 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Traditional, Complimentary and Alternative Medicines, Vol. 5, No. 2, 2008, pg. 180-186 Research PaperProtective Effect of Garcinia Kola (Kolaviron) Extract on Predis-Position of Rats to Cardiovascular Diseases Following Separate Administration of Amodiaquine and Artesunate E.O. Ajani*; P.D. Shallie**, B.O. Adegbesan*, B. A. Salau* and M Adesanya* *Department of Biochemistry, Faculty of Basic Medical
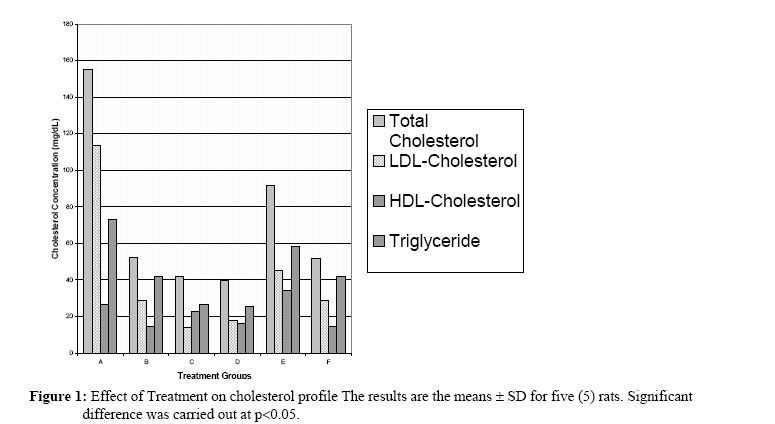
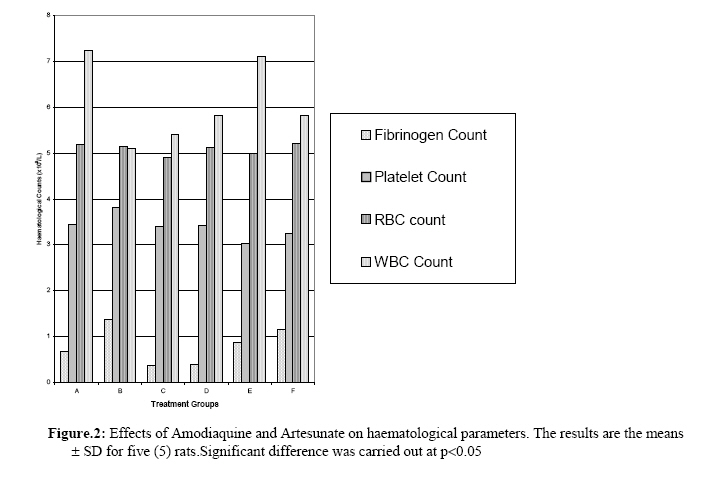
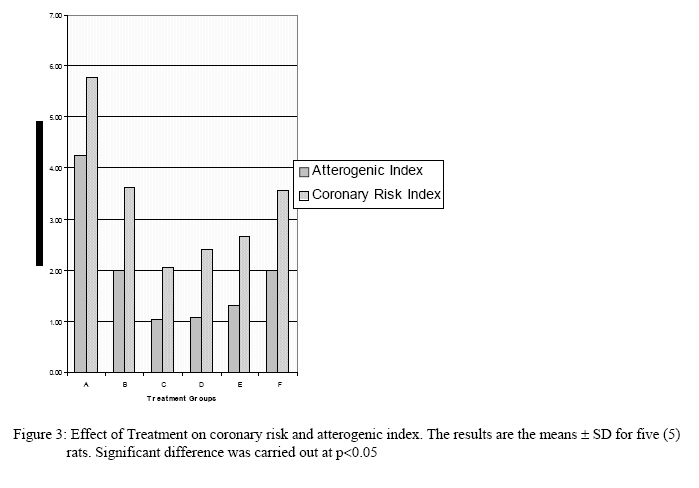
Sciences, Olabisi Onabanjo Code Number: tc08025 Abstract This study was carried out to investigate the cardiovascular effect of administration of antimalarial drugs amodiaquine and artesunate and the efficacy of Garcinia kola extract (kolaviron) in protecting against such possible effect. Thirty (30) adult male albino rats divided into six (6) groups were used in this study. Groups D, E and F were treated with 100 mg/Kg b. w of the extract twice daily for the first one week and 200 mg/Kg b. w. /day for the subsequent three (3) weeks. Amodiaquine (10mg/Kg. b. w. /day) was administered orally for four (4) days into rats in groups A and E while rats in groups B and F were treated with artesunate (5mg/Kg b. w. /day) for four (4) days. Group C rats (normal control) were treated with normal saline. All the rats were sacrificed after four (4) weeks treatment period. Blood was withdrawn by cardiac puncture while the liver, kidney, stomach and heart were removed, cleansed and weigh. Total cholesterol, LDL- cholesterol, HDL- cholesterol and triglycerides were measured in the serum, while total fibrinogen, platelet count, red blood cell and white blood cell count were measured in the whole blood. The artherogenic and coronary risk index were also determined. Results indicate that both amodiaquine and artesunate predispose to cardiovascular disease, however the effect was more pronounced with artesunate than amodiaquine. The result also suggests that both drugs could increase the risk of coronary and artherogenic diseases and that Garcinia kola do not prevent the cardiotoxicity and coronary risk effect. Key Words: Garcinia kola, Cardiovascular disease risk factor, amodiaquine and artesunate Introduction Amodiaquine (Camoquine, Parke – Davis) is a 4-aminoquinoline derivative similar to chloroquine and has been widely used both in the prophylaxis and treatment of malaria (Pero and Taylor, 2002; WHO, 1990). Following serious toxicity associated with its use as prophylaxis, it was withdrawn by the World Health Organization (WHO) from the list of drugs for the treatment of malaria during 1990 – 1996 but later re- instated in 1996 (Pero and Taylor, 2002). Aggranulocytosis and liver damage have repeatedly been reported as adverse reactions (ADR’s) to amodiaquine (WHO, 1990). The 19th expert committee on malarial reported that amodiaquine could be used for treatment if the risk of infection out weigh the potential for ADR’s but still did not recommend amodiaquine as first line treatment (WHO, 1993). Today, the drug is still in use in the tropics for malaria therapy (Koech et al., 1989) In recent years, increasing attention has been given to therapies combining antimalarial drugs with different mode of actions. Amodiaquine has been tested in clinical trials in combination with artesunate or sulfadoxine/pyrimethemine with very encouraging results (WHO, 2001). Artesunate is a water soluble hemisuccinate derivative of dihydro – artemisinin. Artemisinin is a sesquiterpene lactone isolated from Artemisia annua, an herb that has traditionally been used in china for the treatment of malaria (Greenberg, 2004). Amodiaquine in combination with artesunate is now one option that is recommended by the WHO for use in malarial control programmes. Artesunate and other related artemisinin derivatives have been widely used with no reports of any serious adverse reactions. Neurotoxicity has however been observed in animal studies but not in human (http://www.malaria_ipca.com). Cardiovascular disease (CVD) has been described as the major cause of morbidity and mortality in adult human being (John et al., 1999). Epidemiological studies have shown that elevated concentrations of serum total cholesterol and LDL-cholesterol, triglycerides, fibrinogen and platelet count are independent risk factors for CVD (John et al., 1999; Mark et al., 1999). Garcina kola is a medium sized forest tree found throughout West and Central Africa. The