 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Traditional, Complementary and Alternative Medicines, Vol. 6, No. 4, 2009, pp. 494-517 Review Paper TREATING GYNAECOLOGICAL DISORDERS WITH TRADITIONAL CHINESE MEDICINE: A REVIEW Jue ZHOU1 and Fan QU2 * 1The Centre for Natural Medicines Research, King’s College London, Franklin-Wilkins Building, 150
Stamford Street, London, UK., Code Number: tc09039 Abstract Traditional Chinese Medicine (TCM) has significant advantages in treating gynaecological disorders. The paper has provided a brief introduction on the current progress of treating some gynaecological disorders including endometriosis, infertility, dysmenorrhea, abnormal uterine bleeding, premenstrual syndrome, menopausal syndrome, uterine fibroids, chronic pelvic inflammation, polycystic ovarian syndrome (PCOS), cervicitis and vaginitis with Chinese Herbal Medicine (CHM) and acupuncture. The use of TCM in the field of assisted reproductive techniques (ART) has also been included in the review. In addition, thirty-two commonly used Chinese medicinal formulas in treating gynaecological disorders have been introduced. Key words: Traditional Chinese Medicine (TCM); Chinese Herbal Medicine (CHM); acupuncture; gynaecological disorders; review. Abbreviations: TCM: Traditional Chinese medicine; CHM: Chinese herbal medicine; PCOS: Polycystic ovarian syndrome; MOD: Mean optic density; VEGF: Vascular endothelial growth factor; MMP-9: Matrix metalloproteinase-9; POF: Premature ovarian failure; ER: Estrogen receptor; PMS: Premenstrual syndrome; WHI: Women's heath initiative; HRT: Hormone replacement therapy; BMD: Bone mineral density; LDL-C: Low-density lipoprotein cholesterol; TRAP: Tartrate-resistant acid phosphatase; ART: Assisted reproductive techniques; IVF: In vitro fertilization; ET: Embryo transfer; ICSI: Intra-cytoplasmic sperm injection; LIF: Leukemia-inhibitory factor; BMI: Body-mass index; SHBG: Sex hormone hiding globulin; OHSS: Ovarian hyperstimulating syndrome; Uu: Ureaplasma urealyticum; RT-PCR: Reverse transcription polymerase chain reaction; FSH: Follicle stimulating hormone; LH: Luteinizing hormone; E2: Estradiol. Introduction Traditional Chinese Medicine (TCM) includes a series of traditional medical practices originating in China . It is considered as a complementary or alternative medical system in most of the western countries while remaining as a form of primary care throughout most of Asian countries. TCM is a comprehensive system for the assessment and treatment of acute and chronic disorders, as well as for the preventative health care and maintenance. TCM theory is extremely complex and originated thousands of years ago through meticulous observation of nature, the cosmos, and the human body. The major theories of TCM include the Yin-yang , the Five Elements , Qi and Blood, and Zang-fu organ theories. In TCM, the understanding of the human body is based on the holistic understanding of the universe as described in Daoism, and the treatment of illness is based primarily on the diagnosis and differentiation of syndromes. The clinical diagnosis and treatment in TCM are mainly based on the Yin-yang , the Five Elements and Zang-fu organ theories. These theories apply the phenomena and laws of nature to the study of the physiological activities and pathological changes of the human body. The typical TCM therapies include Chinese Herbal Medicine (CHM) and acupuncture. CHM acts on Zang-fu organs internally, and acupuncture is accomplished by stimulating certain areas of the external body. TCM has significant advantages in treating gynaecological disorders. As early as in 1237 A.D., the first book devoted solely to gynaecology and obstetrics of Chinese Medicine, The Complete Book of Effective Prescriptions for Diseases of Women, was published. CHM and acupuncture usually led to satisfactory curative effects in treating some gynaecological disorders such as endometriosis, infertility, dysmenorrhea, abnormal uterine bleeding, premenstrual syndrome, menopausal syndrome, uterine fibroids and chronic pelvic inflammation, polycystic ovarian syndrome (PCOS), cervicitis and vaginitis. This review will provide a brief introduction on the current progress of treating these gynaecological disorders with CHM and acupuncture. In addition, thirty-two commonly used Chinese medicinal formulas in treating gynaecological disorders have also been introduced. Endometriosis Endometriosis, defined by the presence of viable endometrial tissue outside the uterine cavity, is among the most common gynaecologic disorders affecting women of reproductive age. According to the theory of TCM, the etiology of endometriosis is Blood stasis. Blood stasis causes a Fire syndrome and the accumulation of Damp-heat in the lower part of the body (“Lower Jiao”). As most of the patients with endometriosis suffer from the symptoms of pelvic inflammation, the accumulation of Heat and Blood stasis are the main pathologic changes. Although the pathogenic factors and pathogenesis are complex, the keys are Dampness, Heat, and Stasis. CHM and acupuncture have gained satisfactory curative effects in treating endometriosis. In one clinical research, a Chinese medicinal formula with Radix ec Rhizoma Rhei as the main ingredient was used to treat 76 patients with endometriosis, and the total effective rate was 80.26% (Wang et al., 1991). Another clinical research, with removing Blood stasis, resolving Phlegm, softening and resolving the Lump as the therapeutic principles, successfully treated 46 endometriosis patients with a total effective rate of 91.3% (Liu, 1994). Ketong Decoction, with Radix codonopsitis pilosulae , Radix paeoniae rubra and Rhizoma ligusticum wallichii as the main herbs (ingredients), respectively obtained a curative rate of 81.0%, 75.9% and 58.3% in treating endometriosis patients of I, II, and III stages, all higher than those of the controls (Yu, 1998). Neiyixiao Recipe (including Rhizoma sparganii, Rhizoma curcumae, Hirudo, Eupolyphaga sinensis walker, Squama manitis, Semen cuscutae, Herba epimedii, etc) has also been found to be effective in treating endometriosis by tonifying Kidney and removing Blood stasis (Liu et al., 1998). NYF (consisting of Radix ec rhizoma rhei, Semen persicae, Ramulus cinnarnomi, Rhizoma sparganii, Spica prunellae and Carapax et Plastrum testudinis) has been found to have good clinical effects in treating endometriosis., which had significantly decreased the prostaglandin F 1α (PGF1α) levels and increased the 6-keto- PGF1α/ thromboxane B 2 (TXB2) ratio and the level of β-endorphin in the patients (Yu et al., 2003). Yushi Neiyi Fang, consisting of Radix Astragali, Pollen Typhae, Semen Persicae, Hirude Nipponica Whitman and Herba epimedii gained a total effective rate of 91.67% in treating 36 patients with endometriosis (Song et al., 2005). A study with the purpose to observe the clinical efficacy of Quyu Jiedu Recipe, which consisted of Caulis sargentodoxae, Flos rosae rugosae, Flos lonicerae, Fructus forsythiae, Radix salviae miltiorrhizae, Radix paeoniae rubra, Cortex moutan, in treating endometriosis, and to explore the changes of the levels of vascular endothelial growth factor (VEGF) and cell proliferative nucleoprotein antigen (Ki-67) before and after treatment, showed that before treatment, the VEGF and Ki-67 expression positive rates and their mean optic density (MOD) were higher in patients than in healthy women, while, after treatment, the positive rate and MOD of VEGF expression significantly lowered, but those of Ki-67 changed insignificantly, and the comparison between the two treatment groups showed no significant difference (Lian et al., 2007). For those patients with post-operational relapsed endometriosis, Chinese medicinal herbs have also gained satisfactory curative effects. Zhu treated 31 patients of post-operational relapsed endometriosis with integrated TCM and Western medicine and gained a total effective rate of 90.32%, in which, Radix salviae miltiorrhizae, Cortex moutan, Radix paeoniae rubra, Pollen typhae and Semen persicae, Hirudo were used as the main herbs (Zhu, 1998). Another research aiming to observe the clinical efficacy and safety of Yiweining (YWN, a Chinese medicinal formula, consisted of Radix angelicae sinensis, Rhizoma corydalis, Rhizoma curcumae, Semen persicae, Radix paeoniae rubra, Flos carthami, Radix salviae miltiorrhizae, Carapax et Plastrum testudinis ) and gestrinone (GT) in treating post-operational patients of stage III endometriosis found that the recurrence rate in the YWN group and the GT group were 5.0% and 5.3% respectively, showing insignificant difference between the two groups and the adverse reaction rate in the YWN group was lower than that in the GT group, which concluded that the application of YWN to prevent the post-operational recurrence of endometriosis was effective and safe, and its efficacy was similar to that of GT (Yang et al., 2006). Another research was also conducted to investigate the effects and the mechanism of E-leng Capsule (consisting of Rhizoma sparganii, Rhizoma curcumae, Radix paeoniae rubra and Radix salviae miltiorrhizae) in preventing and treating post-operation recurrence of ovarian endometriotic cysts (Cao et al., 2008). The 12-month follow-up showed that recurrence presented in 1 patient in the treatment group (3.3%), and 6 in the control group (20.0%), showing significant