 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Traditional, Complementary and Alternative Medicines, Vol. 6, No. 3, 2009, pp. 275-280 Research Paper KNOWLEDGE, ATTITUDE AND USE OF ALTERNATIVE MEDICAL THERAPY AMONGST URBAN RESIDENTS OF OSUN STATE, SOUTHWESTERN NIGERIA 1 *Bamidele, James Olusegun, 2Adebimpe, Wasiu Olalekan., 1Oladele, Edward Adekola. 1Department of Community Medicine,LAUTECH College of Health Sciences, Osogbo, Osun State.
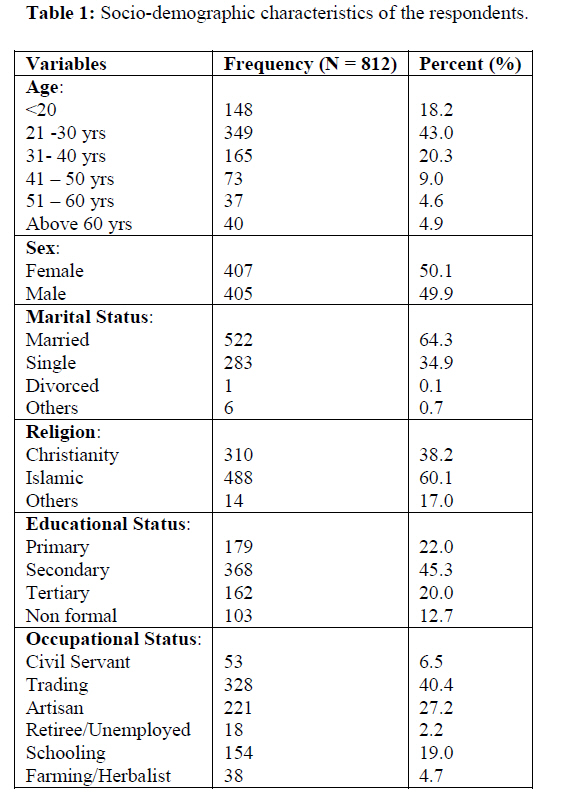
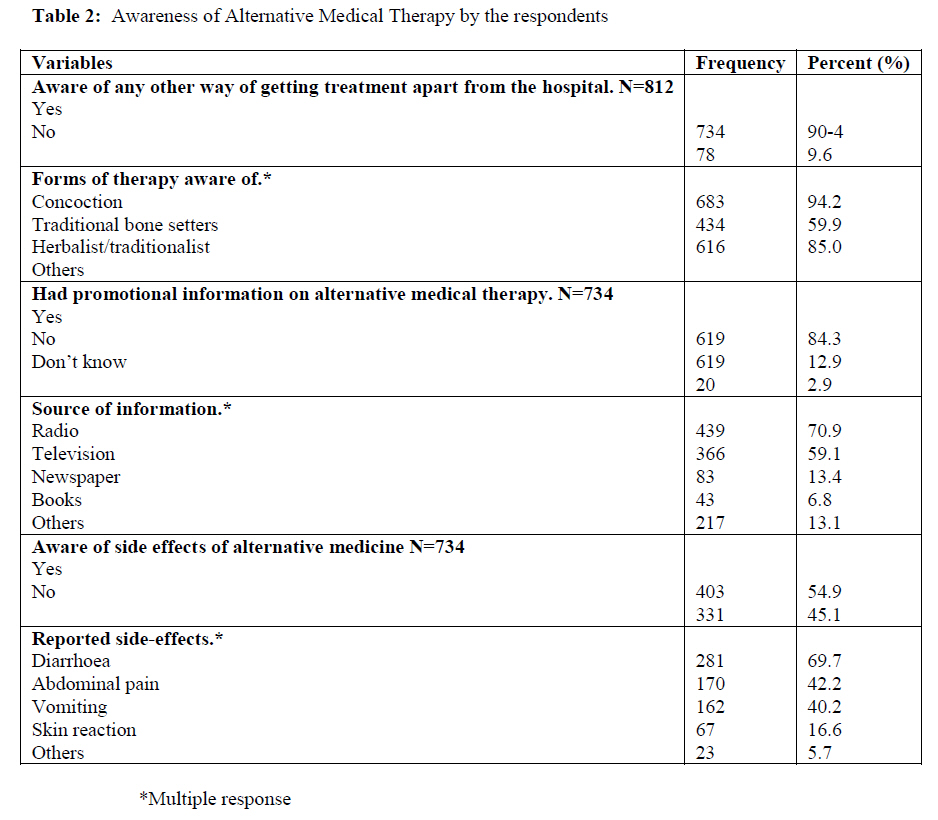
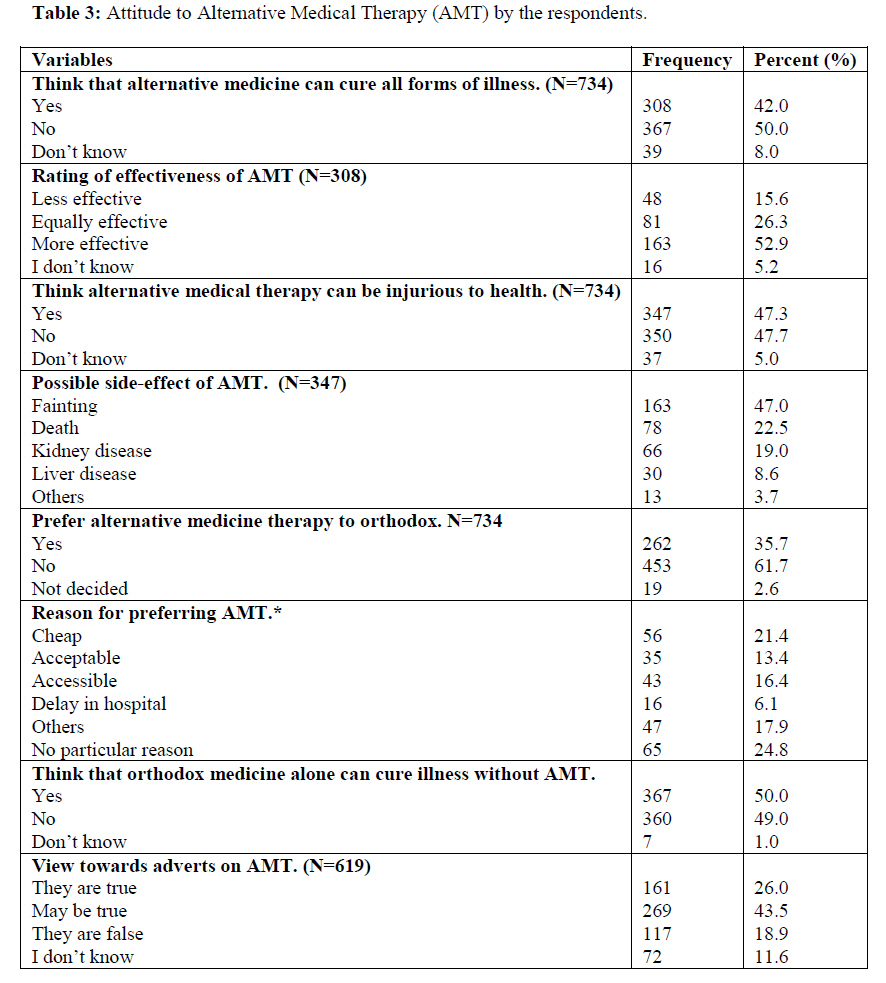
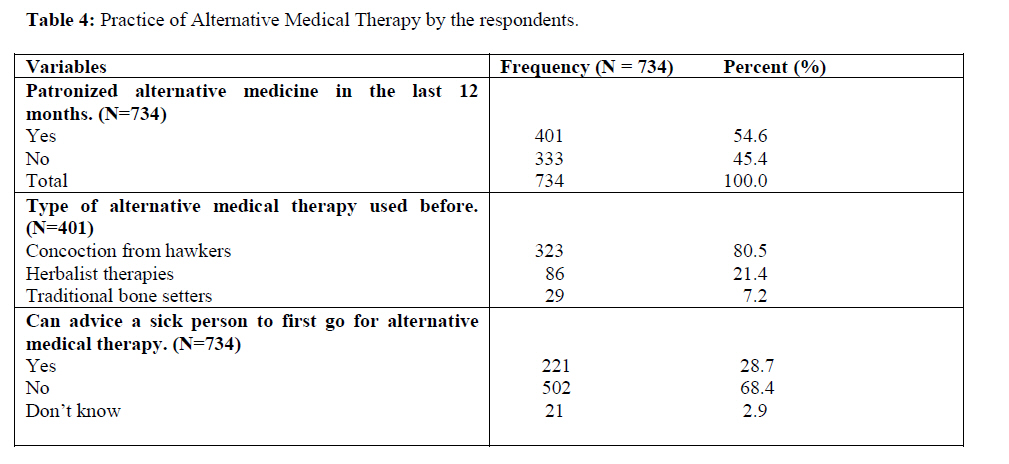
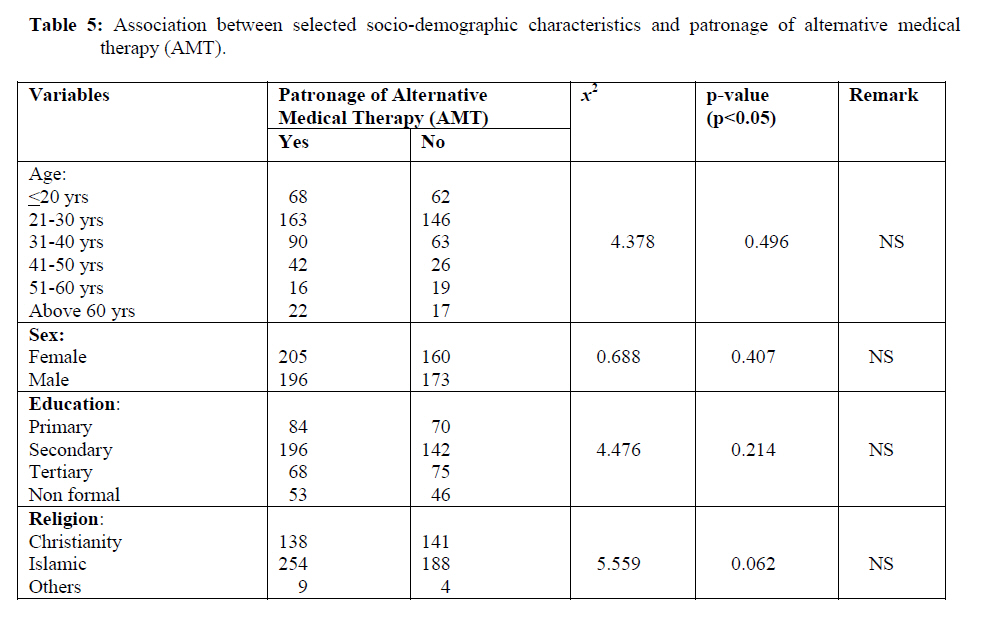
Nigeria. Code Number: tc09038 Abstract Alternate medicine which has a long history has been relegated to the background by the evolution of modern medicine. In recent times, however, alternative medical therapy has been growing in popularity and getting increasing attention and interest. This study assessed the knowledge, attitude and use by urban dwellers of alternative medical therapies. This was a cross-sectional descriptive study which used a semi-structured questionnaire to gather information from 812 randomly selected urban respondents. Majority 734 (90.4%) of the respondents were aware of an alternative way of getting treatment for their ailments apart from the orthodox medicine. The forms of alternative medical therapy (AMT) respondents were aware of include: concoction (herbal preparations) 683 (94.2%); herbalists/traditionalists 616 (85.0%); traditional bone setters therapy 434 (59.9%); among others. The main source of information was through radio 439 (70.9%). About half 403 (54.9%) of the respondents were aware of side effects from AMT and these include diarrhea, abdominal pain and vomiting which accounts for 69.7%; 42.2% and 40.2% respectively. About 347 (47.3%) think AMT could be injurious to health. About a third 262 (35.7%) of the respondents who were aware of AMT prefers it to orthodox medicine. Reasons given for the preference were that: AMT is cheap 56 (21.4%); accessible 43 (16.4%) and acceptable 35 (13.4%) to them. About half 367 (50.0%) also believed AMT alone could cure their illness without resort to orthodox medical therapy (OMT). Over half 401 (54.6%) of the 734 respondents that were aware of AMT had patronized or taken one form of alternative medical therapy or the other in the last 12 months prior to the study. Of these number, 323 (80.5%) had taken concoction (herbal preparations). However, there was no relationship between respondents’ age, sex, educational level or religion and the patronage of AMT as all test of associations were not statistically significant p>0.05. This study has revealed that the use of alternative medical therapies is quite popular among the studied population and a high proportion of the respondents use AMT notwithstanding that they live in the urban communities where they have better access to orthodox medical care and medical practitioners. Regulations should be made concerning the advertisement of alternative medicine and practices as orthodox medicine and practices are usually not