seeds are eating as refreshing past time in Nigeria and are known to contain high content of biflavonoid compound. The toxicity is very low, the oral 50% lethal dose being above 5000 mg/Kg b. w. (Nwankwo et al, 2000). The seeds known as “bitter kola” or “false kola” are believed to posses’ aphrodisiac properties and are used for the treatment of catarrh and abdominal colicky pain (Adaramoye et al., 2005). Considerable experimental evidence has been adduced in support of the antihepatotoxic efficacy of kolaviron in animals against such hepatotoxicants as paracetamol (Iwu, 1986), carbon tetrachloride, thioacetamide, galactosamine, phallodine, and ethanol (Farombi, 2000; Adaramoye et al, 2005). In a previous study, we also observed the hepatoprotective effect of the extract in amodiaquine induced gastric ulceration (Ajani et. al., Unpublished data). There has been increasing report of ischaemic heart disease (Khaw and Barret, 1987). This increase may be attributed to an increase in the prevalence of known cardiovascular risk factor including drugs and local herbs. The aim of the present study is to investigate the risk of developing cardiovascular disease risk factors with administration of amodiaquine and artesunate and also examine the efficacy of kolaviron in reversing such possible symptoms of cardiotoxicity Materials and methods Plant materials Garcina kola seeds (Guttiferae) (voucher No. OPZH 1034g) were obtained locally in Sagamu market and certified by the Plant Science Department, Olabisi Onabanjo University, Ago – Iwoye, Nigeria. The peeled seeds (7.5kg) were then sliced, pulverized with an electric blender and dried at 400C in a Gallenkamp drying oven Preparation of Garcina kola extract The method of Iwu et al (1990) was used in the extraction of Garcina kola seed. The powdered seeds were extracted with light petroleum ether in a Soxhlet for 24hours. The defatted dried mare was repacked and extracted with acetone. The extract was concentrated and diluted twice its volume with water and extracted with ethyl acetate (6 X 300ml). The concentrated ethyl acetate fraction gave a yellow solid known as kolaviron. Appropriate dose dilutions were made by suspending the extract in 0.9% NaCl solution while normal saline was administered into the control group. Treatment and care of Animals Thirty (30) healthy male albino rats weighing between 150 – 220g were used in the study. They were all obtained from the animal house, Physiology Department, University of Ibadan, Nigeria and were acclimatized for a week. The rats were randomly distributed into six (6) groups. Amodiaquine {Sigma, St. Louis, USA} (10 mg/kg b. w. / day) was administered orally into group A for 4days. Group B was treated with artesunate {Sigma, St. Louis, USA} (5 mg/kg b. w. /day) orally for 4days. Rats in group C were treated with normal saline while those in group D were treated with Garcina kola extract (200 mg/kg b. w. /once daily) for 4weeks. Rats in group E and F were treated with Garcina kola extract (100 mg/kg b. w.) twice daily for the first one (1) week and 200 mg/kg b. w. once daily for the next 3weeks. In the second week of treatment with Garcina kola, amodiaquine (10 mg/kg b. w.) and artesunate (5 mg/kg b. w) was administered orally into group E and F rats (respectively) continuously for 4days. All administrations were carried out with oral intubator. Animal care and protocols were in accordance with the guidelines of the Institutional Animal Ethics Committee (Committee on care and use of Laboratory animals, 1985). Animals were housed in individual cages in a temperature and humidity controlled room having a 12hr light and dark cycle. Feed and clean drinking water were supply ad libitum. All animals were sacrificed after 4weeks. Blood was withdrawn by cardiac puncture into a heparinized bottle. The blood was centrifuged at 3000g for 10min and the plasma was carefully extracted by pastures pipette. The plasma was stored at 30 to 400C until analyzed. The livers, kidney, spleen stomach and heart were quickly removed cleaned, dried and weighed. Determination Of Serum Cholesterol, Lipoproteins And Triglyceride Serum total cholesterol was determined using the method of Liebermann (1958). HDL- cholesterol was determined by the precipitation, enzymatic, colorimetric method of Sigma (1991) Triglyceride was determined by colorimetric end point of Sigma (1991). Serum LDL- Lipoprotein was determined by difference. Platelet was counted microscopically while plasma fibrinogen was