 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
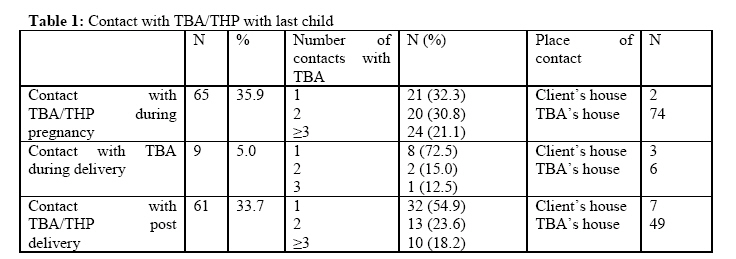
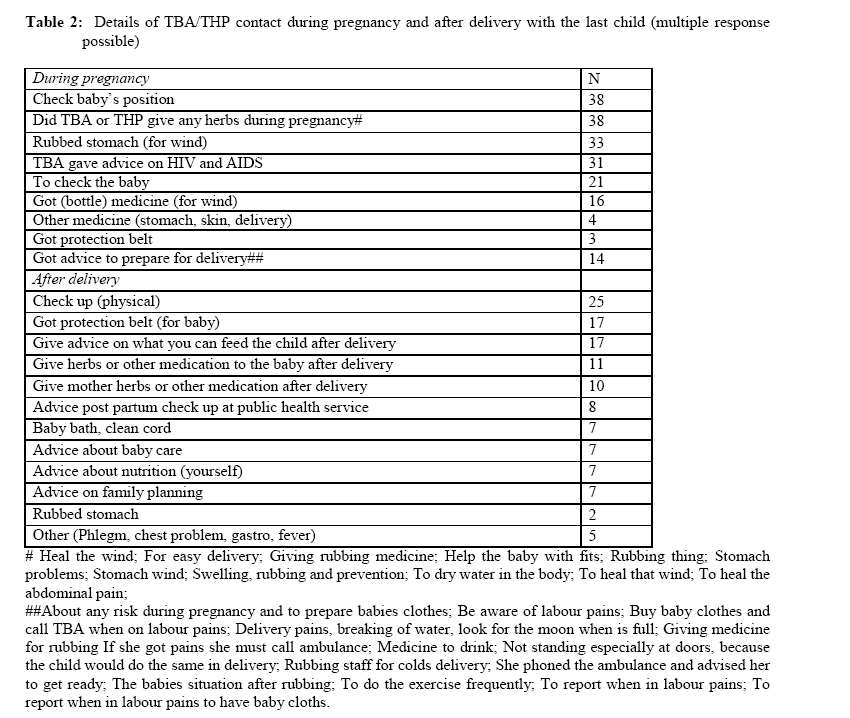
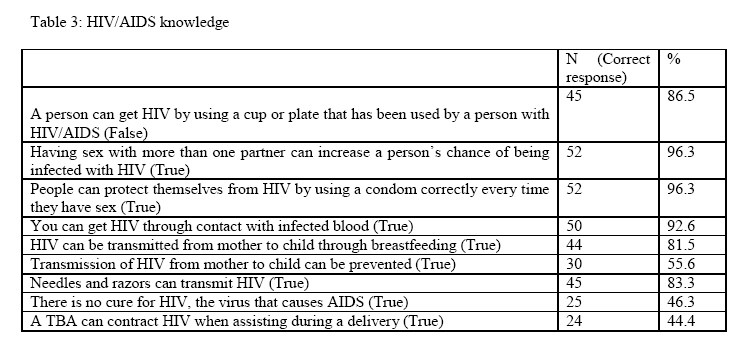
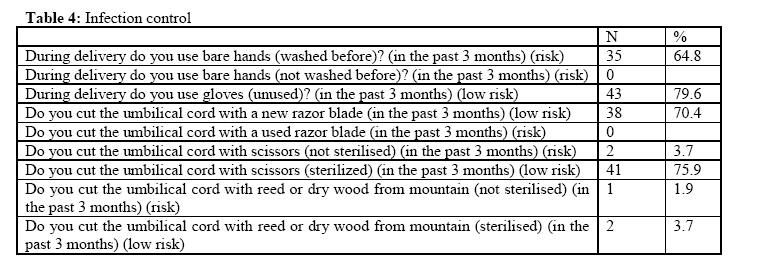
African Journal of Traditional, Complementary and Alternative Medicines, Vol. 6, No. 2, 2009, pp. 155-162 Research Paper USE OF TRADITIONAL AND COMPLEMENTARY HEALTH PRACTICES IN PRENATAL, DELIVERY AND POSTNATAL CARE IN THE CONTEXT OF HIV TRANSMISSION FROM MOTHER TO CHILD (PMTCT) IN THE EASTERN CAPE, SOUTH AFRICA Karl Peltzera , Nancy Phaswana-Mafuyab and Latasha Tregerc aSocial Aspects of HIV/AIDS and Health, Human Sciences Research Council, Pretoria, South Africa& Department of Psychology, University of the Free State, Bloemfontein, South Africa. Code Number: tc09021 Abstract The aim of this study was as part of a baseline assessment in PMTCT in the traditional health sector: a) to determine the views of women who have used the services of traditional practitioners before, during and/or after pregnancy, and b) to conduct formative research with traditional health practitioners (THPs), i.e. herbalists, diviners and traditional birth attendants (TBAs) on HIV, pregnancy care, delivery and infant care. The sample included a) 181 postnatal care clients with a child less than 12 months interviewed at postnatal clinic visits from 20 primary care clinics in the Kouga Local Service Area (LSA), Cacadu district, Eastern Cape, and b) 54 traditional birth attendants (TBAs) and 47 herbalists and/or diviners were interviewed from Kouga LSA. Results showed that THP (in particular TBAs and to a certain extend herbalists/diviners) play a significant role in pregnancy and postnatal care, and also with the assistance of delivery. Certain HIV risk practices were reported on the practice of TBAs. THPs also seem to have some role in infant feeding and family planning. THPs should be trained in optimising their services in pregnancy and postnatal care, and preparation for health facility delivery. In addition, they should be trained on HIV risk practices, HIV/AIDS, HIV prevention including PMTCT, infant feeding and family planning. Key words: Traditional medicine, traditional practices, complementary medicine, prenatal care, postnatal care, delivery, infant care, HIV, PMTCT, Eastern Cape, South Africa Introduction Abrahams et al. (2002) studied indigenous healing practices and self-medication among pregnant women in Cape Town, and found that the majority of Xhosa speaking women follow indigenous health practices for both themselves and their babies because of the need to “strengthen” the womb against witchcraft or sorcery, to prevent childhood illnesses, and to treat symptoms they perceive that biomedical services would not be able to treat. Selfmedication with non-prescribed drugs, herbs and Dutch remedies was common among Afrikaans speaking women. Herbs and Dutch remedies were mainly used to treat indigenous illness (baarwind) while over-the-counter drugs were used to treat minor ailments associated with pregnancy. In pregnancy, herbs or minerals are often used as a tonic to clean the womb, to ease delivery, to induce labour, and to protect the child from evil and have a healthy child (Henda and Peltzer, 2005; Van der Kooi and Theobald, 2006; Varga and Veale, 1997). According to Nolte (1998) Traditional Birth Attendents (TBAs) can be characterized in South Africa as a middle aged or elderly lady with no formal training, who acquired her skills through experience and attends to women during pregnancy, labour and the postnatal period in different ways. This may include advice or instructions as to what to eat, what not to eat, the giving of herbal remedies for pain, sickness or discomfort; abdominal massages, offering comfort to mothers, giving them a sense of security. They also assist with the delivery of the baby and advise and assist the new mother on how to care for the baby after it is born (Department of Health, 2004). A number of authors have indicated the importance of traditional birth attendants in the delivery of health care to the mother and child in South Africa (Nolte, 1998; Jepson and MacDonald, 1988; Selepe and Thomas, 2000; Troskie, 1997). Little