 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
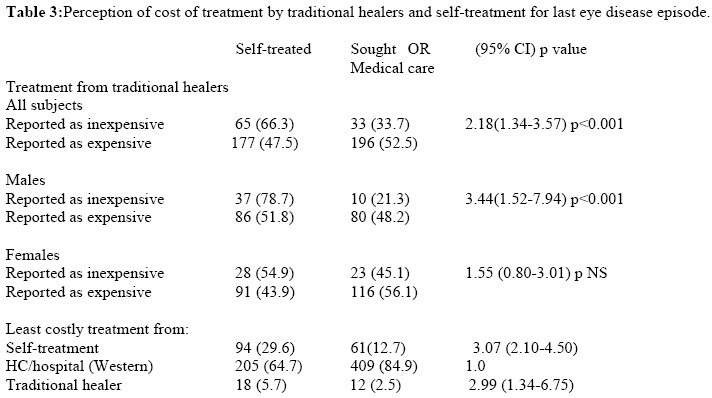
African Journal of Traditional, Complimentary and Alternative Medicines, Vol. 6, No. 1, 2009, pp. 23-29 Self treatment of eye diseases in Malawi Thomas Bisika 1-2 , Paul Courtright 3-4, Robert Geneau 3 ,Anthony Kasote 2,Lucy Chimombo 2and Moses Chirambo 5 1 University of Pretoria, School of Health Systems and Public Health, Code Number: tc09004 Abstract Self-treatment for eye diseases is very common in most developing countries yet there has been little investigation of such attitudes and practices. In many settings, people do not proceed beyond self-treatment and do not receive care from either traditional healers or Western eye care providers. Visual impairment and blindness can be the result. We conducted population-based survey of use of eye care services and self-treatment in two districts of Malawi. Adults were administered a detailed interview regarding their use of eye care services (Western and traditional as well as self-treatment) and their knowledge and use of traditional eye medicines. Self-treatment was defined as use of either Western or traditional medicines by the individual for their most recent eye condition. Only eye conditions that were considered severe by the study subjects were correlated with treatment options. Interviews were carried out among 800 adults in the study areas. Self-treatment was reported for the last episode of eye disease by 39.8% of the study population. Factors associated with self-treatment included sex, religion and socioeconomic status. Even though 76.8% of the respondents reported treatment from the health center or hospital to be the least expensive option, many opted for self-treatment first. Among those opting for self-treatment 72% used traditional eye medicines. Even among cases that individuals considered to be quite severe (these included cataract, trachoma and conjunctivitis), self-treatment was the option of choice in 22.2% of cases. Key words: eye diseases, Malawi, self-treatment, traditional eye medicine, health service utilization Introduction Global blindness increased from 28 million to 45 million in the two decades between 1975 and 1995. (Johnson and Foster, 2003) Current projections suggest that 76 million people will be blind by 2020 unless specific activities are undertaken to halt the trend (Frick and Foster, 2003). This problem is most pronounced in developing countries due to increasing life expectancy and population growth. Malawi has been the focus of considerable long-term programme and research activities on blindness (Chirambo et al., 1986). The Lower Shire Valley (Chikwawa and Nsanje districts) blindness survey of 1983 demonstrated that both trachoma and vitamin A deficiency were serious public health problems (Tielsch, 1986; Tielsch, 1988). Blindness (defined as <3/60 in the better eye) was recognized in 1% of the population over 7 years of age (Chirambo et al., 1986). These findings served as the baseline for vitamin A, trachoma, and cataract programmes in the Lower Shire Valley as well as elsewhere in Malawi. Recent research has shown a reduction in the prevalence of trachoma (Hoeschmann et al., 2001). Nevertheless, while there has been a reduction in the prevalence of the blindness in all adult age groups, the increasing size of these age groups (particularly, the most elderly) has led to a 24% increase in the number of blind people. (Courtright et al.,, 2003) In Malawi, as elsewhere in Africa, traditional healers commonly treat eye diseases. There are an estimated 135 eye care interactions between healers and residents for every interaction between biomedical eye care personnel and residents (Courtright, 1995). Research among patients presenting to district hospitals with corneal ulcers has found self treatment to be quite common (Courtright et al., 1996). While it has often been the practice of health care providers to blame traditional healers for much of the damage due to the use of traditional eye medicines, it appeared from our previous work that instillation of traditional eye medicines by patients themselves may account for much of the unintended consequences. Self treatment for eye diseases is common in many countries; in Brazil 14.4% of those having cataract surgery reported that they had self-medicated at home for the cataract prior to surgery (Rocha, 1997). In the Brazilian setting it has been suggested that the choice of alternative treatments depends on the characteristics of a given community in which tradition, customs and local values play an important role (Temporini et al., 2002)). According to Lane and Millar (1987), eye treatment in Egyptian villages almost always began at home. It may have been either preventive or therapeutic, depending on the condition. Only if “cure” was not achieved within the family was treatment, by either traditional healers or biomedical physicians, attempted. In their study, the vast majority of individuals did not proceed beyond treatment within the family. Health care practiced in eastern Africa is characterized by medical pluralism. The biomedical model, which distinguishes very clearly body, mind and self, is present alongside non-western ethnomedical