 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
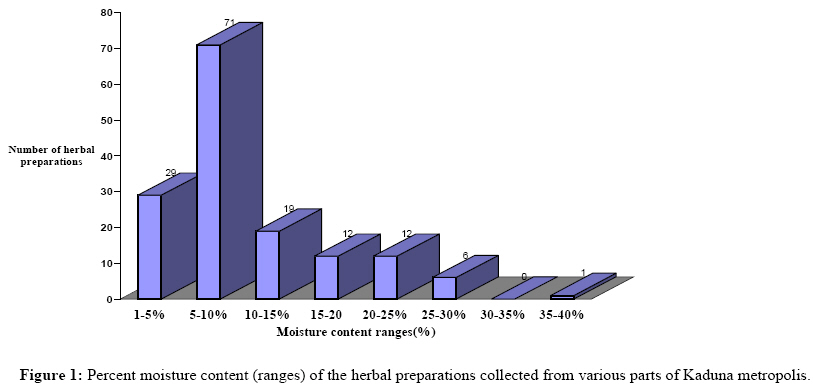
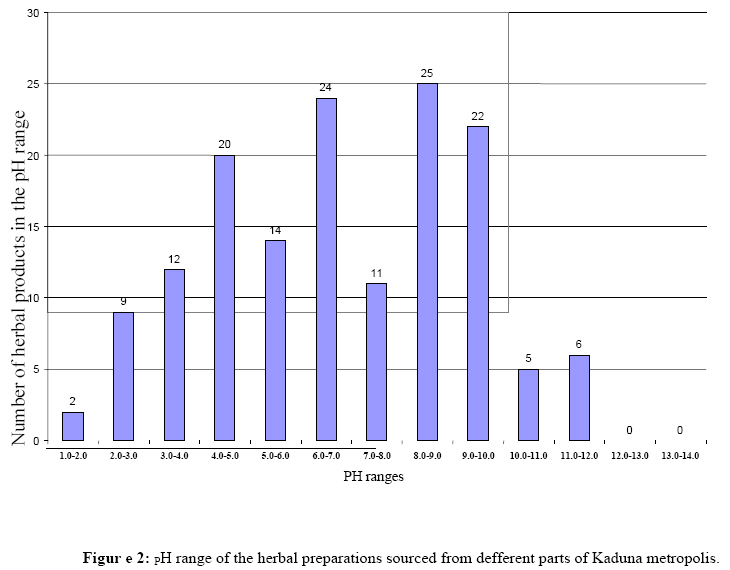
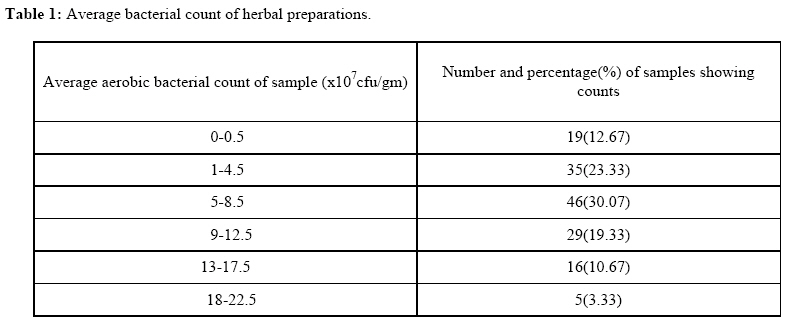
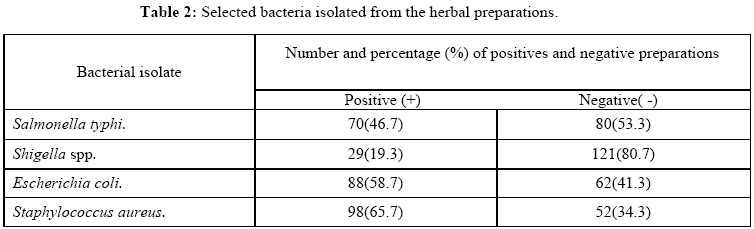
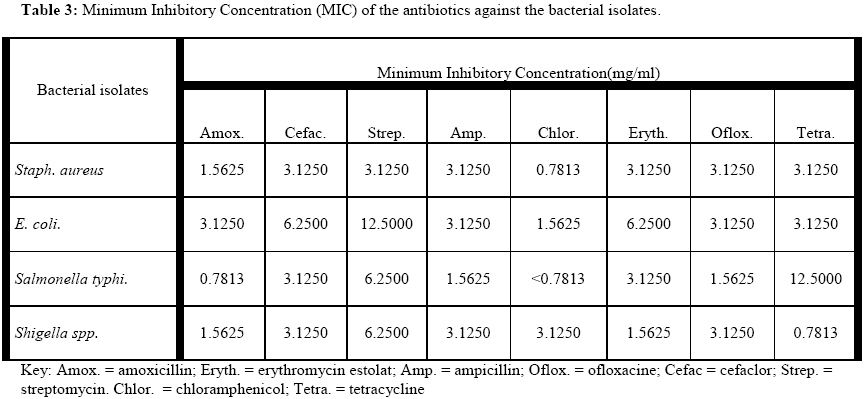
African Journal of Traditional, Complimentary and Alternative Medicines, Vol. 6, No. 1, 2009, pp. 70 - 77 Research Paper Contamination of herbal medicinal products marketed in Kaduna metropolis with selected pathogenic bacteria Danladi Abba, Helen I. Inabo, Sabo E. Yakubu, and Olayeni S. Olonitola,* Department of Microbiology, Ahmadu Bello University, Zaria, Nigeria. *E-mail: olonisteve@yahoo.com Code Number: tc09010 Abstract The study aimed to evaluate the bacterial contamination of powdered herbal medicinal preparations sourced from identified herbal retail outlets in different parts of Kaduna metropolis. The assessments of the contamination of the herbal products were carried out using standard procedures: total aerobic bacterial plate count, measurement of some physical parameters, isolation and characterization of selected bacterial pathogens etc. The results showed that out of a total of 150, 70 (46.67%) herbal remedies were contaminated with Salmonella typhi, twenty nine (19.33%) with Shigella spp. Eighty eight (58.67%) and 98 (65.33%) were contaminated with Escherichia coli and Staphylococcus aureus, respectively. The total aerobic plate count results showed that the highest average count of > 5×107cfu/g was found in 89 (59.33%) of the preparations, while average plate count of ≤5×107cfu/g was found in 42 (28%) and no bacterial count was obtained in 19 (12.67%) of the preparations. Correlation was positive (P = 0.01; r = +0.109) between the physical parameters tested and the bacterial load. Antibacterial activities result of some common antibiotics showed that all the antibiotics had activities on the test bacterial isolates at various minimum inhibitory concentrations. Most traditionally prepared herbal medications in Kaduna state are likely to be contaminated with a wide variety of potentially pathogenic bacteria. The quality assurance of these products should be thoroughly enforced and monitored in the production and distribution of herbal preparations. Key words: Herbal preparations, Kaduna metropolis, bacterial contamination, antibacterial assessment. Introduction The history of using herbs is inextricably intertwined with that of modern medicine. Many synthetic drugs listed as conventional medication were originally derived from plants, for example the antimalarial drug quinine from Cinchona species (Janetzang, 1994). Traditional herbalists in Nigeria use various herbal preparations to treat various types of ailments, including diarrhea, urinary tract infections, typhoid fever and skin diseases (Sofowora, 1993). Most of the herbal preparations are used in different forms and may carry a large number of various kinds of microbes originating from soil usually adhering to leaves, stems, flowers, seed and root of the herbs (Adeleye et al., 2005). The World Health Organization (WHO, 1998) survey indicated that about 70-80% of the world population particularly in developing countries rely on non-conventional medicines mainly of herbal origins for their primary health care. This is because herbal medicines are accessible and cheap (Sofowora, 1993). Therefore, the quality and safety of herbal preparations are also of great concern. The WHO (1993) explained that quality is the basis of reproducible efficacy and safety of herbal drugs, and to ensure the standard of research on herbal medicines, the quality of the plant materials or preparations is of utmost importance. Bauer (1998) showed