is known about the role of traditional healers (herbalists or diviners) in obstetric care. Oyebola (1980) interviewed a group of 106 Yoruba traditional healers who practice midwifery and found that these herbalists are indispensable to delivery services in Nigeria. Bulterys et al. (2002) noted that traditional (or "trained") birth attendants could play a critical role by reaching pregnant women not currently receiving formal antenatal care and by assisting with delivery of primary services designed to prevent HIV transmission. Trained birth attendants could oversee the provision of nevirapine to women infected with HIV who give birth at home and to their newborn infants. Traditional birth attendants could also counsel women and their partners on how to reduce the risk of HIV being transmitted to the child, focusing particularly on the postpartum period. A different view is held by Berge (2003) arguing that the TBAs cannot be expected to carry out HIV/AIDS prevention and treatment activities (to administer HIV tests or deliver antiretroviral drugs to women giving birth at home) because of their lack of resources and skills. In developed countries one can argue this but in developing countries this argument is questionable. WHO (2004) notes that TBAs have the potential for improving maternal and newborn health at community level. The role of TBAs in caring for pregnant women and conducting deliveries is acknowledged, but generally TBAs are not trained to deal with complications. The aim of this study was as part of a baseline assessment in PMTCT in the traditional health sector: a) to determine the views of women who have used the services of traditional practitioners before, during and/or after pregnancy, and b) to conduct formative research with traditional health practitioners (THPs) i.e. herbalists, diviners and traditional birth attendants (TBAs) on HIV, pregnancy care, delivery and infant care. Method Sample and procedure (postnatal clients) The sample included 181 postnatal care clients with a child less than 12 months old chosen from consecutive postnatal clinic visits at convenience from 20 primary care clinics in the Kouga Local Service Area (LSA), Cacadu district, Eastern Cape. Half (50.7%) of the participants were between 18-25 years old, 39.9% 26-35 years and 9.4% 36 years and older; 27.5% had less than Grade 8 education, 60.1% between Grade 8-11, and 12.3% Grade 12 education. The racial background was 69.6% Xhosa, 29.0% Coloured, and 1.4% other. Most (76.3%) indicated that they were single and 23.7% married or co-habitating; 52.2% were living in their parent’s house, 42% in their own house and 5.8% in the house of the in-laws. Most (74.6%) indicated that they were unemployed, 23.2% employed and 2.2% self-employed at the time of the survey interview. Nine in ten women indicated that their family income was less than R3000 per month, 1% R3000 and more and 9%, no income. Mothers with an infant from 0-6 months were 37.8% and from 7-12 months were 62.2%. Postnatal clients were interviewed with a semi-structured questionnaire by a trained external researcher after informed consent was obtained and the client was exiting the primary care facility. All clients approached agreed to participate in the study. A semi-structured questionnaire for THP clients included biographic and health care information, information on the last delivery, contacts/relationship with TBAs, THP, HIV and AIDS, antenatal care, obstetric care, post-partum care, and counselling on safe infant feeding for HIV exposed newborn babies. Sample and procedure (traditional health practitioners) The sample included 54 TBAs from Kouga LSA, 27 from Kouga municipality, 12 from Koukamma and 15 from Sundays river municipalities. Except for one, all TBAs were older than 45 years; two in three (68.5%) were Coloured and 31.5% Xhosa by racial or ethic background; 49% had either no formal education or up to Grade 4 education. 