTAN Mushtaq Ahmad, Mir Ajab Khan, Muhammad Zafar and Shazia Sultana Department of Biological Sciences, Quaid-I-Azam University, Islamabad-Pakistan 46000, E-Mail: mirajab@hotmail.com Code Number: tc07004 Abstract District Attock is one of the resource-based areas of medicinal plants in the north of Punjab province of Pakistan. The local people of the area have always used medicinal plants for their common ailments by traditional methods. Indigenous knowledge of local people about medicinal plants is directly linked to their culture and history. It is therefore felt worthwhile to record the indigenous knowledge about the plant-based remedies. The present communication deals with the common diseases treated by plant based remedies such as abdominal pain and worms, asthma, cough and bronchitis, cold, flu, influenza, diabetes, diarrheoa, dysentery, digestive disorders, ear infections and eye complaints. 25 species belonging to 25 genera were used for common ailments. It was found that plant based remedies were used in effective prescriptions, which are simple, inexpensive, and acceptable among the local inhabitants of the area. Key words: Ailments, medicinal plants, Attock, Pakistan Introduction District Attock is a famous historical region situated in the north of Punjab province of Pakistan. It acts as a gateway for the province N.W.F.P. of Pakistan. Due to its unique location, it has very useful resources of medicinal plants. District Attock lies between 370 and 340 North latitude, 71.45 and 730 east longitude. The river Indus bound it on North and West. In east lies district Haripur of North West frontier province and Rawalpindi district of Punjab. Southern side is occupied by district Chakwal of the Punjab. The average annual rainfall is 783 mm. The mean maximum and mean minimum temperature in January is 17.9 oC and 5.2 oC respectively. The mean maximum and mean minimum temperature in July is 42 C0 and 26.45 C0 respectively. The total area of the district is 6856.703 sq. km (Anonymous, 1998). The area has a rural culture of old traditions and the local people have their own principle and choice for a village site, house, family, dress and ornaments, weddings, childbirth, death ceremonies, cultural functions, festivals and socio-religious belief. The local ladies are more dynamic and laborious in comparison to the gents. The lack of communication with modern civilization have kept them closer to nature where they derive many of their day-to-day needs. The people of the area are very much close to natural vegetation, both in their habitat and livelihood. So, the people of the area have empirical observations of nature and by communicating with other people of their culture, they derive indigenous knowledge of the local plants. They, thus gain indigenous knowledge generation after generation from their ancestors. Plant and plant materials available from the local area are used as food fodder, medicine, veterinary medicines, timbers, households, oilseeds and also for socio-religious and other purposes. Similarly, local people in various villages of the area would gather indigenous medicinal plants throughout the year for marketing, personal and whole community use with in the area. In this way, the ethnobotanical knowledge of wild and cultivated plant use is directly linked to local culture and history. Medicinal plants are valuable natural resource and regarded as potentially safe drugs. They have been playing an important role in alleviating human sufferings by contributing herbal medicines in the primary health care systems of rural and remote areas where more than 70% of population depends on folklore and traditional systems of medicines. The reason for their popularity is due to the high cost of allopathic medicines and side effects which encouraged manufacturers of Greco-Arab and Ayurvedic systems of medicines to merge their orthodox medicine with local traditional medicines in order to spread health coverage at a reasonable prize (Shinwari and Khan, 2000). Pakistan occupies a unique position among developing countries as it has a good potential with in the variety of medicinal plants due to its varied climatic and edaphic factors, which reflect diversity and valuable medicinal plant heritage. About 6,000 flowering plants have been reported to occur in Pakistan. A very large number of drug plants are found in northern and northwestern parts of country (Ali and Qaisar, 1986). The study area has three distinct regions, Chhachh, Sarwala and Nala Tract. The vast area and varied agro-climatic conditions of this area make it possible for all types of the medicinal plants and other usefull plants to grow. Rich biodiversity of medicinal plants in this area demand extensive research. The documentation of indigenous knowledge of local people about the use of plants is often the source of ideas for developing plants species for wider use and economic benefit and there are a large number of unidentified plant