systems that often don’t make that distinction (Locke and Sheper-Hugues, 1996). These different systems are not mutually exclusive and people often migrate between them according to the perceived symptoms, causes and severity associated with their condition. East African medicine also has “experts”, i.e. traditional healers but Geissler et al. (2002) and Pierce (1993) argue that, unlike in the West, ‘lay” practice is the core of medical knowledge to which specialists only add. Other studies in South America also showed that in some non-western ethnomedical systems there is little to differentiate laypersons and specialized healers in their store of healing knowledge (Rubel and Hass, 1996). Self-treatment is a central part of local medical cultures in African societies, where people are used to taking treatment into their own hands on a daily basis (Deressa et al., 2003). In some settings, common illnesses are dealt with by lay people on their own; only when an illness is prolonged or serious do people seek expert advice, be it a local healer or a biomedical professional, however, this scenario is not universal. Conversely, self treatment can also be viewed as a natural response to a malfunctioning public health system. The functioning of the official health care system is often impaired by a lack of drugs and a lack of staff that are often forced to engage in other activities to supplement their government salary. Consequently, self-treatment may be the only alternative for most people. We sought to determine the frequency and characteristics of self-treatment for eye diseases in rural Malawi to lay the groundwork for a more practical and comprehensive approach to addressing eye diseases in rural communities in Africa. Methods We conducted a population-based survey utilizing a two-stage cluster sample of adults from two districts in the Southern Region of Malawi (Chikwawa District and Zomba District). In each district a list of the villages and their respective populations was generated from the National Statistics Office census demarcated enumeration areas. As Chikwawa was to be the focus of additional qualitative assessment, it was over-sampled (n=500 respondents) compared to Zomba (n=300 respondents). From the list a population proportional to size sample of 25 villages was selected. In each selected village households were selected according to a strategy whereby the first household was a randomly selected distance (based upon the number of households to the edge of the village) in a randomly selected direction from the centre of the village. Each subsequent household was selected as the next nearest door, regardless of direction. Within each household only one person was selected for interview. Selection was based upon presence of the eldest adult (over 20 years) in the household during the enumeration/interview day. Identified respondents were administered a detailed questionnaire regarding their use of eye care services (western and traditional as well as self-treatment), their knowledge and use of traditional eye medicines (TEM), and their perception of the biodiversity of TEM. No clinical examinations were conducted. On average, the questionnaire took 30-45 mins per respondent. For the purposes of this paper, self treatment has been defined as use of either Western or traditional medicines by the individual for their most recent eye condition. All patients reported some past eye problem and the analysis includes all respondents. Eye diseases, conjunctivitis in particular, is very common in most developing countries, however most adults are aware that these diseases are generally not sight threatening. To understand more about conditions found to be those of greatest concern and their anticipated treatment seeking patterns individuals were asked about the eye condition that was of greatest concern to them (using the local language, which does not exactly translate to a specific clinical condition such as cataract, trachomatous trichiasis??, uveitis, conjunctivitis, etc.). Following identification of the eye disease of greatest concern the respondents were asked to whom they would seek care from first (traditional healer, district hospital, or self-treatment) and how much time was needed to determine if treatment was successful. Prior to the start of the survey the interviewers were trained in interview techniques. The questionnaire, developed from in-depth field work prior to the survey, was made in English and local language “Chichewa”. SPSS was used to analyse the results and univariate analyses (chi-square and odds ratios) used to explore associations with reported self-treatment of eye diseases, demographic and reported knowledge, attitudes, and practices of the respondents. Multivariate analyses were also used in order to control potential confounding. The survey was approved by the Malawi National Health Sciences Research Ethics Committee and consent was requested prior to the starting of each interview. ResultsAll the 800 interviews that were conducted were completed successfully, yielding a response rate of 100%. There were significant differences between male and female respondents in terms of baseline demographic characteristics (Table 1). About 