difference between them and the expressions of tissue inhibitor of metalloproteinase-1 (TIMP-1) mRNA in eutopic and ectopic endometrium were both higher in the treatment group than the control group, while the expressions of matrix metalloproteinase-9 (MMP-9) mRNA were lower, indicating that E-leng Capsule can reduce the invasive ability of endometrium tissue probably by regulating the balance of MMP/TIMP, namely, increase the expression of eutopic and ectopic endometrial TIMP-1 and decrease the expression of ectopic endometrial MMP-9, and thus achieve its preventive and therapeutic effects on the recurrence (Cao et al., 2008). Some animal experiments have ever been conducted to explore the mechanism of Chinese herbs and acupuncture in treating endometriosis. Two researches were conducted to explore the effects of Yiweining (YWN, a Chinese medicinal formula, consisting of Radixp paeoniae rubra, Rhizoma curcumae, Rhizoma corydalis, Radix scutellariae, Semen coicis, etc.) on the cytokines and the expressions of metalloproteinase-2 (MMP-2) and cyclooxygenase-2 (COX-2) mRNA of the model rats with endometriosis (Qu et al., 2005; Qu et al., 2006). Their results showed that the contents of tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6), and interleukin-8 (IL-8) in the peripheral blood of the model group were apparently higher than the false-operation group, and YWN had reduced the amount of TNF-α, IL-6, and IL-8 in the serums of the model group's rats, which concluded that YWN could prevent the growth of ectopic endometrium by inhibiting the synthesis and secretion of TNF-α, IL-6, and IL-8 (Qu et al., 2005). There were also significant differences in the expressions of MMP-2 and COX-2 mRNAs between the untreated group and the high-dose YWN-treated group (Qu et al., 2006). In the prescription of YWN, Radix paeoniae rubra is the main herb to resolve dampness, remove blood stasis, and reduce Fire, which adapts to the pathogenesis of endometriosis. Rhizoma curcumae could remove blood stasis, promote flow of Qi, soften solid masses and relieve pain, promote the circulation of the efficient components of the drugs in Blood. All these herbs, used together, play a role of promoting the circulation of blood and removing blood stasis and act as monarch herbs. Rhizoma corydalis can promote the flowing of Qi and relieve pain in order to increase the function of promoting the circulation of blood and removing blood stasis. Radix scutellariae and Semen coicis in the prescription function together to reduce Fire and resolve dampness (Qu et al., 2005; Qu et al., 2006). Acupuncture also has good curative effects in treating endometriosis. Acupuncture at Xuehai (SP-10) and Sanyinjiao (SP-6) acupoints were found to have a better therapeutic effect on the model rats with endometriosis, which could down-regulate the abnormal increase of MMP-2 levels to inhibit the invasion of ectopic tissue to extracellular matrix, thus reducing the ectopic tissues (Chen et al., 2008). In a clinical research to compare the therapeutic effects of the combined use of Shu-Mu acupoints, routine needling method and Western medicine treatment on the patients with endometriosis, the researchers found that the total effective rates were similar in the three groups and the Shu-Mu acupoints combination group was superior to other two groups in improvement of dysmenorrhea, irregular menstuation, lumbago and sacrodynia, anus engorge, moreover, the serum CA125 levels in the Shu-Mu acupoints combination group were significantly decreased (Sun and Chen, 2006). Endometriosis is a common cause of pelvic pain in women, which has a negative influence on the ability to work, on family relationships and sense of worth. Acupuncture may be used as an adjunct in treating endometriosis pain (Lundeberg and Lund, 2008). In a case report, two adolescent girls with endometriosisrelated chronic pelvic pain of more than 1 year experienced modest improvement in pain as measured by oral self-reports of pain on a scale from 1 to 10, as well as self or family-reported improvement in headaches, nausea and fatigue after undergoing between 9 and 15 treatments over a 7- to 12-week period and no adverse effects were reported, which provided a preliminary evidence that acupuncture may be an acceptable and safe adjunct treatment for some adolescents with endometriosis-related pelvic pain refractory to standard anti-endometriosis therapies (Highfield et al., 2006). Ear acupuncture therapy has also demonstrated satisfactory curative effects in treating 37 cases of dysmenorrhea due to endometriosis in a clinical research (Xiang et al., 2002). At present, a randomized controlled trial is being conducted to test the hypothesis that TCM (acupuncture and CHM) reduce endometriosis-related pelvic pain as effectively as nafarelin therapy without causing the pseudo-menopausal side effects that accompany gonadotropin-releasing hormone-α (GnRH-α) therapy in Women’s Health Research Unit of the Oregon Health Sciences University and the Oregon College of Oriental Medicine, U.S.A. In the study, women were randomly assigned to receive either 12 weekly treatments of TCM or 12 weeks of the FDA-approved GnRH-α treatment. The protocol (NCT00034047) is funded by the National Center for CAM (NCCAM). This will likely prove to be a landmark study in alternative endometriosis therapy. A great number of clinical researches as well as animal experiments have demonstrated the eminent efficacy of CHM and acupuncture in treating endometriosis. However, large-scale, multi-centre, randomized, double-blind and placebo-controlled clinical researches should be conducted in the future and a standard therapy of TCM should be established. Infertility TCM has a long history in treating infertility. The earliest records of treating infertility with TCM can be dated back to 200 A.D. in the famous medical classics, Treatise on Febrile Diseases . According to the theories of TCM, infertility can be the result of several types of syndromes. It can be caused by a deficiency in the kidney and liver organs, which disrupts the endocrine system. This creates an imbalance of hormones in the body, making sexual reproduction impossible. Infertility can also be the result of stagnant Qi (energy) and Blood; this lack of circulation stymies sexual reproduction even though hormone levels are normal. Blood stagnation is commonly found in women’s bodies as endometriosis, which can also be treated through the use of acupuncture and CHM. Finally, a Damp-heat syndrome can cause infertility that makes internal systems function improperly. The presence of a Damp-heat syndrome is much like inflammation and it causes blockage that must be relieved for sexual reproduction to be possible. With all of these types of infertility diagnoses, TCM provides a variety of treatment options. In modern China, TCM is used to treat infertility in both men and women. Although no individual Chinese herb is considered especially useful for promoting fertility, more than 100 different herbs, usually given in complex formulas comprising of 12 or more ingredients, are used in the treatment of infertility with the purpose of correcting a functional or organic problem that caused infertility. The design of the formulas has varied somewhat over the centuries, based on the prevailing theories and available resources. Individual TCM practitioners have a preference for particular herbs, thus accounting for some of the variations among formulas that are recommended. Herbs can be administered as pills, powders, tablets, or decoctions (teas). All methods of administration can be effective. Chinese clinicians appear confident that most fertility problems can be overcom solely or primarily with the use of CHM and acupuncture. Although most medical books describing Chinese methods of treating infertility do not mention acupuncture, acupuncture therapy may address particular symptoms of concern either directly related or unrelated to infertility, and might be influential in speeding up the development of normal fertility. In the event that infertility is mainly due to the functional disorders, it is possible that acupuncture alone could resolve the problem. A recent review giving an overview of the potential use of TCM in the treatment of infertility, including an evidence-based evaluation of its efficacy and tolerance, showed that the growing popularity of TCM used alone or in combination with Western medicine highlights the need to examine the pros and cons of both Western and TCM approaches. Integrating the principle and knowledge from well characterized TCM and Western medical approaches should become a trend in existing clinical practices and serve as a better methodology for treating infertility (Huang and Chen, 2008). Recent studies demonstrated that TCM could regulate the gonadotropin-releasing hormone (GnRH) to induce ovulation and improve the uterus blood flow and menstrual changes of endometrium (Huang and Chen, 2008). In addition, it also has impacts on patients with infertility resulting from PCOS, anxiety, stress and immunological disorders (Huang and Chen, 2008). One Chinese medicinal formula (consisting of Semen cuscutae, Radix dipsaci, Radix polygoni Radix Polygoni Multiflori Preparata, Fructus lycii, Herba lycopi, Herba leonuri, Radix angelicae sinensis, Radix paeoniae rubra, Rhizoma cyperi, etc), when combined with