species in the area which could prove useful. The local people have good knowledge of the utilization of natural resources in this area. This knowledge is going to be lost because of the interference of modern cultural changes. Continuity of this practice will result in the loss of such knowledge. Therefore, efforts were made to understand the indigenous knowledge of local people with special reference to chemical constituents and ethno-pharmacological practices for the treatment of common day ailments. The present study was designed to investigate the ethno-medicinal potential of local people. It was also considered necessary to identify the medicinal plants, chemical constituents and their ethnopharmacological uses among different groups of society, for future research in production technology, phytochemistry and production of pharmaceutical products for wider circulation. Methodology The present research work was carried out during March 2004 to February 2006 through field surveys in different remote villages of the District of Attock. The questionnaires were devised to identify the indigenous knowledge of plant-based remedies from local people. The research work was unique in that the emphasis was on both men and women and also herbal doctors (Hakims). The medicinal herb data sheet was incorporated into the research work as a means of obtaining detailed information on specific medicinal plant species used in indigenous recepies. During the survey, 150 men, 50 women and 10 local herbalists (Hakims) were interviewed from different villages in the area. Frequent field trips of the area were conducted according to the life form, flowering period and season of utilization of plant products by local people. The plant specimens were collected, dried, poisoned and identified with help of flora of Pakistan (Nasir and Ali, 1970-1995 ; Stewart, 1972) and deposited as voucher specimens in the herbarium of Quaid-i-Azam University, Islamabad. Plant-based remedies were presented with common disease& apos;s name followed by botanical name of species, local name, English name, part used, chemical constituents and preparation and use. For chemical constituents prior informed consent (PIC) was used in carrying out this work. The investigation on chemical constituents of the medicinal plants were reviewed from Baquar, (1989) and Bartram, (1995). Results The data on 10 common diseases, namely abdominal pain and worms, asthma, cough, bronchitis, cold, flue and influenza, diarrhea and dysentery, digestive disorder, ear infections and eye complaints which were analysed with the plants as presented in Table 1 a, b, c, d, e. Information on indigenous recipes were originally documented from local communities of the area and chemical constituents of the medicinal plants were given as reviewed by Baquar, (1989) and Bartram, (1995). Useful findings about indigenous medicinal plants Collection Medicinal Plants gathering is done by all members of the community while children also play an important role in the collection of medicinal plants. Gatherers are mainly low income people. Shepherds, men, women and Nomad ethnic groups, also collect medicinal plants. Different parts of the plant can be used to treat different conditions. For example, the fruit of Acacia nilotica (Kikar) has aphrodisiac action and bark of the same species have different primary action to the fruit by being strongly diuretic. Identification of the correct time for collecting plant species is crucial. Optimal timing has a direct link with the part of plant used. Processing Fresh and dried plants were both used. Processing techniques were found to be same throughout the study area. Various techniques were observed but the most popular proved to be sun drying and shade drying. According to specialists (Hakims and elderly people) of the area, shade drying is considered to be better than sun drying because during sun drying the volatile oil like contents of the plants were destroyed. The optimal method for drying herbs according to Bartram (1995) is to spread the unwashed, dust-free, organic plants out on racks in a well ventilated room away from sun lights, and excessive heat. Turning or agitation should occur daily, and the herb should not under go further preparation until the procedure has been successfully completed. Further processing for internal use included decoctions, fresh juices, infusions, syrups and cooking the herb. However, these alternative preparations do provide substantial medicinal benefits. Table 2: List of medicinal plants used for ethnopharmacological treatments