24.5% had Grade 6-7, and 26% had more than Grade 7 formal education. The 54 TBAs interviewed fall into the categories of (1) traditional birth attendants only (85%) and (2) TBA and herbalist or diviner (15%). Two of the TBAs were registered with the Traditional Health Practitioners Council, while 52 were not. Most TBAs received their training as a TBA from their mother (n=26), followed by grandmother (n=16), other relative (n=10) and selftrained (n=2). In addition, 47 herbalists and/or diviners were interviewed from Kouga LSA, 17 from Kouga municipality, 12 from Koukamma and 18 from Sundays river municipalities, using a similar procedure as above; 46 were Xhosa and 1 Coloured, 17 Male and 30 female, 25 (53.2%) were registered with the traditional healer’s council; 70% saw less than 10 patients a month. TBAs and herbalists and/or diviners were recruited from existing lists of the traditional health practitioner coordinating office in Cacadu District, through key informants in 20 primary care clinics in Kouga LSA and community members. They interviewed with a structured questionnaire after informed consent had been obtained by a trained researcher at their homes or surgeries. The interview schedule and questionnaire were translated and administered in IsiXhosa and Afrikaans by two trained HSRC researchers. A semi-structured questionnaire was used for herbalists/diviners and it covered sections on biographic information, practice characteristics, HIV attitudes, risk perceptions and practices, referral, family planning, pregnancy and infant care. The HSRC research ethics committee and the Eastern Cape Department of Health approved the study protocol. Results Results are divided into findings from interviews with (1) postnatal clients and (2) traditional health practitioners. Postnatal clients Eighty-three (45.9%) of the clients reported that they had never consulted a traditional health practitioner (THP); 36% had consulted a THP (including a traditional birth attendant=TBA) with their last pregnancy (more than half of them 51.9%) more than once. The traditional birth attendance was only 5% in this sample, while 34% utilized THPs or TBAs for postnatal care. The place of consultation with the THP or TBA was mainly at the surgery or home or the THP or TBA (Table 1). The most frequent reason for consultation with a THP/TBA during pregnancy was (1) check baby’s position, followed by (2) rubbing stomach (for wind), (3) checking the baby, (4) getting medicine (for wind). Only 14 (16.7%) got advice from the TBA about preparing for delivery about risk signs during pregnancy, frequent exercise, not standing especially at doors (because the child would do the same in delivery), to be aware of labour pains, call TBA/ambulance when labour pains/begins and prepare baby cloth. After delivery the most frequent postnatal traditional care was (1) (physical) check up, followed by (2) “got protection belt” (for baby), (3) infant feeding advice, (4) referral to health facility for postnatal care, (5) baby bath and cleaning the cord, (6) advice on nutrition of the mother, (7) family planning and (8) medicines for various ailments for the mother and infant (Table 2). Attitude about taking traditional medicine Most postnatal clients (64, 86.5%) did not tell their obstetric care provider if they were taking traditional medicine, one in five (19.5%) think that telling their obstetric provider about having used traditional medicine would affect the care (negatively) given by the obstetric care provider, and nine (12.3%) believed that traditional herbs can hurt unborn baby. The treatment of infant with traditional and complementary medicine included in order of frequency (1) gripe water (for the wind) (24.3%), (2) pharmaceutical agent (over-the-counter drug) (13.8%), (3) rooibos tea (9.9%), (4) galactogogue (a galactagogue is any substance that stimulates lactation, hence it increases milk production) (8.8%), and (5) traditional medicines given to the infant (8.3%). Home delivery Most women gave birth at health facility (93.4%) and their babies were delivered by nurses (48.6%) and doctors (38.3%). From 11 mothers who had delivered their last baby with the TBA all said that their TBA washed her hands before assisting in the delivery, and 8 used a new razor blade but 4 had not used gloves, 3 had used herbs for cleaning the umbilical cord, and only 2 asked about nevirapine (administration) (n=2). Traditional health practitioners TBAs Most TBAs reported to