that the quality criteria for herbal drugs are based on a clear scientific definition of the raw materials. It is difficult to establish comprehensive quality criteria for herbal drugs due to ‘professional secrecy’ of herbalists, but in order to improve the purity and safety of the products, observation of basic hygiene during preparation, standardization of some physical characteristic such as moisture content, pH and microbiological contamination levels are desirable. Previous studies have confirmed the presence of potential contaminants in herbal preparations (De-Smet, 1999). The contaminants that present serious health hazard are pathogenic bacteria such as Salmonella, Escherichia coli, Staphylococcus aureus, Shigella spp and other Gram positive and Gram negative strains of bacteria (Arias et al., 1999; Erich et al., 2001; Wolfgang et al., 2002; Adeleye et al., 2005; Okunlola et al., 2007). A greater number of residents in Kaduna metropolis are believed to depend on traditional herbalists for their medical needs. Unfortunately, no researches (to the best of our knowledge) have been carried out to determine the microbiological safety of these herbal products in Kaduna metropolis. In this paper, the level of contamination of powdered herbal products marketed in Kaduna metropolis with selected pathogenic bacteria and the susceptibility of these contaminants to commonly prescribed antibiotics in the metropolis are reported. Materials and Methods Study area and sampling A total of 150 different herbal preparations were purchased randomly from identified herbal shops and retail outlets in different parts of Kaduna metropolis. Packaged herbal samples were collected and taken to the laboratory, while those that were not packaged (such as herbal preparations sold by local herbalist) were collected in sterile polythene bags (Pearce et al., 2004). All samples collected from the sites were analyzed in the laboratories of Department of Microbiology, Department of Pharmacognosy and Drug Development, Ahmadu Bello University, Zaria and NAFDAC Area Laboratory, Kaduna. Physical analyses Determination of pH The pH of the products was determined (Norris and Ribbons, 1970) by using Hanna Microprocessor pH meter. Sample solution (10%) was prepared by weighing 10g of the sample into 200ml beaker and adding sterile distilled water (100ml) with shaking to obtain a homogenous solution. There after the pH of the preparation was taken with Hanna microprocessor pH meter – pH 211 (Hanna Instruments, UK). Determination of moisture content A Motler Toledo HR73 Halogen moisture analyzer was used to determine the moisture content of the powdered herbal preparations. One gram (1g) was weighed into a clean pan (which was a part of the machine accessories). The analysis was done automatically and the reading was shown in percentage on the screen (NAFDAC SOP, 2000). Bacteriological analyses General purpose nutrient media, enrichment media and other appropriate selective media (all obtained from Oxoid) were employed in the culturing and isolation of selected pathogenic bacteria in the study (Prescott et al., 1999). Preparation of media All dehydrated media were prepared according to manufacturer’s instructions. They were mixed with distilled water and dissolved by gentle heat to boil. The media were sterilized in an autoclave (LTE J7090 model, LTE Scientific Ltd, England) at 121°C for 15 minutes. The sterile media were dispensed or poured into sterilized Petri dishes and allowed to cool. The sterility of the prepared media was checked by incubation of blindly selected plates at 37°C for 24hrs. Total aerobic bacterial plate count The method of Colle and Miles (1989) was used with some modifications. A stock solution of the sample was prepared by weighing one gram (1g) of the sample into 25ml of 0.1% sterile peptone water and shaken thoroughly. A ten-fold serial dilution of the bacterial suspension was made. This was done until 10-7 dilution was achieved. 