Western medicine, gained a total effective rate of 81.25% in treating 64 patients with anovular infertility (Yan et al., 2003). The combined therapy of CHM and compound cyproterone acetate can significantly relieve the clinical symptoms, improve the abnormal blood level of sex hormones and significantly elevate the pregnancy rate of the patients of non-obesity PCOS, in which, Guishao Dihuang Decoction (consisting of Radix rehmanniae, Fructus corni, Rhizoma dioscoreae, Cortex lycii, Cortex moutan, Poria, Radix dipsaci, Semen cuscutae, Radix angelicae sinensis and Radix Achyranthis bidentatae), Cupailuan Decoction (consisting of Radix angelicae sinensis, Radix paeoniae rubra, etc), Yulinzhu Decoction (consisting of Semen cuscutae, Cortex Eucommiae, Placenta Hominis, Cornu Cervi Degelatinatum, Radix Rehmanniae), Shixiao San (consisting of Pollen typhae, Rhizoma cyperi, Radix linderae, Herba lycopi, Radix Rubiae, Herba Leonuri, Fructus Crataegi, Radix Polygoni, Radix Polygoni Multiflori Preparata, Radix dipsaci, Semen cuscutae) and Cangfu Daotan Wan (consisting of Herba epimedii, Radix rehmanniae, Rhizoma dioscoreae Fructus corni, Cortex moutan, Sclerotium poriae Cocos Rhizoma alismatis, Cortex eucommiae, Semen cuscutae, Rhizoma cyperi, etc) were used, respectively (Tao et al., 2003).Yangjing Zhongyu Decoction (YZD) has been found to sooth the Liver and nourish the kidney, and promote MMP-9 gene expression in endometrium to benefit the degradation of extracellular matrix of endometrium, and facilitate blastocyst implantation (Wu and Zhou, 2004). In another clinical research exploring the effects of Nuzhen Yunyu Decoction (NYD, a Chinese recipe for nourishing blood and reinforcing the kidney) on the hemodynamic parameters in ovarian and uterine arteries, 68 patients were randomly divided into two groups at the ratio of 2:1, 45 in the TCM group were treated with Chinese medicine and 23 in the control group treated with clomiphene citrate and the results showed that the ovulation promoting rate, pregnancy rate and abortion rate in the two groups were similar, but the treated group showed better effects than that of control group in such aspects as regulating menstruation, promoting growth and development of follicle, strengthening endometrium, improving blood supply and circulation of uterine and ovary (Xia et al., 2004). A Chinese medicinal formula-Xiaokang Wan (consisting of Radix salviae miltiorrhizae, Flos carthami, Radix angelicae sinensis, Radix scutellariae, Radix astragali, Rhizoma anemarrhenae, Sclerotium poriae Cocos etc.), when used together with dexamethasone, vitamin E and vitamin C, can reduce or eliminate the influence of antibodies in the serum of patients on pregnancy, thus reaching the goal of curing infertility, in which 2,062 cases were periodically treated for 2 periods as a course of treatment and at the end of a treatment period, the rate for the antibodies to turn negative reached over 85% and the average pregnant rate reached 36.66% (Du et al., 2005). In addition, two case reports have also demonstrated the satisfactory curative effects of Chinese herbs in treating female infertility (Chao et al., 2003; Qu et al., 2007). In the first report, the patient with premature ovarian failure (POF) and secondary amenorrhea for 8 years presented ovulation after the administration of Chinese herbs for 3 months (Chao et al., 2003). In the case, TCM concentrated herbal extracts of Radix rehmanniae, Rhizoma dioscoreae, Fructus lycii, Fructus corni, Radix cyathulae, Semen cuscutae, Cornu cervi pantotrichum, Carapax et Plastrum testudinis, Herba epimedii and Radix morindae officinalis were prescribed, which were a modification of a famous Chinese medicinal formula - Zuo Gui Wan. When the patient discontinued the CHM treatment and tried therapy with clomiphene citrate, neither ovulation nor conception occurred. Eight months after beginning clomiphene citrate therapy, the concentrations of follicle stimulating hormone (FSH) and luteinizing hormone (LH) were still in the postmenopausal range. The modified formula of Zuo Gui Wan was prescribed again and the patient conceived 1 month after taking the formula. The case suggested that CHM restored ovarian function effectively and promptly, and offered another option for treating infertility in patients with POF (Chao et al., 2003). In the second report, a patient who suffered from secondary amenorrhea for 6 years and primary infertility for 2 years due to pituitary atrophy was successfully cured with Chinese herbs. After orally administered Chinese herbs (Radix rehmanniae, Radix astragali, Radix angelicae Sinensis, Radix Codonopsis Pilosulae, Rhizoma Dioscorea, Fructus Corni, Semen cuscutae, Fructus Rubi, Radix dipsaci, Rhizoma cyperi, Radix salviae miltiorrhizae, Cortex cinnamomi, Fructus psoraleae, Fructus ligustri lucidi, Herba leonuri) for 1 month, the patient menstruated once and became pregnant later (Zhou and Qu, 2007). Bushen Yugong Granule (consisting of Radix rehmannia, Semen cuscutae, Cortex eucommia, Fluoritum, Fructus corni, Placenta hominis, Cornu cervi pantotrichum, Radix salviae miltiorrhizae, etc.) were also found to have an estrogen-like activity, which could increase the endometrial content of estrogen receptor(ER), enhance the effect of estrogen on uterus and promote the uterine development, so as to elevate the fertilization rate (Qian et al., 1998). The effect of Chinese herbs in treating infertility has also been demonstrated in model animals. In an experiment study, after the sex gland axis and adrenal gland of female SD rats of 9 days old were disturbed with exogenous androgen, Chinese herbs (including Radix aconiti Lateralis preparata, Cortex cinnamomi, Herba epimedii, Semen cuscutae, Rhizoma polygonati, Fructus psoraleae and Radix rehmanniae) were orally administered and the results showed that these herbs could reduce androgen levels and induce ovulation through regulating sex gland axis and adrenal gland in multi-levels and multi-target organs (Gui et al. 1998). Auricular acupuncture also seems to offer a valuable alternative therapy for female infertility due to hormone disorders (Gerhard and Postneek, 1992). Following a complete gynecologic--endocrinologic workup, 45 infertile women suffering from oligoamenorrhea (n=27) or luteal insufficiency (n=18) were treated with auricular acupuncture, and the results were compared to those of 45 women who received hormone treatment. Women treated with acupuncture had 22 pregnancies, 11 after acupuncture, 4 spontaneously, and 7 after appropriate medication. Women treated with hormones had 20 pregnancies, 5 spontaneously, and 15 in response to therapy. Four women of each group had abortions (Gerhard and Postneek, 1992). Although CHM and acupuncture have been found to have significant advantages in treating infertility, lack of standard animal models and lack of large-scale, multi-centre, randomized, double-blind and placebocontrolled clinical researches have limited the practices of treating infertility with TCM. Further researches should be conducted to address the issues. Dysmenorrhea In TCM, the specific details of the menstrual cycle (duration, volume, appearance of flow, etc) are only the surface phenomena. The underlying causes of menstrual disorders are the dysfunction of the internal organs; disharmony of Qi, Blood and Body Fluids; imbalance of the Ren and Du meridians; and the irregularity of Kidney Essence. In any type of menstrual disorder, blood is critical. For regulating the menstrual cycle, regulating Blood is always necessary. Radix angelicae sinensis, Radix paeoniae rubra and Radix rehmanniae can function to nourish the blood and regulate the menstrual cycle. Radix angelicae sinensis tops the list for gynaecological problems. The “female ginseng” can tonify the female reproductive system, relieve menstrual pain, regulate the menstrual cycle, reduce premenstrual syndrome and relieve many symptoms of menopause. The following three patterns of menstrual disorders are very common and have been emphasized by Chinese medicine practitioners for hundreds of years. Disharmony of Liver, Spleen, and Kidneys: This pattern includes irregular periods and dysmenorrhea. Also indicated are potential profuse bleeding and amenorrhea. This pattern is always connected to emotions. Ding Jing Tang is the main prescription for this type of menstrual disorders. Ding Jing Tang consisted of Radix bupleuri chinensis, Herba schizonepetae, Radix angelicae sinensis, Radix paeoniae lactiflorae, Rhizoma dioscoreae, Rhizoma smilacis glabrae, Semen cuscutae, Radix rehmanniae preparata. This formula was prescribed by Dr. Fu Qingzhu in his famous book, Fu Qingzhu’s Gynecology, written in 1827. This is one of the most important gynaecological textbooks in TCM. His formulas are still the standard in the modern textbooks. In this formula, Radix bupleuri chinensis and Herba schizonepetae soothe the Liver, Rhizoma dioscoreae and Sclerotium poriae cocos strengthen the Spleen, Semen cuscutae and Radix rhmanniae tonify the kiney. All these herbs help Radix angelicae Sinensis and Radix peoniae rubra to “soften and comfort” the Liver, nourish the Blood and regulate the menstruation. It is a well-balanced formula. Excessive Heat Pattern: This pattern includes early periods, heavy menstruation, profuse bleeding, dysmenorrhea with symptoms such as anxiety, feverish feeling, dry mouth, purple