be involved in pregnancy care (88.9%), prenatal check-ups (75.9%), conducting a postpartum visit (76.9%), assess the baby’s position in the uterus (75.9%), family planning (90.7%) and only a few took the mother’s (9.3%) pulse, checked the mother if she had taken nevirapine (18.5%), and conducted abnormal or complicated deliveries (3.7%). HIV/AIDS knowledge Most had good HIV transmission knowledge (more than 80% correct responses), while only 56% knew that the transmission of HIV from mother to child can be prevented, 46% knew that there was no cure for AIDS and only 44% knew that they can contract HIV when assisting during delivery (Table 3). Infection control TBAs were asked about infection control practices. Although 64.8% reported using their bare (but washed) hands during delivery; 79.6% reported the use of gloves; 70.4% reported cutting the umbilical cord with a new razor blade or with sterilised scissors (75.9%) (Table 4). Herbalists and/or diviners (n=47) Almost one in two of the herbalists and/or diviners (48.9%) indicated that pregnant women consult them during their pregnancy, with 85% saying they would come more than once during pregnancy. Reasons for such consultations included:
The reported THP treatments prior to delivery varied from rubbing, medicines for bathing or ingestion to referral to TBAs or the clinic. Reported post-partum care included checking of mother and infant; advice on breastfeeding; medicines for baby protection or for ingestion and referrals to the clinic. Limitations of the study This study uses a convenient sample and was by self-report. Postnatal clients may not have felt free to answer questions on traditional health practices being interviewed in a health care facility. So findings cannot be generalised to the study area. Discussion The study found that THP (in particular TBAs and to a certain extend herbalists/diviners) play a significant role in pregnancy and postnatal care, and also with the assistance of delivery. Certain HIV risk practices were reported on the practice of TBAs. THPs also seem to have some role in infant feeding and family planning. In this study 83 (45.9%) of the clients reported that they had never consulted a traditional health practitioner (THP); 36% had consulted a THP (including a traditional birth attendant=TBA) with their last pregnancy (more half of them 51.9%) more than once. In a similar study among postnatal women in Lusaka, Zambia, 21% reported using a traditional healers during the current pregnancy, and Bland et al. (2004) found that 26% of the mothers had consulted a traditional healer at some point in the first 12 weeks of life. Abrahams et al. (2002) found also among the majority of Xhosa speaking women that they follow indigenous healing practices for both themselves and their babies because of the need to “strengthen” the womb against witchcraft, to prevent childhood illnesses and to treat other symptoms. Other studies also found the use of herbs/home remedy such as Isicakathi, Isihlambezo (Agapanthus sp. L’Herit), which is a plant used by the expectant mother from the period she is six months pregnant until the baby is born. Pharmacological analysis suggests the possibility of both therapeutic and harmful consequences (Dlisani and Bhat, 1999). The treatment of infants in this study with traditional and complementary medicine included in order of frequency (1) gripe water, (2) pharmaceutical agent (over-the-counter drug), (3) rooibos tea, (4) galactogogue, and (5) traditional medicines. A similar wide distribution including herbs and gripe water (the latter contains sodium bicarbonate and alcohol and is used to relief ‘colic’ or ‘wind’ or perceived abdominal pain) was found in a study on the use of non-prescribed medication in the first three months among the Zulus in rural South Africa (Bland et al., 2004) and other studies (Abrahams et al., 2002; De Wet, 1998; Cocks and Dold, 2000; Cocks and Moller, 2002). It is possible that the perceived benefits of Gripe water may be partially caused by the relaxation and sleep-inducing effects of the alcohol (Bland et al., 2004). Whilst the administration of non-prescribed medications may not cause any clinical problems, they may be