65% of women were under 40 years of age compared to 51% of men. Information on age was missing for 56 men and 168 women. The vast majority of the men that participated in the study (91%) were married. Only 74% of women were married. The differences in marital status could be a result of widowhood (12% of women compared to 3% of men) and divorce (10% of women compared to 2% of men). Educational attainment varied by gender with 29% of males having no formal education as compared to 56% of females. Thus men were 4.2 (95% CI 3.1-5.7) times more likely to be literate compared to women. There was no gender difference in terms of housing, which was used as one proxy for socioeconomic status. Among the study population, 318 people (39.8%) reported self-treatment for the last episode of an eye disease. However, there was no difference in self-treatment by district of residence (Table 2). Factors associated with self-treatment were sex (more common among men), religion (more common among Christians), and socioeconomic status (more common among those whose houses were constructed with brick instead of poles and mud). A regression analysis revealed that all three characteristics remained associated with self-treatment. Males were 1.84 times (94% CI 1.58-2.14) more likely to report self-treatment compared to females. Christians were 2.01 times (95% CI 1.64-2.47) more likely than Muslims or those reporting no religion. Those whose house was made of a pole and mud construction were 0.61 times (95% CI 0.52-0.71) more likely to report treatment compared to those with brick (or other more expensive construction material). Possible reasons for reporting self-treatment included perception of treatment from traditional healers, availability of traditional eye medicines, perception of cost of treatments (western, self-treatment, and traditional healers), perceived reliability of successful treatment, and type of eye disease (involving pain, irritation, vision loss). Overall, (Table 3) individuals who reported self-treatment (males in particular) were more likely to view treatment from a traditional healer to be expensive. Most respondents (76.8%) viewed treatment from the health centre or hospital as being the least expensive, however, this varied by treatment modality (self treatment versus seeking medical care). Males were slightly more likely to view self-treatment as the least expensive option compared to females (Table 3). All respondents, regardless of self-treatment or not, were asked if they knew where to find traditional eye medicines; 112 (36.9%) of men reported that they knew where to find traditional eye medicines compared to 110 women (23%, p<0.001). People who self-treated were 3.5 times (95% CI 2.5-4.9, p<0.001) more likely to know where to find traditional eye medicines compared to those who sought treatment. There was no association between self-treatment and other measure of traditional eye medicine availability (e.g., difficulty finding traditional eye medicines (TEM) now as compared to the past). Among the sub-population reporting self-treatment, 229 (72%) reported using traditional eye medicines. Among them, 55.4% used plants near their house (no difference by sex). Individuals were not questioned as to which TEM they used, primarily because of the wide variation in TEM used and issues of intellectual property and indigenous knowledge.
* The unmarried group comprises 13 men and 14 women who were single, 8 men and 60 women who were widowed and 6 men and 51 women who were divorced. ** 27 men and 47 women were Muslim and 41 men and 27 women reported no religion *** There were 22 men and 67 women reporting business, 22 men and 8 women reporting unskilled labor, and 24 men and 3 women reporting skilled labor. Table 2:Reported self-treatment of last eye condition
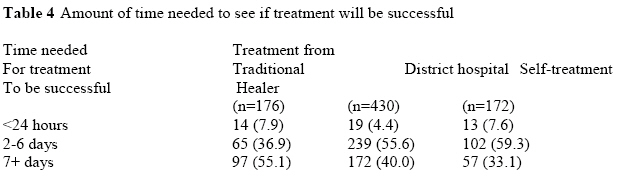
Respondents were asked to identify the eye condition of greatest concern to them and then requested to identify which modality of treatment (district hospital, self-treatment, or traditional healer) is their first choice. The study subjects identified cataract, trachoma and conjunctivitis as serious eye conditions because they cause pain and can result in blindness. Overall, even for these serious eye conditions, 172 (22.2%) still reported that they would resort to self-treatment first, while 176 (22.6%) preferred treatment from a traditional healer and 430 (55.3%) chose for going to the district hospital. Among the different options those electing to use a traditional healer were willing to wait longer for the treatment to be effective than those electing to self-treat or visit the district hospital (Table 4). Furthermore, pain, as a primary condition was more likely to be associated with seeking care at a district hospital compared to relying on self-treatment. The majority of the respondents who opted for self-treatment were those who reported trachoma and conjunctivitis as being severe (47.7% and 45.9% respectively). Only 6% of those who mentioned cataract chose self-treatment. Cataract accounted for 61.4% of those who would go to a traditional healer as compared to 31.8% and 6.8% for conjunctivitis and trachoma respectively. Those who opted for the hospital were more