clots in menses, breast distention, hypochondriac pain or abdominal distention. Qing Jing Tang is the main prescription for menstrual disorders of Excessive Heat Type. This formula was also prescribed by Dr. Fu Qingzhu in his Fu Qingzhu’s Gynecology. Excessive Cold Pattern: This pattern includes scanty periods (oligomennorrhea), delayed periods, amenorrhea, or dysmenorrhea. Main symptoms include Blood stasis with periods, cold limbs, abdominal pain with periods, and aversion to cold. Wen Jing Tang is the main prescription for menstrual disorders of the Cold Type. This formula was prescribed by Dr. Chen Ziming in his book, Fine Prescriptions for Women, written in 1237 during Song Dynasty. Dysmenorrhea is one of the most common menstrual disorders directly influencing a woman’s quality of life. Dysmenorrhea refers to lower abdominal pain or other discomforts before, during or after menstruation. If the dysmenorrhea starts from menarche, it is called primary dysmenorrhea (functional dysmenorrhea). The patients who suffered from the primary dysmenorrhea have no pathogenic changes in their genital organs. If the dysmenorrhea emerges after the occurrence of menarche, it is called secondary dysmenorrhea, which are often caused by endometriosis, adenomyosis, chronic pelvic inflammatory disease, pelvic tuberculosis, tumor, cervicitis, among which endometriosis is the most common one. As the patients who suffered from primary dysmenorrhea have no pathogenic changes in their genital organs, they can be cured by CHM and acupuncture. Dysmenorrhea was first documented in Synopsis of Prescriptions of the Golden Chamber by Zhongjing Zhang of Donghan Dynasty (A.D.196). According to TCM, primary dysmenorrhea is usually caused by emotional factors, invasion of six exogenous pathogenic factors and stagnation of Qi and Blood; or by retention of Blood in the Paogong due to Liver depression and Qi Stagnation resulting from emotional upsets; or by Colddampness attacking the Lower Jiao and lodging in the Paogong due to walking in water during menstruation or sitting on damp ground; or by constitutional Deficiency of Qi and Blood, or consumption of Qi and Blood due to serious diseases and prolonged illness. Acupuncture has a reliable therapeutic effect on primary dysmenorrhea, which is superior to that of Somiton tablet, and the mechanism might be exerted by regulating prostaglandin F2α (PGF2α) level in menstrual fluid (Lin et al., 2008). Acupuncture at such acupoints as Taixi(KI-3), Gongsun(SP-4), Zusanli(ST-36), Tianshu(ST-25), Guilai(ST-29), Qichong(ST-30), Guanyuan(CV-4) can be used to treat dysmenorrhea, especially to treat those subjects in whom oral contraceptives are contraindicated or refused (Iorno et al., 2008). Li, et al (Li et al., 2008) observed the therapeutic effect of acupuncture at Siguan points with Qinglong Baizei method on primary dysmenorrhea and to explore the mechanism. In the research, one hundred and eighty cases of primary dysmenorrhea were randomly divided into group A, group B and group C, 60 cases in each group. Group A were treated by acupuncture at Hegu (LI-4) and Taichong (LR-3) with Qinglong Baiwei method; group B were treated by routine acupuncture with Sanyinjiao (SP-6) and Ciliao (BL-32) as the main acupoints; and group C were treated by oral administration of Yueyueshu Decoction, a Chinese medicinal formula. The results showed that the curative rate and the total effective rate were 75.0% and 100.0% in group A, 60.0% and 95.0% in group B, and 25.0% and 90.0% in group C, respectively, group A and B being significantly better than group C. The analgesic effects within 30 min of treatment in both group A and group B were significantly better than that in group C, and that in group A was significantly better than that in group B. It is then concluded that acupuncture at Siguan points with Qinglong Baiwei method has a significant therapeutic effect on primary dysmenorrhea. In another clinical research to observe the therapeutic effects of acupuncture in treating primary dysmenorrhea combined with spinal Tuina, thirty cases of the treatment group were treated by acupuncture combined with spinal Tuina, and thirty cases in the control group were treated by routine acupuncture. The total effective rate was 93.3% in the treatment group, and 73.3% in the control group, with a significant difference between the two groups, indicating that acupuncture combined with spinal Tuina has good prospects for treatment of primary dysmenorrhea (Guo and Meng, 2008). A study evaluating the analgesic and therapeutic effects of electrosuperficial- acupuncture of Sanyinjiao (SP-6) for treating primary dysmenorrhea found that the analgesic effects of both electro-superficial-acupuncture and superficial-acupuncture at Sanyinjiao (SP-6) for primary dysmenorrhea patients were significantly better than that of oral administration of Brufen (Zhi, 2007). Acupuncture in patients with dysmenorrhea was found to be associated with improvements in pain and quality of life as compared to treatment with usual care alone and to be cost-effective within usual thresholds in a randomized study (Witt et al., 2008). The central modulating mechanism of acupuncture at Sanyinjiao (SP-6) in treatment of primary dysmenorrhea has been demonstrated in a study (Gong et al. 2006). Vitamin K acupuncture point injection, a dysmenorrhea treatment derived from TCM, has also been a standard treatment in some hospitals in China since the 1980s. A recent research showed that acupuncture point injection with vitamin K can alleviate acute menstrual pain, and the relief extended through the nontreatment follow-up cycles in an uncontrolled pilot study, which was conducted in two countries (Wang et al., 2004). Acupuncture at such acupoints as Baihui (DU-20), Hegu (LI-4), Zhongji (CV-3), Guanyuan (CV-4) and Qihai (CV-6) has also shown satisfactory curative effects in treating primary dysmenorrhea (Habek et al., 2003). Acupuncture can improve the dysmenorrhea symptom to a certain extent, and the mechanism is possibly related to regulative effects of acupuncture on the hormones-mediating receptors in mice (Yang and Huang, 2008). In the animal experiment, the adult mice with no pregnancy were randomly divided into a normal group, a model group, an acupuncture group and a medication group. The model group, the acupuncture group and the medication group were modeled by Diethylstilbestrol and Ocytocin. For the acupuncture group, at the 7th day of modeling, acupuncture was given at Sanyinjiao (SP-6), Diji (SP-8), once a day, for 5 days; and at the 7th day of modeling, Yimucao Gao 0.6 mg/g was given intra-gastrically to the medication group for 5 days. The stretching latent period and the number of stretching within 30 min were observed, and mRNA levels of ocytocin receptor and vasopressin receptor in the uterus tissue were detected with reverse transcription polymerase chain reaction (RT-PCR) method (Yang and Huang, 2008). As conventional treatment for primary dysmenorrhoea has a failure rate of 20% to 25% and may be contraindicated or not tolerated by some women, besides acupuncture, CHM may be another suitable alternative treatment. Tongjing powder, a Chinese medicinal formula, could improve the state of blood circulation and treat the dysmenorrhea effectively (Wu et al., 1998). A recent review found promising evidence supporting the use of CHM for primary dysmenorrhea; however, results are limited by the poor methodological quality of the included trials (Zhu et al., 2008). Although CHM and acupuncture have satisfactory curative effects in treating dysmenorrhea, especially the primary dysmenorrhea, most of the clinical researches are not large-scale, multicentre, randomized, doubleblind and placebo-controlled clinical ones, which should be addressed in the future. Abnormal uterine bleeding Abnormal uterine bleeding is usually caused by weak constitution, insufficiency of Kidney Qi, weakness of Chong and Ren meridians to control menstruation, or excessive sexual intercourse and multiparity that impair Kidney Qi. The syndrome should be differentiated according to the quantity, color and texture changes of the bleeding in light of the tongue and pulse conditions as well as the duration of disease. Besides, age is also an important factor to be taken into consideration. For example, the patients at puberty are usually due to insufficiency of Kidney Qi; the patients of childbearing age are frequently due to Liver Stagnation and Blood Heat, and the patients during perimenopausal period are often due to Deficiency of the Liver and Kidney or Deficiency of Spleen Qi. A study on the TCM syndrome factors of dysfunctional uterine bleeding based on cluster analysis and factor analysis showed that one hundred and thirty types of symptom were found in 1000 patients with dysfunctional uterine bleeding and the cardinal symptoms with comparative high frequency of occurrence (>35%) were as follows: coagulated blood, long menstruationis (more than 14 days), big menstrual blood volume, dark red blood, dripping-wet blood and bright red blood (Jin and Ma, 2008). The slow decrease of serum nitric oxide (NO) and plasma cyclic guanosine monophosphate (cGMP) levels was found to be closely related to prolonged bleeding after medical abortion, and Gong-Fu mixture, a Chinese medicinal formula is effective in the prevention and treatment of the prolonged