advertised. Key words: Knowledge, attitude, use, alternative medical therapies, urban dwellers Introduction Alternative medicine has been around for a long time and happens to be the origin of scientific medicine as we know it today. The evolution of modern medicine has confined alternative medicine into the backstage. In recent times, however, alternative medicine has been growing in popularity and getting increasing attention and interest as earlier noted by Stephen et al (2003). David (1997) in his write-up defined alternative therapies as medical interventions that are neither taught in medical schools nor generally available in hospitals. Angeli and Kassirer (1998) also described alternative medicine as practices used in place of conventional medical treatments; which includes practices that incorporate spiritual, metaphysical, or religious underpinnings; non-European medical traditions, or newly developed approaches to healing. He further stated that alternative medicine is any treatment where the efficacy and safety has not been verified through peer-reviewed, double blind placebo controlled studies, regarded as ‘gold standard’ for determining the efficacy of a compound. In the pre-colonial era in Nigeria as highlighted in the Nigerian Health Review (HEBRON, 2006), all communities had some form of organized social structure, an important component of which was a health care system (HERFON, 2006). Attention for the provision of personal health care usually centered on individuals with expertise in preventive, curative, and rehabilitative medicine. The knowledge, skills and expertise of the traditional health practitioners were passed down the generations within families, to kith and kin. Such knowledge and skills were closely guarded secrets because the practitioners made their living and sustained their dependants with income from the successful provision of personal health care. There was of course an admixture of witchcraft and traditional herbalism, with the use of crude forms of therapeutically active concoctions, shades of which still persist in some communities (HERFON, 2006). In Nigeria, as noted in the Word Health Assembly resolution 56.31 (WHO, 2003), traditional medicine is partially recognized as forming a part of the national health delivery system. Some components of traditional medicine are included as part of national health policy and, hence, are governed by a single or a set of different national legislative measures. This practice has continued to be a main source of health care in the rural communities since modern medicine has not been able to reach the majority of the populace. It has been relatively non-popular in the urban areas since modern or orthodox medical practice and practitioners are mostly located in the urban settings and therefore quite accessible to the urban dwellers. However, there seems to be a resurgence of interest by residents in the urban communities as the alternative medical therapists now pay for extensive air time on government radio and television to announce their wares which they said could cure any disease ever known to mankind. It