 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
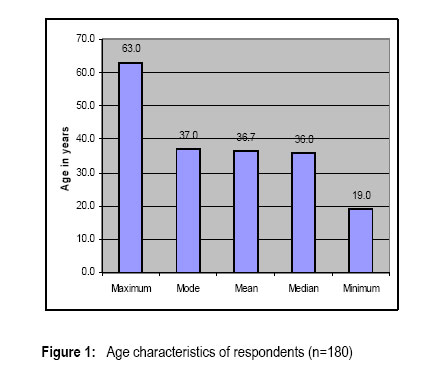
African Journal of Traditional, Complimentary and Alternative Medicines, Vol.4, No. 3, 2007, pg. 273-278 Research Paper SELF-REPORTED USE OF TRADITIONAL, COMPLEMENTARY AND OVER-THE-COUNTER MEDICINES BY HIV-INFECTED PATIENTS ON ANTIRETROVIRAL THERAPY IN PRETORIA, SOUTH AFRICA Malangu, N. National School of Public Health, University of Limpopo (Medunsa Campus), Box 215, MEDUNSA 0204, Pretoria, South Africa. Telephone: (27) 12 521 4613; Fax: (27) 12 546 5101 . Code Number: tc07048 Abstract Current management of HIV involves the use of conventional prescription medicines, called ‘antiretroviral drugs’ (ARV), over-the-counter (OTC), complementary and alternative medicines (CAM), as well as African traditional medicine (ATM). The aim of this study was to determine the prevalence of use of traditional, complementary and over-the-counter medicines. A cross-sectional survey of HIV-infected patients who started ART between July 2004 and August 2005 at Dr George Mukhari Hospital (Pretoria), who consented to be interviewed, was conducted. Using a pre-tested structured questionnaire, data were collected by two trained interviewers on sociodemographic characteristics, and on non-prescribed medicines used of three sources: African traditional medicine (ATM), complementary and alternative medicine (CAM), and over-the-counter (OTC) medicines. The 180 patients who consented to be interviewed had a mean age of 36.7 (±8.1) years old; 68.8% were female, 86.7% unemployed, 73.9% with high school level of education, 77.8% single. Some 8.9% of respondents used at least one non-prescribed medicine. In descending order, 4.4% of respondents used ATM, 3.3% CAM, and 1.7% OTC medicines. The ATM products used included unspecified traditional mixtures, and those made of the African potato (Hypoxis hemerocallidea), and coconut (Cocos nucifera); OTC products used were paracetamol and sennosides (Senokot®) tablets as well as a soap containing triclosan 1.5%; CAM products used were “sex booster” capsules of unknown composition, mercury-containing soaps (Mekako®), and the Zion Church of Christ special tea, a mixture of Rooibos tea (Aspalathus linearis) plus sunflower oil (Helianthus annuus) and prayed for. In conclusion, only 8.9% of HIV-infected patients on ART in this study used a limited range of over-the-counter products as well as those from traditional, complementary and alternative medicine practices. Key words: Traditional, complementary, medicines, HIV Introduction Current management of HIV involves the use of conventional prescription medicines, called ‘antiretroviral drugs’ (ARV), over-the-counter (OTC), complementary and alternative medicines (CAM), as well as medicines from traditional practices such as the African traditional medicine (ATM). The complexity of HIV treatment is further compounded in some instances by the use and/or abuse of recreational drugs, vitamins, and mineral supplements that HIV-infected patients may procure themselves for self-care; as well as the use of medicines prescribed for treating opportunistic infections and other co-morbidities that may affect people infected with HIV. The multiplicity of medicines used lead not only to potentially severe side effects, but also to clinically significant interactions with ARVs and other medicines. These side effects and interactions affect patients with regard to their adherence to treatment, and quality of life, which ultimately affect the effectiveness of the antiretroviral therapy (ART). It is, therefore, important to establish the extent of use of non-prescribed medicines namely, over-the-counter, traditional and complementary products. This was the aim of this study. While the purpose of the antiretroviral treatment is to suppress viral load and maintain it at undetectable level as long as possible because of the associated clinical benefits (O’Brien et al., 1996), it is reported that the purposes for which HIV-infected patients use CAM and possibly ATM medicines include the need to combat weight loss, nausea, and diarrhea, to fight HIV or boost immunity, and to relieve stress (Eisenberg et al., 1998; Fairfield et al., 1998). Hence, the use of CAM therapies is reportedly more prevalent in patients infected with HIV. Duggan et al. (2001) surveyed 191 patients seeking care for HIV infection. Approximately 67% of the surveyed group reported using CAM therapies currently or in