bleeding (Liao et al., 1999). Yaoliuan Capsule (YLAC) has significantly decreased the time of vaginal bleeding after abortion inducing compared with the controls (Jin and Zhang, 2000). The difference between the two groups in menstrual cycle and menstrual period recovery after abortion was also significant. YLAC consisted of Radix angelica sinensis, Rhizoma ligusticum wallichii, Semen persicae, Flos carthami, Radix notoginseng, Colla corii asini, pollen typhae, Radix astragalus, Herba leonuri, Radix rubiae, Radix scutellaria, Radix glycyrrhiza, Rhizoma zingiber and Ophicalcitum. ChanLe Chongji, another Chinese medicinal formula has also been demonstrated to be effective for reducing bleeding after abortion (Zhao et al., 1999). Due to the features of acute attack, few large-scale, multicentre, randomized, double-blind and placebocontrolled clinical researches has been conducted to explore the effects of TCM in treating the disease. An appropriate animal model needs to be established. Premenstrual syndrome Premenstrual syndrome (PMS) refers to a collection of cyclical physical and/or psychologic symptoms that appear during the late luteal phase of the menstrual cycle. This syndrome is usually caused by Liver depression and Qi Stagnation leading to transformation of Fire and disturbing cardiac spirit; or by invasion of Liver Qi into the Spleen and Stomach; or by constitutional Yin asthenia; or by constitutional asthenia of the Spleen and Kidney. It is clear that this syndrome is mainly caused by dysfunction of the Liver and is related to the Heart, Spleen and Kidney. According to the clinical symptoms, this syndrome pertains to the conceptions of headache during menstruation, fever during menstruation, body pain during menstruation, edema during menstruation, diarrhea during menstruation, dizziness during menstruation, abnormal emotional changes during menstruation and distending pain in breasts during menstruation in TCM, generally known as symptoms before and after menstruation. In classical Chinese medical records, the earliest discussion of premenstrual and menstrual symptoms dates back to the Ming Dynasty (1368-1644 AD). In The Appendix of Dan-Xi’s Experiential Methods , Fang advised that to diagnose cases of feverish sensation in women’s diseases, one should ascertain whether it occurred during menstruation or also at other times. In Ye Tianshi’s Gynaecological Records , up to 22 premenstrual symptoms were recorded, such as edema, feverish sensation, pain in the hypochondrium, diarrhea, body aches, abdominal cramps, and reduced appetite. This syndrome is clinically divided into Excess and Deficiency types. The Deficiency type is marked by Kidney Deficiency and Spleen Deficiency. The Excess syndrome is marked by Qi Stagnation. The viscera involved are the Liver, the Spleen and the Kidney. Since clinical symptoms are complicated, clinical syndrome differentiation should be done in light of the time, location and nature of the symptoms as well as the conditions of the tongue and pulse. A study has been done to examine the effects of CHM for the treatment of PMS among Australian women within the theoretical framework of TCM, in which, sixty-one women were assigned randomly into two groups within different TCM patterns. There were significant differences after three months of treatment between CHM and placebo in premenstrual physical and psychological symptoms, depression, anxiety and anger, but with no difference in perceived stress, suggesting that the symptoms occurrence and severity of PMS can be effectively reduced by the use of CHM (Chou et al., 2008). One animal experiment has also been done to confirm the efficacy of Chinese herbs in treating PMS (Qiao et al., 2007). As rhesus monkeys (Macaca mulatta ) have a close phylogenetic relationship to humans, and have a similar 28-day menstrual cycle with similar hormonal fluctuations, in the study, the authors attempt to establish the premenstrual depression syndrome of rhesus monkey (M. mulatta) models by isolation with physical restraint of low social status young female monkeys during their luteal phase and the low social status young female rhesus monkeys (M. mulatta) were isolated with physical restraint during their luteal phase by using a specifically designed isolating-cage. During the entire menses cycle, serum levels of 5-hydroxytrypamine, noradrenalin and adrenalin were detected by capillary zone electrophoresis, and the changes in the serum levels of progesterone, estradiol (E2) and prolactin were investigated by radioimmunoassay. At the same time, the pharmaceutical interference effect of Jingqianshu Granule, a TCM formula specifically used to cure premenstrual depression patients, was tested using this premenstrual depression syndrome monkey model. The study showed that after being immured in two consecutive menstrual cycles, the monkeys presented depressive symptoms during the premenstrual phase of three consecutive menstrual cycles. The serum contents of the three kinds of monoamine neurotransmitters in depressive monkeys were significantly higher than the normal ones. The serum levels of progesterone and prolactin increased obviously, and a marked change in the pattern of progesterone secretion could be observed. Moreover, the premenstrual depressive symptoms of model group monkeys could not only be cured by Jingqianshu Granule, but the higher serum levels of prolactin and monoamine neurotransmitters in these monkeys could be reduced by this herbal medicine (Qiao et al.,2007). Besides CHM, there are more than 20 studies reporting the effects of acupuncture in the treatment of PMS. One study (You, 1997) classified the patients into one group with Yang Deficiency of the Spleen and the Kidney and another group with Stagnation of the Liver Qi. Taichong (LR-3), Taixi (KI-3), Qihai (CV-6), Ganshu (BL-18), Tanzhong (CV-17), and Sanyinjiao (SP-6) were used as the main acupoints in the first group and Zusanli (ST-36), Pishu (BL-20), Shenshu (BL-23), Taixi (KI-3), Sanyinjiao (SP-6) and Guanyuan (CV4) in another. Acupuncture in treating edema during menstruation was also reported effective in two studies (Li, 2002, Liu et al., 2002). The first study only used Fuliu (KI-7) as the point, and the second study used Zhongwan (CV- 12), Qihai (CV-6), Hegu (LI-4), Zusanli (ST-36), Sanyinjiao (SP-6) as the main points. Headache during menstruation could also be treated by acupuncture, one study (Zhang and Fu,2001) selected Fengchi (GB-20) as the main acupoint and another study (Sun, 1999) used Baihui (DU-20), Qihai (CV-6), Guanyuan (CV4), Sanyinjiao (SP-6), and Zusanli (ST-36) as the acupoints, in conjunction with Chinese herbs. These studies demonstrated that PMS symptoms may be alleviated by acupuncture or acupuncture in conjunction with other means (Beal, 1999). Large-scale, multicentre, randomized, double-blind and placebo-controlled clinical researches are needed to further demonstrate the efficacy of CHM and acupuncture in treating PMS. Moreover, cheap animal models of PMS should be established next. Menopausal syndrome Most women in their postmenopausal years may experience a variety of vasomotor and psychological symptoms such as hot flashes, night sweats, menstrual irregularities, vaginal dryness, depression, nervous tension, palpitations, headaches, insomnia, lack of energy, difficulty concentrating, and dizzy spells. Management of menopausal syndrome has received increased attention in recent years due to the growing interest in women’s health and the greater number of women entering the menopausal years. Although the current trend is to treat climacteric women with various forms of hormone replacement therapy (HRT), many women prefer not to or can not take HRT. In July 2002, a Women's Heath Initiative (WHI) clinical trial, designed to clarify the risks and benefits of combination HRT to the postmenopausal women, after an average follow-up of 5.2 years, found that a combination of estrogen and progestin frequently prescribed to postmenopausal women in U.S.A. increased the risk of invasive breast cancer, heart disease, stroke, and pulmonary embolism while reduced bone fractures and colorectal cancer. The overall risks of HRT outweigh the benefits, which provide an opportunity for TCM going to the world. A variety of clinical and experimental evidences have showed that TCM exerts quite satisfactory effects on relieving postmenopausal symptoms with little adverse effects (Chen and Yang, 2003). There is no corresponding name to menopausal syndrome in ancient books of TCM. The clinical manifestations are similar to those of hysteria, melancholia, vertigo, headache, palpitation, insomnia, et al. In light of the theory of TCM, menopausal syndrome is usually caused by the decline of Kidney Qi, near exhaustion of Tiangui, Deficiency of the Chong and Ren meridians or the insufficiency of Essence and Blood before and after menopause. In a famous ancient Chinese medical classics, Golden Mirror of Orthodox Medical Lineage·Essentials of Gynecopathy in Verse, it says, “Tiangui, the substance necessary for the promotion of growth, development and reproductive function of human body, is the source of menstruation. The congenital“Tiangui” comes from the parents, while the postnatal Essence and Blood result from the food stuff. When the girl is about 14 years old, the Chong and Ren meridians get ripe and menstruation occurs”. In