or less evenly distributed across the three diseases with cataract accounting for 34.0% and conjunctivitis and trachoma accounting for 33.7% and 32.3% respectively. Discussion Self-treatment is common in rural Malawi; people treat themselves in order to cope with common eye conditions. On the one hand, it reflects the fact that herbal medicine is common knowledge within most households and considered a legitimate treatment option in the communities. Traditional plants used for eye care are found everywhere in the bush land of Malawi and our findings suggest that most people in the community know about them. This community knowledge of eye care does not seem to be regarded as inferior to that of healers but belongs to a continuum of accepted ways of managing eye diseases. Unlike in Western societies, knowledge of different eye “treatments” is not considered an expert domain, but shared by most community members. Medical specialists, whether biomedical or traditional, are only consulted in special situations (e.g., rare or serious illness). However, even when the eye condition was considered serious, self-treatment was the first choice in 22% of rural Malawians. Our findings on self-treatment suggest that there are no clear borders between biomedical and herbal medicines which are used side by side. Furthermore, it appears that new medicines are incorporated into existing practices. African societies have a long history of incorporating medicines from other peoples, the foreign nature and unknown content of such medicines increasing their perceived power (Prince and Geissler, 2001). Rural Malawians have different expectations of treatment received from health centers, from traditional healers, and through self-treatment. Traditional eye medicines are expected to require more time before “cure” is achieved; this may partially explain the long delays in seeking biomedical care for specific eye conditions (Courtright et al., 1996). The gendered distribution of medical knowledge and patterns of health seeking activities have been extensively reported in Uganda (Geissler et al. 2002). We found gender differences in self-treatment with men more likely to report self-treatment compared to women. As in Uganda, it may be related to the fact that men and women have unequal access to financial resources. It may also be due to the fact that women have more interactions with the public medical system (through Under-Five Clinics) than men. Alternatively, the fact that eye care at health centers and hospitals is provided free of charge may also contribute to this finding. Self-treatment of illness entails a number of health risks. Pharmaceuticals can have toxic effects when used in too high doses or too frequently. Self-medication without knowledge of these risks can have iatrogenic effects. Herbal remedies are not without dangers either. There is the risk that plant products contain toxins, which can be hazardous to the eye or which may interact with Western medicine. Concern has been expressed about the possibility of mixing herbal products and Western medicine in the desire to achieve a more “powerful” treatment (Courtright et al., 2000). Furthermore, experimentation with herbs and visits to traditional healers might delay the patient’s visit to a biomedical practitioner or a health facility. There are few pharmacies in rural Malawi and fewer still who stock eye medicines; in settings where there are community pharmacies it has been noted that pharmaceuticals obtained from shops have had the additional advantage that the shop keepers, who sell the drugs, are fellow villagers. Like the traditional healers in the village, they are integrated in the social network of the villages, which gives their activities transparency. Some of the identified problems in primary eye care in rural Africa reflect weakness in the overall structures: [1] inadequate health facilities, [2] too few trained health personnel; [3] lack of community outreach, [4] poor understanding and tolerance by staff of local health beliefs, [5] declining maintenance of facilities, equipment, and workers skill levels; [6] lack of good management, [7] lack of a clear definition within the front-line health facilities of staff roles, and [8] poor planning. (Lewallen and Courtright, 2001). The weakness of the public health care system makes self-treatment an indispensable complement of rural people’s eye health. Efforts must be made to strengthen front-line infrastructures and systems. Because independent family based medical treatment is rooted in the local medical practices, and because the formal health system is often unable to provide satisfactory medical care, self-treatment will remain common in rural Africa. Instead of ignoring these practices, it is important for eye programme personnel to develop strategies to help people modify existing practices to reach good eye health. Acknowledgements This project was supported by the International Development Research Centre. References
© Copyright 2009 - African. Journal. Traditional, Complementary and Alternative Medicines The following images related to this document are available:Photo images[tc09004t3.jpg] [tc09004t4.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}