the past. In the group using CAM, 50% indicated use of herbal medicines. About 7% of respondents stated that they used CAM alone to control HIV. In another study that involved 1675 HIV-positive participants, about 63% of them used both CAM and ART. Participants in the study reported using approximately 1200 substances such as antioxidants, vitamins, and herbs. Garlic (Allium sativum ) was the most common herbal product used (Standish et al., 2001). However, it is known that some clinicians may not be aware of the fact that their patients are actually using CAM or ATM medicines. In one study, 64% of patients stated that their treating doctors were aware of their use of alternative medicine, although only a few of the clinicians had advised their patients to discontinue the use of these therapies (Miller, 1998). Patients on ART used also African traditional medicines. It is reported that about 75% of HIV-infected patients take some remedies from complementary or African traditional medicine in South Africa (WHO, 2003). A clinical evaluation of an unspecified traditional herbal medication by Tshibangu et al. (2004) showed interesting results. Within eight months of therapy, there was a significant health improvement with regard to physical appearance (80% of patients), disappearance of urogenital lesions (100%), weight gain (80%), as well as a significant reduction in viral load and a significant increase in CD4-cell count. Adewunmi and Ojewole (2005) mentioned that similar findings have been reported elsewhere. However, herbal medicines can cause psychiatric and neurological adverse effects due to improper use, intrinsic toxicity of ingredients, contamination and adulteration of preparations, interactions with conventional drugs (Ernst, 2000). There is still a need for more data in this area; hence the need for this studies that highlights the prevalence of use of over-the-counter, complementary and traditional medicines used by HIV-infected patients. Materials and Methods This investigation was designed as a cross-sectional study. This design was used because it offers a cost-effective way to gather information from many people in a relatively short period and provides a high degree of standardisation coupled with reliability that is useful for the comparability of data (Katzenellenbogen et al., 1997). Using a pre-tested structured questionnaire, two qualified HIV/AIDS counselors from Ga-Rankuwa Township conducted interviews with HIV-infected patients who started ART between July 2004 and August 2005 at Dr George Mukhari Hospital, in Pretoria. The two, a 34-year old man, and a 47-year old woman, were trained by the investigator in the filing of the questionnaire before and during the pilot study. They were all able to speak at least 3 languages including English and Afrikaans. The emphasis of their training was on the need of creating a more comfortable and trusting environment in which patients could honestly report non-prescribed medicines used by them. Moreover, detailed and embedded instructions were provided on what they ought to say to respondents from the structured questionnaire used for the purpose. Data were collected on age, gender, employment and marital status, formal education level, names and types of non-prescribed medicines used (OTC, ATM and CAM). In order to comply with internationally accepted ethical standards and ensure that participants were protected from coercion, undue physical or psychological harm, the proposal for this study was submitted, and approved by the Research and Publications, and Ethics Committee of the Faculty of Medicine of the University of Limpopo-Medunsa Campus. In order to adhere to the principle of autonomy, interviewers explained the content of the informed consent form in the language of choice of participants. Those who consented to participate signed individually a consent form. Interviewers signed also as witnesses on the consent forms. The content of the consent form explained to the respondents was included in the questionnaire as part of the instructions to interviewers. Specifically the purpose of the study as well as its potential risks and benefits to the participants were stated. Results and Discussion The sociodemographic characteristic of respondents is summarised in Figure 1 and Table 1. Among the 180 patients who consented to be interviewed, their mean age was 36.7 (±8.1) years. The majority were female, single, unemployed, and had achieved a high