estimated based on clotting by thrombin physicochemical transformation. Atherogenic index was calculated using the formula of Abott et al, (1988) and coronary risk index was obtained by the method of Alladi et al, (1989) Statistics All results were analyzed by two – tailed student’s t – test. P values of less then 0.05 were considered statistically significant. Results Following administration of artesunate, the relative weight of the heart, the kidney and the spleen were noticed to increase. These increases were however reversed with Garcinia kola pretreatment. Amodiaquine administration increased the liver weight where as the heart, spleen and kidney were not significantly altered (Table 1). Garcinia kola pretreatment also reduced the liver weight of the amodiaquine treated rat to pretreatment level. Figure 1 is the result of the effect of administration of the drugs on serum cholesterol profile. Amodiaquine administration resulted in a significant increase in total cholesterol, LDL cholesterol, and triglyceride level. HDL cholesterol was however not significantly altered. With Garcinia kola pretreatment however, the values obtained for total cholesterol and LDL cholesterol were lowered, though the values obtained were still higher than the control values, where as the HDL cholesterol was not altered significantly. When Garcinia kola was administered alone, no change was observed in these parameters. Similarly, artesunate administration significantly increased serum total cholesterol, LDL- cholesterol and triglyceride values, but lowered HDL- cholesterol. When pretreated with Garcinia kola, artesunate administered rats did not show a significant alteration in these parameters from the values observed with sole administration of artesunate. Result for the hematological parameters is presented in Figure 2. With artesunate administration, significant increases in fibrinogen and platelet count were observed, whereas the RBC and WBC count were not significantly affected. Pretreatment with Garcinia kola however lowered the platelet count and the value of 3.24±0.12x103/µL obtained was not different from the control value (3.40±0.16 x103/µL). This treatment however does not reduce the fibrinogen count from the values obtained with artesunate alone. Neither administration of amodiaquine nor pretreatment with Garcinia kola significantly altered the RBC count. Amodiaquine administration however, significantly increased fibrinogen and WBC count. The value of 7.24 ±0.04x103/µL observed for the WBC count was however still within the normal range for rat (5.5-11x10 3 /µL) The increase in fibrinogen and WBC count with amodiaquine was not reversed with Garcinia kola pretreatment, however the platelet count was reduced to the control value. Sole administration of Garcinia kola does not significantly alter any of these parameters. Figure 3 illustrates the atherogenic (AI) and coronary risk index (CRI). Both parameters were raised following administration of amodiaquine and artesunate. Garcinia kola treatment had no significant influence on the AI and CRI. Pretreatment with Garcinia kola did not alter the AI and CRI in the artesunate treated rats, as the value obtained was not different from the control values. The values for these parameters though still higher than the control values in the rats treated with Garcinia kola extract prior to amodiaquine administration, the values were however lowered compared with the values obtained when rats were administered with amodiaquine without prior treatment with Garcinia kola. Discussion Several Authors have reported on the hepatotoxicity effect of amodiaquine administration (Pero and Taylor, 2002; WHO, 1990), the present study also provide evidence in support of this and further report on the cardiotoxicity effect of administration of artesunate. The increases in the relative liver weight of amodiaquine treated rat and relative heart weight of the artesunate treated rats observed in this study may be as a consequence of fat accumulation and may predispose the subject to arteriosclerosis. John et al. (1999) reported that hypertrophy of the chronically loaded heart not accompanied by a new coronary capillary formation may lead to insufficient oxygen delivery to the cardiac muscle. Hypertrophy can be caused by physiologic or pathologic condition and is caused by increased functional demand, which in the heart is usually chronic thymodynamic overload. With continual enlargement, the heart will reach a stage when it will no longer be able to compensate for the increased burden and cardiac failure will ensures (Cotran et al., 1999). Data obtained for the lipid profile and haematological parameters further support this observation. Hyperlipidemia has been noted as an important Table 1:Effect Of Treatment On Final Organ Weight