is now common to see many urban dwellers trooping into stadia and trade fair centres of our state capitals to visit alternative medical therapists’ stands to consult and buy these untested remedies. As documented in the Traditional Medicine Policy and Regulatory Framework (2006), there are currently 107 registered herbal medicines in Nigeria, but none is listed on the essential drugs list. A post-marketing surveillance system is in development. Herbal medicines are still commonly sold by practitioners and their agents virtually without any restriction. However, a great deal of informality still exists, i.e. the traditional herbal medical practitioners follow very informal and highly varied protocols. These constitute a grave danger to the health of members of the public. There is great concern among orthodox medical practitioners on cases of medical complications from the usage of AMT and the need to stem the trend has brought about the need to carry out this study. This study assessed the knowledge, attitude and use by urban dwellers of alternative medical therapies. It is hoped that the findings from the study will help policy makers to plan for control measures against any health hazards from abuse of alternative medical therapy. Material and Methods This is a cross-sectional descriptive study which used a semi-structured questionnaire to gather information from randomly selected respondents. A total of 812 randomly selected adults took part in the survey from the headquarters of 15 Local Government Areas (LGAs). These LGAs were initially selected by simple random sampling method by balloting from the 30 LGAs of Osun State. The questionnaire was either self administered by the individual respondent or by interview by the trained research assistants where necessary. The questionnaire elicited information on the respondents’ socio-demographic characteristics, knowledge of alternative medical therapies (AMT), and their attitude towards it and if they have ever patronized AMT in the last 12 months prior to the study. Their views about its efficacy and reasons for patronage were also sort among others. All questionnaires were cross-checked to ensure completeness, entered into a computer and analyzed using the statistical package for social sciences (SPSS). Cross tabulations of variables were constructed and chi-square and p-values were calculated to determine the statistical significance if any. Significant p-value was predetermined at p<0.05. Results A total of 812 respondents participated in the study. Their mean age was 32.1+/-13.3; modal age group was 21-30 years. Half (50.1%) of respondents were female; 95.4% belong to the Yoruba ethnic group; 60.1% were Moslems; while 38.2% were Christians. Five hundred and twenty-two (64.3%) respondents were married and 283 (34.9%) were single. Almost two-third 530 (65.3%) has secondary education and above; 179 (22.0%) had primary education; while 103 (12.7%) had no formal education. Respondents were mostly traders 328 (40.4%); artisans were 221 (27.2%); 154 (19.0%) were still in school, while farmers/unemployed/retirees made up of only 53 (6.9%) and civil servants 53 (6.5%). Majority 734 (90.4%) of the respondents are aware of an alternative way of getting treatment for their ailments apart from the orthodox medicine. The forms of alternative therapy respondents are aware of include: concoction (herbal preparations) 683 (94.2%); traditional bone setters therapy 434 (59.9%); herbalists/traditionalists 616 (85.0%) among others. The main sources of information are usually through radio 439 (70.9%) and television 366 (59.1%). Newspaper and books only account for 20.2%. Only about half 403 (54.9%) of the respondents are aware of any side effects from alternative medical therapy (AMT). The main side effects respondents are aware of are diarrhea, abdominal pain and vomiting which accounts for 69.7%; 42.2% and 40.2% respectively. As many as 308 (42.0%) of all the respondents who are aware of AMT believe that it can cure all forms of illness and over half of these number 163 (52.9%) rated alternative medicine as more effective than orthodox medicine. About 347 (47.3%) think AMT can be injurious to health. Fainting 163 (47.3%); death 78 (22.5%); kidney disease 66 (19.0%) and liver disease 30 (8.6%) are what the respondents think AMT can cause to users. More than a third 262 (35.7%) of the respondents who are aware of AMT prefers it to orthodox medicine. The reasons for the preference are that: it is cheap 56 (21.4%); accessible 43 (16.4%) and acceptable 35 (13.4%) to them. About half 367 (50.0%) also believe AMT alone can cure their illness without resort to orthodox medical therapy (OMT). As many as 430 (69.5%) believe the advert on AMT are true or may be true. Over half 401 (54.6%) of the 734 respondents that are aware of AMT had patronized or taken one form of alternative medical therapy or the other in the last 12 months prior to the study. Of these number, 323 (80.5%) had taken concoction (herbal preparations); 86 (21.4%) had taken herbalists’ therapies; while 29 (7.2%) had visited the traditional bone setters. Some 211 (28.7%) would advise a sick person to first go for AMT instead of orthodox medical therapy. However, there is no relationship between respondents’ age, sex, educatioeducational level or religion and the patronage of AMT as all test of associations were not statistically significant p>0.05. Discussion Treatment of diseases using traditional remedies is an age old art which has been confined into the backstage due to access to western biomedicine, adequate education, employment opportunities and economic growth in most families especially in the urban communities in Nigeria. It is common knowledge the rural-urban dichotomy in which majority of the health professionals and government health institutions are located in the urban communities; while very few are found in the rural communities where majority of the population resides (HERFON, 2006). In recent times, however, there have been renewed interest of the residents of urban communities as a result of the pronouncements on radio and TV by AM-Therapist with claims that their ‘wares’ can cure all diseases ever known to mankind. This may be the reason why