0.1ml was then pipetted from the 10-7 dilution onto the surface of each of two Petri dishes containing 20ml of a solidified and sterile Plate Count Agar (PCA), and then spread evenly with sterile glass spreader. The plates were then incubated for a maximum of 48 hr at 37°C (including the control plates). Counting of the bacterial colonies was done using the Stuart Digital colony counter. Isolation and identification of Staphylococcus aureus Enrichment of the bacteria was done by adding one gram (1g) of the sample into peptone water in sterile McCartney bottle and incubated for 18 hr at 37°C. Isolation of the Staphylococcus aureus was achieved by streaking the pre-enriched culture from the peptone water on to a selective differential agar plate of Mannitol Salt Agar (MSA) which was freshly prepared following manufacturer’s instructions. The plates were then incubated at 37°C for 24 hr under aerobic conditions. Colonies showing golden yellow colour or colourless were considered to be Staphylococcus and were subjected to biochemical tests such as catalase as well as slide and tube coagulase for the confirmation of Staphylococcus aureus. Isolation and identification of Escherichia coli Enrichment of the bacteria was achieved by adding one gram (1g) of the sample into a sterile McCartney bottle containing sterile nutrient broth and incubated for 24 hr at 37°C. The pre-enriched culture was then inoculated into the selective differential E. coli medium and incubated at 44°C for 24 hr. Inoculum from E. coli medium was then streaked onto the surface of an Eosin methylene blue (EMB) agar and incubated for 24 hr at 44°C. Dark colonies with metallic sheen indicated the presence of lactose fermenters and were confirmed to be Escherichia coli by IMViC tests (Prescott et al., 1999). Isolation and identification of Salmonella typhi Enrichment was done by transferring 1gm of the sample into 10ml of selenite cysteine broth and incubated for 24 hr at 37°C. The enriched culture after incubation was then streaked on duplicate plates of freshly prepared Bismuth Sulphite Agar (BSA), (one lightly and one heavily), and incubated alone with the control plate of Bismuth Sulphite Agar (BSA) at 37°C for 24 hr. After incubation, typical black and green colonies were regarded as positive for Salmonella. The colonies were then streaked on the nutrient agar slants for further biochemical identifications using Triple Sugar Iron (TSI) and Lysine Iron Agar (LIA) tests. Isolation and identification of Shigella spp Enrichment of the bacteria was achieved by introducing 10g of the sample to a prepared sterile nutrient broth with pH adjusted to 8.0 and incubated for 18 hr at 37°C. The pre-enriched culture was then streaked onto the freshly prepared selective differential agar plates of Salmonella-Shigella agar. Incubation was done at 37°C for 48 hr. Non lactose fermenters that grew as colourless colonies were identified with suitable biochemical test such as Triple Sugar Iron (TSI) agar test. Confirmation of Shigella isolates was by serological tests. Antibacterial susceptibility tests To determine the spectrum of antibacterial activity of antibiotics (commonly sold in the study area), the Clinical Laboratory and Standard Institute (CLSI, 2005) method was adopted. Preparation of paper disks The dilution formula below was used to prepare various concentrations of the antibiotics from the stock solutions