Note: The results are the means ± SD for five (5) rats.Significant difference was carried out at
p<0.05 metabolic risk factor for Ischaemic heart disease and ischemic cerebrovascular accident. Literature has shown that there is a positive correlation between the risk of developing ischemic heart disease and raised plasma cholesterol and LDL cholesterol concentrations and a negative one with plasma HDL cholesterol. Lowering plasma total cholesterol and LDL cholesterol concentrations reduces the risk of cardiovascular disease (Michael et al., 1998; Eun et al., 2002). The increases in serum total cholesterol, LDL cholesterol and triglyceride level with a corresponding reduction in HDL cholesterol value with artesunate administration observed in this study indicate that treatment with artesunate predisposes to cardiovascular disease. The cardiovascular disease risk with this drug is reported here to be higher than that with administration of amodiaquine in that with amodiaquine, HDL cholesterol was not reduced which was the case with artesunate administration. It is important to note that pretreatment with Garcinia kola does not ameliorate this observed effect. Hence, it could be emphasize here that though Garcinia kola have been widely reputed to be hepatoprotective, the extract may not be effective against cardiovascular disease risk. Serum fibrinogen is a component of the blood that plays a central role in clotting process (Cushma et al., 1996). Recent results have shown that the level of fibrinogen and platelet count is independent cardiovascular factor (Mark et al., 1999; Passmore and Eastword, 1986). Higher level of this parameter has been suggested may predispose the affected individual to develop clots in their arteries and platelet aggregation as increase plasma viscosity, thereby increasing the risk of a heart attack or stroke (Cushma et al., 1996). Artesunate administration is reported here to increase both fibrinogen and platelet count providing evidence for cardiovascular toxicity. This effect is however mild with amodiaquine administration. The study also suggests that this cardio- toxicity effect is not reversed with Garcinia kola pretreatment. Raised WBC count is seen in acute infections, metabolic disorders and drug use. Since the observed WBC values reported here, both with amodiaquine, artesunate administration and with garcinia kola pretreatment are still within normal range, the drugs may not contribute to predisposition to infection. The increased atherogenic and coronary risk index observed with administration of amodiaquine and artesunate could be attributable to increased LDL- cholesterol and total cholesterol values. This also could suggest that both drugs when administered for prophylactic purposes may predispose to coronary disorders such as hypertension. Occlusion of a coronary artery by lipid deposit has been reported to cause several local oxygen starvations and ultimately the degeneration of a localized portion of the heart muscle (Ernst, 1991). Garcina kola is also reported here not to be effective in reversing the artherogenic and coronary risk index in artesunate administered rat. Data obtained however suggest that it may reduce the risk in amodiaquine treated rats. We opined that the efficacy of the extract in amodiaquine treated rats may be due to the effect of interaction between metabolites of amodiaquine and kolaviron and that such interaction may not occurred with metabolite of artesunate. Conclusion Our study indicates that administration of amodiaquine and artesunate predisposes to cardiovascular disease. This effect is however more pronounced with artesunate than with amodiaquine. The study also reports that both amodiaquine and artesunate when administered for prophylactic purposes may predispose to artherogenic and coronary diseases and that Garcinia kola, though reputed to be heopatoprotective, is not effective against cardiovascular disease. References
© Copyright 2008 - African. Journal. Traditional, Complementary and Alternative Medicines The following images related to this document are available:Photo images[tc08025f3.jpg] [tc08025f2.jpg] [tc08025f1.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}
{kind=link}