another classic, Plain Questions on Preservation of Congenital Primary Qi of the Ancient People, it says, “When women are about 49 years old, the Chong meridian is failing in function, and menstruation ceases. At the same time, the constitution may gradually get weaker and the fertility ceases”. That is to say, when a woman is about 50 years in age, the Kidney Qi is insufficient. The Kidney Yin and Kidney Yang fall into an imbalance state and a series of clinical symptoms will appear. The principile of reinforcing the Kidney has been proven effective in treating menopausal syndrome (Wang and Wei, 2008). In a review, it was found that the practitioners of TCM who diagnose postmenopausal women with vasomotor symptoms are likely to make a diagnosis that includes Kidney Yin Deficiency (Zell et al., 2000). A pilot study comparing the clinical effects of Jia-Wey Shiau-Yau San (JWSYS), a traditional Chinese herbal prescription, and a continuous combined HRT in postmenopausal women with climacteric symptoms showed that JWSYS effectively alleviated most of the menopausal symptoms with no significant differences with the HRT, and JWSYS had a relatively lower discontinuation rate due to adverse effects, in particular the bleeding and breast tenderness (Chen and Yang, 2003). Zhengan Xifeng Decoction (consisting of Radix Achyranthis Bidentatae, Radix paeoniae rubra, Radix Asparagi, Radix Scrophulariae, Oyster, etc.) has showed good curative effects in treating menopausal syndrome (Li et al., 2003). A study designed to examine the effects of a Chinese herbal preparation-Dang Gui Buxue Tang (a 1:5 combination of Radix angelicae sinensis and Radix astragali) on menopausal symptoms in Hong Kong Chinese women showed that no significant difference between Dang Gui Buxue Tang and placebo in the treatment of vasomotor symptoms in Hong Kong Chinese women was found and the frequency of mild, moderate and severe hot flashes decreased in both treatment and placebo groups, but Dang Gui Buxue Tang was statistically superior to placebo in the treatment of mild hot flashes (Haines et al., 2008). Another study to determine whether a particular Chinese medicinal preparation is effective in alleviating menopausal symptoms found that the menopausal symptom score improved markedly after treatment with Chinese herbs and the scores remained at the same level at 6 months (Chan et al., 2006). A double-blind randomized placebo-controlled trial has also proved clearly that Chinese herbs could help women with their menopausal problems (Kwee et al., 2007). In the research, 31 peri- and postmenopausal Dutch women were recruited to complete 12 weeks of treatment with either Zhi Bai Di Huang Wan, HRT or placebo medications plus 4 weeks of non-treatment follow-up observation. Appropriate to the TCM setting, the CHMprescriptions could be adjusted according to the symptoms and signs of the individuals for that moment. The primary end-point was the reduction in frequency of vasomotor symptoms (hot flashes and night sweats). Secondary end-point was the improvements measured in quality of life questionnaire SF-36 and other symptoms and signs related to the peri- and postmenopausal period. The chosen trial methodology in the research, with its TCM differential diagnosis after orthodox medicine diagnosis, is fully compatible with TCM practice and hence acceptable for western and Chinese medical practitioners. Zhi Bai Di Huang Wan is composed of Rhizoma anemarrhenae, Cortex phellodendri, Radix rehmanniae praeparata, Fructus corni (Kwee, et al., 2007). A clinical research designed to explore the effects of a defined formula of Chinese medicinal herbs, Geng Nian An (consisting of Semen cuscutae, Fructus rubi, Radix angelicae sinensis, Radix paeoniae lactiflorae, Radix bupleuri chinensis, Fructus ligustri lucidi, Rhizoma dioscoreae, Ramulus cinnamomi, Oyster calcium, Radix codonopsis) in relieving menopausal symptoms in ovariectomized women showed that there existed significant differences between the TCM group and the controls in the total Kupperman scoring, MI of vaginal exfoliative cells, and the levels of FSH, LH, and E2 after treatment, indicating that Chinese herbs may be a useful alternative treatment for ovariectomized women suffering from menopausal symptoms, who are unable or do not want to receive HRT (Zhou et al., 2007). Soybean isoflavone was also found to effectively relieve the menopausal symptoms (Dai et al., 2004). Many experiments conducted on the ovariectomized animals have also demonstrated the efficacy of Chinese herbs in treating menopausal syndrome. An experiment conducted on the ovariectomized rats showed that a Chinese medicinal formula (composed of Radix rehmanniae, Rhizoma anemarrhenae, Carapax et plastrum testudinis, Fructus lycii, Herba epimedii, and Cortex phellodendri, etc) could increase the bone mineral density (BMD) and biomechanical parameters of the lumbar vertebrae and reduce the serum total cholesterol (TC) and low-density lipoprotein cholesterol (LDL-C) levels, yet produce no adverse reaction in stimulating proliferation and hypertrophy of uterus(Liu et al., 2006). The extracts of Chinese medicinal herbs were also found to have effects on estrogen deficiency bone loss in ten-month-old ovariectomized female rats, which may be a new approach in treating and preventing postmenopausal osteoporosis (Xu et al., 2003). Similarly, administration of Curculigo orchioides extracts were found to prevent bone loss in the trabecular bone of the tibia in ovariectomized rats without affecting the weight of the body and the uterus, increase serum phosphorus, calcium and osteoprotegerin levels, and decrease tartrate-resistant acid phosphatase (TRAP), and corticosterone levels, but did not alter serum TNF-α, IL-6, and alkaline phosphate levels in ovariectomized rats, indicating that Curculigo orchioides ethanol extract has a definite protective effect on bone loss in ovariectomized rats by inhibiting bone resorption and increasing serum phosphorus and calcium levels, without affecting bone formation(Cao et al., 2008). Radix Puerariae, the root of a wild creeper leguminous plant, contains a high amount of isoflavonoids such as daidzein and genistein, which are known to prevent bone loss induced by estrogen deficiency and Radix Puerariae has been found to prevent osteoporosis in ovariectomized mice, indicating Radix Puerariae may represent a potential alternative medicine for HRT in the prevention of osteoporosis in postmenopausal women (Wang, et al., 2003). In vivo, Shu-Gan-Liang-Xue (SGLX) decoction was found to have synergistic effects on tamoxifen, which can reduce serum hormone levels and alleviate the endometrial hypertrophy, the side effect of tamoxifen (Li et al., 2003). Besides CHM, the combined use of acupuncture and CHM and acupuncture alone were both found to be effective for treating menopausal syndrome (Tian and Zhang, 2008; Alfhaily and Ewies, 2008). Acupuncture was also found to result in a significant improvement in perimenopausal symptoms in women who have had an oophorectomy (Qu et al., 2007). Hot flashes are a significant problem in women going through the menopausal transition, which can substantially affect the quality of life. A recent research aiming to investigate the effects of acupuncture in decreasing hot flashes in peri- and postmenopausal women found that there was a significant decrease in mean frequency of hot flashes between weeks 1 and 8 across all of the usual care group, sham acupuncture group, and TCM acupuncture group, although the differences between the three study groups were not significant, however, the two acupuncture groups showed a significantly greater decrease than the usual care group(Avis et al., 2008). In a randomized clinical study, acupuncture was used for the relief of menopausal hot flashes, sleep disturbances, and mood changes (Cohen et al., 2003). Results from the experimental acupuncture treatment group showed a decrease in mean monthly hot flash severity for site-specific acupuncture. The control sham-acupuncture group had no significant change in severity from baseline over the treatment phase. Sleep disturbances in the experimental acupuncture treatment group declined over the study. Mood changes in both of the two groups showed a significant difference between the baseline and the third month of the study. Acupuncture using menopausal-specific sites holds promise for non-hormonal relief of hot flashes and sleep disturbances (Cohen et al., 2003). A pilot study to evaluate the safety and efficacy of acupuncture for the treatment of menopausal symptoms in tamoxifen-treated patients showed that anxiety, depression, somatic and vasomotor symptoms were improved by acupuncture, indicating that acupuncture seems to be safe and effective for the treatment of menopausal symptoms in women with previous breast cancer taking tamoxifen (Porzio et al.,2002).Acupuncture was shown to be effective in relieving vasomotor and physical disturbances of menopausal women, with the effects lasting at least up to 3 months after termination of the treatment, suggesting that acupuncture may be a useful alternative treatment for women who are unable or do not want to receive HRT (Dong et al., 2001). Although both animal experiments and clinical researches have demonstrated the efficacy of CHM and acupuncture in relieving menopausal syndrome, more researches need to be done