this study found out that majority of the respondents got their information on alternative medical therapy from the radio. This is because of high level of uncontrolled radio coverage and advert of ATM. Side effects of AMT known to respondents include diarrhoea (69.7%); abdominal pain (42.2%); vomiting (40.2%); skin reaction and others 16.6% and 5.7% respectively. These findings corroborate the findings by Krunkel and Spoerke (1984) and Marwick (1995). Respondents also acknowledged that AMT could result in fainting (47.0%); cause death (27.5%); cause injury to kidney (19.0%) or liver disease (8.6%). D’Arcy (1991) and Saxe (1987) reported renal failure and pulmonary disease in their various studies. In his study, Alonge et al. (2004) reported preventable complications from traditional bone setting practices. Notwithstanding their knowledge of side effects and injuries from AMT, more than a third 35.7% of the respondents prefers it to orthodox medicine. Even more than a quarter 28.7% would advise a sick person to seek AMT care first before orthodox therapy. This may be because alternative medicine is intricately interwoven with the culture of the respondents – a socio-economic and socio-cultural heritage as described by Elujoba et al. (2005). The main reason for the preference by this group of respondents is because it is cheap 21.4%. An earlier study in Nigeria by Osujih (1993) also reported that in developing countries where in addition to the dearth of orthodox medical services, institutions and personnel, AMT is cheaper, socio-culturally accessible and acceptable. It has also been documented by Sofowora (1982) that a large percentage of the world continues to depend on‘primitive’ herbal remedies because they are cheaper and easily accessible. As documented in the work of Barnes et al. (2004), this is unlike in the US where the National Centre for Complementary and Alternative Medicine found that the commonest reason for use of AMT by Americans was that they believe ALT would improve health when used in combination with conventional medical treatments. More than half (54.6%) of the respondents who are aware of AMT had patronized it in the last 12 months prior to this study. This agrees with the findings in a USA study where the use of alternative or complementary therapies by the US population appears to be substantial. It was reported that in 1990 such therapies were used in an estimated 34% of the population, increasing to 42% in 1997. The report of Stephen et al. (2003) noted that more visits were made to alternative medical practitioners than to all the primary care physicians in those years. Another US study by Afari et al. (2000) on the use of alternative treatment by chronic fatigue syndrome (CFS) discordant twins showed that 91% of the twins had used at least one alternative treatment in their lifetime and the study concluded that individuals with CFS frequently use alternative medical treatments yet rarely communicated this use to their medical doctor. A study in South Africa by Rolanda van der Kooi et al. (2006) stressed the need to develop strategies that promote open