school level of education. This demographic distribution of respondents is consistent with the epidemiological data of HIV-positive patients in South Africa in that, women and patients older than 30 years were the majority. Connolly et al. (2004) reported that the prevalence of HIV was highest in females in the age group from 20 to 39 years old. The finding that 31.1% of male versus 68.9% of female respondents were on ART suggests that access to ART at this clinic reflects the gender distribution of the infection contrary to the view held by Venter (2005) who stated that access to ART, in South Africa, is disproportionately in favour of women. With regard to self-medication, the use of non-prescribed medicines by patients, primarily on their own initiative and under their own responsibility, has the potential to help prevent and treat minor ailments that may not require medical consultation. Nonetheless, it is reported from studies in the USA that, the most common reasons for using CAM is pain, and that 53% of HIV-infected people use CAM (Tsao et al., 2005; Bausell et al., 2003). In this study, although the purpose of each product used was not assessed, 8.9% of patients used ATM, CAM and OTC medicines. In descending order, 4.4% of respondents used ATM, 3.3% CAM and 1.7% OTC medicines. With regard to ATM, our findings are similar to reports by Shisana et al. (2005) who reported a corresponding figure of 1.1%. This is still far below the figure of 75% quoted elsewhere (WHO, 2003), and reported in other groups of HIV-infected people. With regard to CAM, the figure reported in this study is low as compared with results from a study in Thailand, where 95% and 72% of HIV-infected patients interviewed respectively used CAM, and visited a CAM practitioner (Wiwanitkit, 2003). Both cultural and economic reasons could explain the difference, since in South Africa, it is the ATM practice that is more commonplace. It is reported that HIV-infected patients use herbal and medicinal plants extensively, some of which their active agents have been determined, and have been successfully tested in clinical studies (Vermani and Garg, 2002). In this study, the composition of most ATM mixtures was unspecified. This implies that more studies are needed in this regard in order to identify their active ingredients, and assess the usefulness of the ATM mixtures used by HIV-infected patients (Adewunmi and Ojewole, 2005). The ATM products used included unspecified traditional mixtures and those made of the African potato (Hypoxis hemerocallidea), and coconut (Cocos nucifera); OTC products used were paracetamol and sennosides (Senokot®) tablets as well as a soap containing triclosan 1.5% (Tetmosol®); CAM products used were "sex booster" capsules of unknown composition, mercury-containing soaps (Mekako®), and the Zion Church of Christ (ZCC) special tea. This special tea is composed of Rooibos tea (Aspalathus linearis) plus sunflower oil (Helianthus annuus) and prayed for.
Table 1: Sociodemographic characteristics of respondents (n=180)
The use of soaps containing mercury raises some concerns. The hazards associated with mercury outweigh any therapeutic benefit, and its clinical use has been abandoned (Sweetman, 2006). While ointments containing ammoniated mercury have been used for some skin disorders, nowadays the soaps are commonly abused for skin lightening (Malangu, 2004; Adebajo, 2002; Del Guidice and Yves, 2002). On the contrary, the use of the soap containing triclosan may be useful since it is an antiseptic (Sweetman, 2006), although it was not possible to establish whether this was an appropriate or inappropriate use. These above findings suggest that providers of health care to HIV-infected patients need to communicate with their patients so that they can be made aware of non-prescribed medicines they take. This information could be used by providers to intervene by educating patients on potential dangers, and by encouraging them to stop the misuse of non-prescribed products depending on their circumstances. Conclusion Only 8.9% of HIV-infected patients on ART in this study used a limited range of over-the-counter products as well as those from traditional, complementary and alternative medicine practices. References
© Copyright 2007 -African Journal of Traditional, Complementary and Alternative Medicines ; The following images related to this document are available:Photo images[tc07048t1.jpg] [tc07048f1.jpg] |
| |||||||||

{kind=link}