to explore the mechanism of CHM and acupuncture in treating menopausal syndrome and an appropriate animal model that simulated the pathological condition of menopausal syndrome not only from the viewpoints of TCM, but also from the viewpoints of pathology should to be established next. Uterine fibroids Uterine fibroids are known by many names, including uterine myoma, leioma, fibroma, fibromyoma, or as hysteromyoma; these are equivalent designations for benign growths of smooth muscle tissue in the uterine wall. Clinically, only 10-20% of fibroid cases require surgery and interventions such as TCM may remove the need for surgery in some of these cases, especially if treated early. In TCM, uterine fibroid belongs to the category of “Zheng Xia”. Zheng Xia is defined as “masses in the uterus with a feeling of pain, swelling, or fullness, and with bleeding in severe cases.” The Yellow Emperor's Medicine Classic has recorded this disease in the third century BCE. All TCM gynaecology books address this condition in great detail as it has been treated by various schools of medicine over the last two thousand years. Three patterns of uterine fibroids are differentiated in TCM: Qi Stagnation and Blood stasis, Yin Deficiency and Empty-Fire Blazing, Liver Qi Stagnation and Spleen Deficiency. Some studies showed that Chinese herbal preparations might be able to relieve symptoms and shrink the volume of fibroids without significant adverse effects (Huang, 2003). Isoliquiritigenin (ISL), a calchone flavonoid, has cancer-preventing properties and is often used in TCM. ISL has been found to inhibit cell proliferation by initiating apoptosis in human uterine leiomyoma cells coupled with the increased cell cycle arrest, indicating that ISL could prove to be a promising chemo-preventive and therapeutic agent against human uterine leiomyoma (Kim et al., 2008). Herba scutellariae barbatae (Lamiaceae) (SB) is a perennial herb which is natively distributed throughout Korea and southern China. This herb is known in TCM as Ban-Zhi-Lian and traditional Korean medicine as Banjiryun, respectively. SB has been used as an anti-inflammatory and antitumor agent. A study was designed to determine the expression of cell cycle-related signal molecules for growth inhibition after HCG treatment by the herb SB in two different human myometrial smooth muscle cells (SMCs) and leiomyomal SMCs (Lee et al., 2004). They found although HCG/LH receptor was present in both cultured myometrial and leiomyomal cells, as assayed by RT-PCR analysis, treatment with HCG significantly increased cell proliferation in both myometrial and leiomyomal cells, however, SB reduced the proliferative effect of HCG in leiomyoma and myometrial cells, respectively. The final results suggested that SB reduced the HCG-promoted proliferation of myometrial and leiomyomal cells (Lee et al., 2004). The growth of uterine fibroids is regulated by the complex feedback loops between sex steroid hormones and growth factors (Langevin et al., 2002) and acupuncture has a regulative effect on the pituitary gland, the thyroid gland system, and the central nervous system, without presenting pharmacological interference or having a long-term effect. It may be legitimate to consider acupuncture as a potential therapy for uterine fibroids. There are many types of acupuncture (body, electro, scalp, elongated needle and fire needling) used to treat uterine fibroids in hospitals in China, with body acupuncture being the most commonly used technique (Lan and Li, 1997). However, few animal experiments have been conducted to investigate the mechanism of CHM and acupuncture in treating the disease. The treatment period and the follow-up phase in most of the clinical researches on treating uterine fibroids with TCM are not long enough, which should at least last for three to five years. ART and TCM As many couples try to conceive later in life, fertility difficulties are more prevalent. Assisted reproductive techniques (ART) have become very acceptable and popular. For some couples ART is the only hope to conceive. TCM will greatly improve the outcome of ART procedures. During trans-vaginal ultrasoundguided oocyte retrieval, the needle passes through the vaginal wall to puncture the follicles in the ovary. The procedures are generally short, lasting about 20 to 30 minutes, but can still be painful without adequate anesthesia or analgesia. Acupuncture has been found to be effective in relieving pain during the process. As early as in 1999, a study was designed to investigate the pain-relieving effect of acupuncture during transvaginal ultrasound-guided oocyte retrieval, in which, they randomized 150 patients to receive either acupuncture or conventional analgesia in addition to the paracervical block given to all patients and the results showed that acupuncture had comparable analgesic effect as conventional analgesia. (Stener-Victorin et al., 1999).However, in another two studies, significantly higher pain level was noted in the acupuncture group than in the conventional analgesia group (Humaidan and Stener-Victorin, 2004; Gejervall et al., 2005). A randomized double blind study of 94 in vitro fertilization (IVF) patients comparing the pain-relieving effects between auricular acupuncture with or without electric stimulation and the control groups without needles and without electric stimulation showed that auricular electro-acupuncture was significantly superior in reducing the pain levels during trans-vaginal ultrasound-guided oocyte retrieval to both auricular acupuncture alone and the control group (Sator-Katzenschlager et al., 2006). Two systematic reviews evaluated the analgesic effects of acupuncture during trans-vaginal ultrasound-guided oocyte retrieval, which showed that acupuncture can be recommended as one of the effective analgesic methods for patients who are unable to comply with the conventional analgesia because of adverse effects during and after trans-vaginal ultrasound-guided oocyte retrieval (Kwan et al., 2005; Stener-Victorin, 2005). Acupuncture can also improve IVF outcomes. Paulas et al. (Paulus et al., 2002) were the first to study the effect of acupuncture on the IVF outcomes, in which, acupuncture was administered on the day of embryo transfer (ET) in 160 patients selected randomly to the acupuncture and control groups. The acupuncture group received body acupuncture with manual stimulation and auricular acupuncture, whereas the control group received no acupuncture. The acupoints were selected according to TCM theories. Acupuncture was performed 25 minutes before and after ET, together with auricular acupuncture. Pregnancy rate was significantly higher in the acupuncture group than in the control group. The same authors (Paulus et al., 2003) presented in an abstract another randomized study using placebo needling in the controls. The acupoints used were the same as in the previous study (Paulus et al., 2002), but auricular acupuncture was no longer used. They found that the acupressure induced by the placebo needling in the placebo group resulted in a higher pregnancy rate when compared with the previous control group without any acupuncture treatment. Recently, three more randomized studies (Dieterle et al., 2006; Smith et al., 2006; Westergaard et al., 2006) on the effects of acupuncture on the IVF outcomes were published. Dieterle et al. (Dieterle et al., 2006) randomized 225 infertile patients into verum and sham acupuncture groups with different sets of acupoints. The study used an acupuncture protocol that was different from the one used in the study of Paulus et al (Paulus et al., 2002). Two sessions of acupuncture were given to patients, immediately after ET and 3 days later, together with auricular acupuncture at the same time. The study showed that the clinical and ongoing pregnancy rates of the verum acupuncture group were significantly higher than those of the control group. Smith et al. (Smith et al., 2006) performed a single-blind trial using retractable needles over placebo acupoints among 228 infertile patients. In addition to the two real or placebo acupuncture treatments immediately before and after ET, one additional session was given to patients on day 9 of ovarian stimulation. The acupuncture protocol before and after ET was similar to that of Paulus et al. (Paulus et al., 2002) with some minor modifications, but the details of acupuncture on day 9 of ovarian stimulation were not given. The pregnancy rates of the acupuncture and control groups were not statistically significant. In this study, the acupuncture settings in two groups were not identical. For example, the gauge of needles, the method of manual stimulation, and the locations of acupoints were different between the verum and the placebo groups. Acupuncture was performed by two different acupuncturists. In the study patients were randomized on the day of oocyte retrieval into one of three groups: to receive acupuncture on the day of ET (ACU 1), to receive acupuncture on the day of ET and again two days later (ACU 2), or to receive no acupuncture (control). According to the authors, the rationale for the ACU 2 group was to explore whether an additional acupuncture treatment closer to the time of implantation improves the quality of the endometrium due to a positive effect on uterine blood flow, which would further improve pregnancy and implantation