dangerous, may interfere with appropriate health-seeking behaviour and preclude compliance with breastfeeding as recommended by the World Health Organisation (Bland et al., 2004; Mabina et al., 1997; Varga and Veale, 1997). Traditional healers are highly valued providers who are often consulted for the procurement of traditional preparations for infant use (Sibeko et al, 2005; Varga and Veale, 1997). In this study most postnatal clients (86.5%) did not tell their obstetric care provider if they were taking traditional medicine, one in five (19.5%) thought that telling their obstetric provider about having used traditional medicine would affect the care given by the obstetric care provider, and 88% of the women did not believe that traditional medicines can hurt an unborn baby. Banda et al.. (2007) found among the Lusaka sample that 64% stated that if they sought care from a traditional healer, they would not share this information with their obstetric provider; 54% believed that admitting to a visit to a traditional healer would result in worse medical care; and 61% said that traditional herbs can hurt unborn baby. Women may be unwilling to discuss with their obstetric care provider the use of traditional and complementary medicine, since it could be considered unacceptable. Health care providers need to take into consideration the use of traditional and complementary medicines of their obstetric patients. Most TBAs reported to be involved in pregnancy care, prenatal check-ups, conducting a postpartum visit, family planning, but only a few checked the mother if she had taken nevirapine. TBAs had good HIV transmission knowledge (more than 80% correct responses), but only 56% knew that the transmission of HIV from mother to child can be prevented, 46% knew that there was no cure for AIDS and only 44% knew that they can contract HIV when assisting during delivery. Almost half of the herbalists and/or diviners (48.9%) indicated that pregnant women consult them during their pregnancy; 85% said that the pregnant women would consult them more than once during pregnancy. It is revealing that herbalists and/or diviners play such an important role in antenatal care, and further research should be conducted on this. Although some health care providers remain suspicious of traditional remedies, most agree that traditional healers can play an important complementary role in health care provision (Bodeker et al., 2006; Baggaley et al., 1996; Burnett et al., 1999; Bulterys et al., 2002). Use of traditional medicines on infants and consultation with traditional healers seem to be common. The importance of recognizing and directly addressing the use of traditional medicines is reiterated in this study. Health programmes that neglect this matter may be missing important opportunities to provide education and minimize drug interactions. Health care providers must open lines of communication with traditional healers and with mothers to maximize PMTCT programme success. Given the use of traditional medicines, incorporation of traditional healers into health initiatives could be an effective strategy for meeting selective health needs (Bodeker et al., 2006; Ndulo et al., 2001; Nations and Souza, 1997). THPs should be trained in optimising their services in pregnancy and postnatal care, and preparation for health facility delivery. In addition, they should be trained on HIV risk practices, HIV/AIDS, HIV prevention including PMTCT), infant feeding and family planning (Peltzer and Henda, 2006). Acknowledgements This study was supported by Cooperative Agreement number 1U2G PS 000570-01 from the US Centers for Disease Control and Prevention (CDC). Special thanks to the Eastern Cape Department of Health Management, and in particular to the Kouga LSA staff and managers, in particular Ms Joyce Nakupi, for their support. We also thank Laetitia Rispel for her input and comments on parts of the draft of the paper. References
© Copyright 2009 - African. Journal. Traditional, Complementary and Alternative Medicines The following images related to this document are available:Photo images[tc09021t1.jpg] [tc09021t4.jpg] [tc09021t3.jpg] [tc09021t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}