for the disk potencies (Taura et al., 2004). The dilution formula: V1= R (V2/O) where; V1 = initial volume of the solution. V2 = final volume of the solution. R = required concentration. O = observed concentration. The prepared standard paper discs measuring 6mm in diameter were sterilized in a clean bijou bottle in an autoclave. Preparation of antibiotic stock solutions Standard solutions of antibiotics were prepared by reconstitution of the powder as described by the manufacturers to give a concentration of 125mg/5ml. Doubling dilutions were carried out with the final concentration in the tubes as follows: 25.000mg/ml, 12.500mg/ml, 6.250mg/ml, 3.125mg/ml, 1.563mg/ml and 0.782mg/ml. Disks (100) were placed into each of the six tubes with final concentration of 25.000mg/ml, 12.500mg/ml, 6.250mg/ml, 3.125mg/ml, 1.563mg/ml, 0.782mg/ml respectively until all the solution of antibiotics was completely absorbed and the disks properly impregnated with antibiotics. The impregnated disks were then allowed to dry in LTE IP30- UF oven for 20 mins at 30°C. Test bacteria and antibiotics used for the susceptibility test Bacteria isolated from the herbal preparations were screened for their susceptibilities to the selected antibiotics. They included: Escherichia coli, Staphylococcus aureus, Salmonella typhi and Shigella spp. The antibiotics screened included: amoxicillin, ampicillin, chloramphenicol, erythromycin, streptomycin, cefaclor, tetracycline and ofloxacin. The antibiotics have also been recommended for routine dilution and disk diffusion susceptibility tests (Yolker et al., 2005). Determination of zones of inhibitions using disks diffusion test Clinical Laboratory and Standard Institute (CLSI, 2005) disk diffusion method was employed. To prepare the inocula, five colonies of bacteria were picked from culture media and inoculated into Mueller-Hinton broth and incubated at 37°C for 24 hr. Approximately 0.5ml of the culture was pipetted onto Mueller-Hinton agar surface, and spread evenly with a sterile bent glass rod. A sterile pair of forceps was used to place the appropriate antibiotic test disks on the cultured plates. The plates were then incubated at 37°C for 18 hr. The diameters of the zones of inhibition were measured (to the nearest mm) using a transparent meter rule. Determination of Minimum Inhibitory Concentrations (MIC) This was determined using the broth dilution technique (Prescott et al., 1999). Decreasing concentrations of the desired antibiotic was challenged with standardized bacterial suspension. The lowest concentration of antibiotics that inhibited cell growth, as validated on a recovery broth (nutrient broth supplemented with yeast extract and tween 80), was taken as the MIC. Statistical analysis Chi-square test of association was used to determine if there were associations between the various factors examined. Results The result presented in Figure 1 is the moisture content analysis of the herbal medicinal preparations. Seventy five (50%) of the samples had their moisture contents greater than 8% maximum limit (as required by NAFDAC). The pH analyses in Figure 2 indicated that 24(16%) and 11(7.33%) of the samples were within the pH ranges of 6 to 7 and 7 to 8 respectively, while 2(1.33%) were in the pH range of 1 to 2. Results of the bacteriological analyses of the herbal medicinal preparations obtained are shown in Table 1. A total of 5(3.33%) samples contained average aerobic bacterial count of between 1.8×108 to 2.25×108 cfu/gm, while 19(12.67%) showed bacterial counts between 0-0.5×107cfu/gm. The most frequently occurring member of the selected pathogenic bacteria screened for were Staphylococcus aureus and E. coli. They