dialogue between health providers and communities on the use of traditional medicine. Of those that have patronized alternative medical therapists in this study, 80.5% have used concoctions (herbal remedies) especially from hawkers. This agrees with Elujoba et al. (2005) that over 80% of Africans use herbal medicine. Other forms of AMT used by this group of respondents include herbalist homes/remedies 21.4% and traditional bone settings (7.2%) among others. This is not surprising as it has been documented in the proceedings of the WHO working group meeting on Integration of Traditional and Complementary/Alternative Medicine into National Health System (WHO, 2006) that within African Region of the WHO as a whole, over 80% of the population use traditional medicines for their primary health care needs. Also according to the Nigerian Traditional Medicine Policy in the Nigerian Health Review (HEBRON, 2006), traditional medicine is recognized as part of the health culture o Nigeria. Findings in a survey by Oladunni et al. (2005) of treatment practices for febrile illness in the Nigerian middle belt zone strengthen the need to recognize the traditional health practitioners in the treatment of health problems especially febrile illnesses and to establish quality control mechanism in partnership with them to improve their treatment practices. Conclusion This study has revealed that the use of alternative medical therapies is quite popular among the studied population and a large proportion of the respondents not only prefer but also use AMT notwithstanding that they live in the urban communities with better access to orthodox medical care and medical practitioners. Since safety and efficacy of these remedies remain largely unknown and untested to have met the ‘gold standard’ therapy, advising patients and the general public who use or seek alternative medical therapy presents a professional challenge. This notwithstanding, it is recommended that health practitioners must always explain and health educate the patients and the public at large of the need to seek orthodox medical therapy first. Also it is time that government should regulate the activities of the alternative medical therapists/practitioners and finds a way of fully integrating their practices into the orthodox and modern medicine. Regulations should be made concerning the advertisement of alternative medicine and practices since appropriate diagnosis were usually not made for the use of these drugs and respondents were usually not aware of dosage requirements. Acknowledgement The authors would like to express their sincere gratitude to all the people (students; the respondents and the senior colleagues who read through the manuscripts and gave valuable suggestions and references) who have contributed to making this study possible. References
© Copyright 2009 - African. Journal. Traditional, Complementary and Alternative Medicines The following images related to this document are available:Photo images[tc09038t4.jpg] [tc09038t3.jpg] [tc09038t2.jpg] [tc09038t1.jpg] [tc09038t5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}