In fact, some plants are thought to have a greater efficacy when used individually for a particular ailment. For example, Tribulus terestris (Caltrops, Bhakra) roots& apos;decoction is most commonly used for kidney stone and kidney disorders. Fresh leaf juice of Adhatoda vasica (Vasaka, Bekkar) is given to reduced blood glucose level of diabetic patient. Similarly juice obtained from fresh leaves of Solanum nigrum (Night shade, Kuchmach) in 2-3 drops is used in the night for ear infection and ear bleeding. Grinding of dried and fresh herbs is also a common technique. Storage Dried herbs should be stored in an air-tight container in a cool, dry, dark environment to prevent the loss of volatile oils and possible spoilage. Storage conditions includes the use of cloth bags (not air-tight), clear glass bottles and plastic bags. On some occasions the plants were stored in direct sunlight, but were usually kept either inside a dark room or outside on the verandah. Further preparation of dried herbs were rarely stored. These preparations (decoctions, infusion), can only be stored for a few days before their quality deteriorates. Cultivation Practices of Medicinal plants: Cultivation of medicinal plants is mostly done by the local people of Chhachh region (About 53%). The farmers cultivate certain medicinal plants along these crops, fodders and vegetables for their own domestic used and small scale for local markets in the Chhachh region. These cultivated medicinal plants were not produced in large quantities because local farmers have little or no marketing strategy and ability. In Sarwala and Nala tract of Tehsil Attock, the cultivation of medicinal plants is undertaken but to lesser degree (30% & 17% respectively). The commonest cultivated medicinal plants for treatment of various ailments are, Abelmoschus esculentus (Bhindi), Aloe vera (KunwarGandel), Foeniculum vulgare (Sonf), Solanum nigrum (Kuchmach), Mentha sylvestris (Pehari Podina), Trachyspermum copticum (Ajwain) and Raphanus sativus (Mooli). It was also observed that the most households grow medicinal plants for themselves, relatives and neighbours and not for commercial purposes. An understanding of the market potential for medicinal plants could provide rural farmers with the incentive for cultivation of high demand species. Discussion Life and diseases go together, where there is a life, diseases are bound to exist. Dependence and sustainability of men, women, children and animal life were revolving to exist. Traditional uses of natural plants remedies provide potential indicators for biological activities. In the last few decades, there is a resurgence of public interest in medicinal plants and their role in primary health care (Haq, 1983). Alternative medicine using herbal mixtures is becoming more popular as these are believed to be safer and natural. However, there still exists an immense gap between the local traditional knowledge and modern medical sciences. This has resulted in the development of research priorities on plant used in traditional medicine to provide important sufficient information for commercialization. According to WHO, about three quarters of the world population relies upon traditional medicines (TM) mainly herbs for their healthcare. TM is now increasingly becoming essential part of the medicinal curriculum at a global level and it is anticipated that the modern physicians who are also skilled with some alternate methods of treatment are likely to be more successful physician in the years to come (Shinwari and Khan, 1999). Thus there is a huge potential of medicinal plants in health care of not only in remote areas like Attock of developing countries but also in the industrialized world and the acceptance of botanicals in modern medicines is likely to increase in future. In this study data on 25 medicinal plant species belonging to 18 families were presented. Main emphasis was on the traditional plant based remedies which are used through out the area and the correlation between their actions and active chemical constituents which were reviewed by Bradly (1992) and Baquar (1989). It was found that the people of the area had and still have rich heritage of indigenous knowledge related to medicinal plants. In developing country like Pakistan, the benefits of modern medicine and health care is a luxury because only a small percentage of the population have access to it. Every year a considerable amount of scarse foreign exchange is used in the importation of modern drugs. The utilization of indigenous plant-based drug resources will increase the importance of the local industry on the one hand and will minimize the expenditure incurred on the purchase of foreign drugs on the other. Hence there is a need for the inclusion of herbal medicines at primary health care level, since their long standing use as plant drugs without toxic effects would reasonably guarantee their medical efficacy and safety. It is concluded that collaborative work amongst the taxonomists, ethnobotanists, ethnopharmacologists and phytochemists is essential for the productive evaluation of these resources. References
The following images related to this document are available:Photo images[tc07004t1a.jpg] [tc07004t1b.jpg] [tc07004t2.jpg] [tc07004t1e.jpg] [tc07004t1d.jpg] [tc07004t1c.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}