were isolated in 98(65.7%) and 88(58.7%) of the samples, respectively. Salmonella typhi occurred in 70(50.7%) of the samples, while Shigella spp. was the least frequently isolated and occurred in 29(19.3%) samples (Table 2). The minimum inhibitory concentrations of the test antibiotics against the selected bacterial isolates are presented in Table 3. Salmonella typhi had the least MIC for chloramphenicol (< 0.7813), but had a very high MIC value of 12.5000 against tetracycline. Similarly, E. coli had a very high MIC value (12.5000) against streptomycin. Generally, however, the isolates had very low MIC values against the tested antibiotics. Discussion The results of the moisture content showed that there was remarkable variation among the different herbal preparations sampled. European Agency for the Evaluation of Medicinal products (1998) suggested that water content should be included in the list of comprehensive specifications for herbal medicinal products especially the powdered forms. The maximum moisture content limit of 8% /g of herbal preparations are satisfactory according to National Agency for Food and Drug Administration and Control (NAFDAC SOP, 2000). In this study, 75 (50%) of the 150 herbal products were within, while 75 (50%) were outside the NAFDAC stated limit. Even at less than 8% moisture content limit various pathogenic bacteria were found; but at very low moisture content of less than 6% there were no bacterial counts in some of the herbal preparations. The bacterial counts observed in the 75 (50%) herbal preparations with high moisture contents were high, suggesting that high moisture contents favoured the growth of pathogenic bacteria as well as non-pathogenic ones in herbal preparations. Similarly, the low bacterial counts in the other preparations could be attributed to very low moisture contents. In order to ascertain the correlation between the moisture content and bacterial load, Pearson chi-square correlation test was employed. At 0.01 level of confidence there was positive correlation between moisture content and bacterial counts (r = +0.109) Based on the pH values determined, 43(28.67%) of the herbal products had acidic properties, while 25(16.67%) possessed basic properties and 35(23.33%) were at the neutral range. When the pH value is low (acidic), the bacterial count was observed to be equally low, but at neutral or higher pH the level of contamination of the herbal preparations were observed to be higher. This suggests that a neutral or alkaline pH favoured high contamination levels of the herbal preparations. This agrees with the observation that bacterial growth is optimal at more or less neutral pH, around pH 5-8.5 (Lamikanra, 1999). The limits of bacterial contamination given in European pharmacopoeia as reported by Okunlola et al. (2007) are: total aerobic bacteria (105cfu/g), Enterobacteria and other Gram negative organisms (103cfu/g). Escherichia coli and Salmonella should be absent. The herbal products under study did not meet these specifications in most cases. The samples were contaminated to varying degrees with pathogenic bacteria. Nineteen (12.67%) of the 150 herbal preparations were however free from bacterial contamination, but thirty five (23.33%) had bacterial counts in the range of 1.0×107 to 4.5×107cfu/g; while forty six(30.07%) showed count between 5×107 and 8.5 ×107cfu/g. The bacterial counts, in general, ranged between 1.0×107 and 1.8×108cfu/g. Of concern also is the level of contamination of herbal medicinal preparations by pathogenic Gram negative bacteria. Eighty eight (58.7%) of the samples were contaminated by E. coli, which is an intestinal bacterium and is an indicator for faecal contamination, 70(46.7%) were contaminated by Salmonella typhi and 98(65.7%) by Staphylococcus aureus, while 29(19.3%) were contaminated by Shigella spp. The presence of large numbers of selected pathogenic bacteria in the analyzed herbal medicinal preparations in this study may be due to the methods of their preparation or the equipment and materials used in preparing the herbal medicines. Other possible sources of contaminants are the personnel(s) that could introduce the bacteria when handling the raw materials during processing. Therefore, the process of harvesting, drying, storage, handling and the soil influence the bacteriological quality of raw material which in turns affects the entire quality of the herbal preparation. Thus, manufacturers should ensure the highest possible level of hygiene during manufacturing as well as the lowest possible level of pathogenic organisms in their herbal products so as to maintain correct quality, safety and efficacy of the final herbal preparations. In the present study, the herbal medicinal preparations contained high levels of bacteria, and the counts were beyond the European Pharmacopoeia stated limit, and also carried pathogenic Gram negative bacteria (such as Salmonella, Shigella and E. coli) that are expected to be absent. Coliforms such as E. coli are the most reliable indicators of faecal contamination, thus the test for their presence is an index of the degree of faecal contamination, which may indicate a possible presence of harmful disease-causing organisms (APHA, 1992; Jay 1997). These bacteria constitute the intestinal flora of humans and other animals, and are therefore used as indicator organisms and as an index of possible contamination by human pathogens (APHA, 1992). The significance of faecal bacteria is that if these specific bacteria are present then other harmful microorganisms may also be present, such as Salmonella (Forest, 2004). Therefore, the high recovery rates of these suspected perilous bacteria from indigenous orally consumed herbal medications could be of clinical relevance. Antibiotic susceptibility studies on the bacterial contaminants of the powdered herbal products indicated that the isolates were susceptible to the antibiotics tested. This is not unexpected as it has been previously observed that organisms such as Methicillin Resistant Staphylococcus aureus (MRSA) which are known to be resistant to multiple antibiotics, tend to be susceptible to multiple antibiotics when they are of environmental origins (Shukla et al., 2004; Wylie and Nowicki, 2005). The near uniform antibiotic susceptibilities of the isolates could therefore be because they are of environmental origins and agrees with the observation of Edberg and co-workers (1986) that environmental bacterial isolates are susceptible to most antibiotics because resistance transfer is thought to be much less efficient in the environment where microorganisms are widely separated by distance as compared with human and animal intestines. It may be concluded from this study that most traditionally prepared herbal medications in Kaduna state and Nigeria as a whole are likely to be contaminated with a wide variety of potentially pathogenic bacteria, and that the quality assurance should be thoroughly enforced and monitored in the production and distribution of herbal preparations from the beginning to the final products. References
© Copyright 2009 - African. Journal. Traditional, Complementary and Alternative Medicines The following images related to this document are available:Photo images[tc09010t1.jpg] [tc09010t3.jpg] [tc09010t2.jpg] [tc09010f2.jpg] [tc09010f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}