rates. The study found that acupuncture given on the day of ET significantly improves the reproductive outcome of IVF/intracytoplasmic sperm injection (ICSI) patients (Westergaard et al., 2006), which was consistent with the findings of another study (Paulus et al., 2002). CHM has also been found to improve the outcomes of ART. A clinical research was to assess embryo implantation rate and pregnancy rate in women who received Bushen Wengong Decoction (BSWGD), a Chinese herbal formula, combined with low dose of human menopausal gonadotropin (hMG) prior to frozen-thawed embryo transfer (FET), which found that a programmed cycle of BSWGD combined with low dose of hMG could improve the embryo embryo implantation rate and pregnancy rate of FET (Zhang et al., 2006). Bushen Yiqi Hexue Recipe (consisting of Radix astragali, Radix angelicae sinensis, Herba taxilii, Radix ligustici chuanxiong, Radix salviae miltiorrhizae) was also found to improve pinopodes expression on endometrial surface, eventually better the uterine receptivity and improve the embryo implantation (Huang et al., 2004). Another Chinese medicinal formula, Bushenantai Recipe (consisting of Radix codonopsis, Rhizoma atractylodis, Fructus evodiae, Herba cistanches, Fructus corni, Radix angelicae sinensis, Radix salviae miltiorrhizae and Caulis spatholobi) could increase the expression of leukemia-inhibitory factor (LIF) mRNA and protein in endometria of mice with embryonic implantation dysfunction. It was suggested that Bushenantai Recipe could improve embryo implantation of mice with embryonic implantation dysfunction by promoting the endometrial LIF expression and endometrial decidualization (Zhang et al., 2008). CHM and acupuncture have significant advantages in improving the outcomes of IVF and ET. However, most of the relevant researches are clinical researches and only a limited number of studies focused on the mechanism. To explore the mechanism of CHM and acupuncture in improving the outcomes of IVF and ET will lead to better clinical practices of the combination of TCM and ART in the future. A standard TCM treatment should also be established to enforce the great advantages of TCM in the field of ART. Chronic pelvic inflammation Chronic pelvic inflammation is a frequently encountered disease in female genital system. Most cases of chronic pelvic inflammation result from acute pelvic inflammation which had not been cured thoroughly, but there are some patients without any acute inflammatory medical history. The main clinical manifestations are low fever and lassitude, abdominal pain, irregular menstruation dysmenorrhea and sterility. Examination of gynaecology shows that the uterus is often in a posterior position; its movement is restricted or it adheres to the circumferential tissues, resulting in lump formation; appendixes on both sides are often obviously thickened. TCM has gained satisfactory effects in treating chronic pelvic inflammation in the past years. The ancient Chinese medical physicians said, “Chong meridian is the sea of twelve meridians, the sea of five Zang and six Fu”; “Stomach is the acquired Essence, the sea of food stuff”, “Kidney is the congenital Essence, the root of primordial Qi”. Therefore Chong meridian is selected to strengthen the functions of five Zang and six Fu, dredge twelve meridians to further strengthen the Stomach, invigorate the Spleen and tonify the Kidney. Ren meridians can govern Yin meridian-Qi of the whole body, and is the sea of Yin meridians. Therefore the acupoints of Ren meridian are selected to treat abdominal pain and lumbago, irregular menstruation and sterility. Acupuncture combined with moxibustion has the functions of warming and promoting Qi and the Blood, strengthening the body resistance to eliminate pathogenic factors and relieving swelling and dissolving lump, so as to achieve the aim of treating chronic pelvic inflammation. Qi Jie Granule, which consisted of Radix astragali, Resina draconis, Radix angelicae sinensis, Ramulus cinnamomi, Caulis sargentodoxae, Herba patriniae, Radix et rhizoma rhei preparata, Myrrha, Radix paeoniae rubra, Radix glycyrrhizae, has been found to have a satisfactory curative effects in treating chronic pelvic inflammation through improving blood viscosity and regulating T-lymphocytic subgroups (Zhang et al., 2004). In a study to observe the clinical efficacy of Penyanqing Capsule (PYQC, consisting of Radix Salviae Miltiorrhizae, Radix paeoniae rubra, Fructus Aurantii Immaturus, Radix Ilicis Pubescentis, etc) in treating pelvic inflammation of Qi-Stagnation with Blood stasis syndrome, the total effective rate in the PYQC group was 83.3%, which was insignificantly different from that in the control group and PYQC could significantly lower the hemorrheologic indexes in patients and showed definite influences on the pathogenetic chlamydia and mycoplasma (Shen et al., 2005). Chronic pelvic inflammation is mainly caused by accumulated Heat in the Liver Channel, Stagnation of the Liver-Qi affecting the Spleen, failure of the Spleen to resolve Dampness and Dampness interweaving with Heat. A long-standing illness may lead to the obstructed circulation of Qi and Blood and blockage of Blood vessels to form lumps. TCM decoction has an immediate effect on those mild cases with short courses. However, it is appropriate to use acupuncture and moxibustion for those with serious and a lingering illness. In differentiating the syndromes, attention should be paid to the constitution of the Deficiency and Excess. Acupuncture, moxibustion and the ancient recipe Long Dan Xie Gan Tang used together have been found to enhance the therapeutic effects on chronic pelvic inflammation, in which, reducing method was applied at ZhongJi (CV-3), Guanyuan (CV-4) and Zigong (EX-CA-1), reinforcing method at Zusanli (ST-36), Sanyinjiao (SP-6) and Diji (SP-8) and indirect moxibustion with 3 medicated cakes was performed at Shenque (CV-8) (Jin, 2004). Zhao’s study showed that vitamin K3 acupoint injection at Sanyinjiao(SP-6) is an effective and safe measure for treating patients with primary dysmenorrhea, and it has also some effects in relieving pelvic pain caused by chronic pelvic inflammatory disease and endometriosis (Zhao et al., 2003). PCOS PCOS, with a prevalence of 5%–10%, is the most common endocrinopathy in women of reproductive age, and is characterized by chronic anovulation and hyperandrogenism. TCM has shown in many clinical studies to restore regular menstruation, relieve symptoms, and induce ovulation in PCOS patients (Hou et al., 2000; Stener-Victorin et al., 2000; Yu, 2004). To evaluate whether electro-acupuncture could affect oligo- /anovulation and related endocrine and neuroendocrine parameters in women with PCOS, twenty-four women with PCOS and oligo-/amenorrhoea were included in a non-randomized, longitudinal, prospective study (Stener- Victorin et al., 2000). In the study, the period was defined as the period extending from 3 months before the first electro-acupuncture treatment to 3 months after the last electro-acupuncture treatment (10-14 treatments altogether), a total of 8-9 months. Nine women (38%) experienced a good effect, showing increased rates of regular ovulations. These women also demonstrated significantly lower levels of body-mass index (BMI), serum testosterone concentration, serum testosterone/sex hormone hiding globulin (SHBG) ratio and serum basal insulin concentration and significantly higher levels of serum SHBG than those who did not respond to electroacupuncture. It was concluded that repeated electro-acupuncture treatments induced regular ovulations in PCOS with oligo-/amenotthoea (Stener-Victorin et al., 2000). Hou, et al. (Hou, et al., 2000) compared the effects of a common Chinese herbal formula (Tiangui Fang) with metformin in PCOS patients. They found that both metformin and the Chinese herbal formula could reduce the high serum levels of insulin in patients and induce regular ovulation. Moreover, the combined use of Bushen Houxue (BSHX), a Chinese medicinal formula, and ultrasound-guided follicle aspiration were found to be a safe and effective treatment for refractory PCOS with few trauma and CHM could significantly reduce dosage of HMG used for promoting follicle and the production of multiple mature follicles, thus avoiding the risk of ovarian hyperstimulating syndrome (OHSS) (Liang et al., 2008). In the study, forty-four patients with PCOS were randomly assigned to two groups by randomizing digital table, 20 in the observation group and 24 in the control group. The ultrasound-guided follicle aspiration was performed on both groups, and the decoction of BSHX, which consisted of Semen cuscutae, Radix rehmanniae praeparata, Herba taxilii, Herba epimedii, Fructus psoraleae, Rhizoma polygonati, Spina gleditsiae, Semen persicae, Rhizoma homalomenae, Radix salviae miltiorrhizae, and Radix glycyrrhizae, was given to the observation group one dose every day for 14 days in every menstrual cycle (Liang et al., 2008). In the past ten years, there emerged many clinical researches to investigate the effects of CHM and acupuncture on PCOS, however, almost all of them focused on the anovulation and few focused on the effects of CHM and acupuncture in treating PCOS-associated hyperandrogenism. Besides, few of the clinical researches has standard follow-up phase, and few studies has been done to explore the mechanism of CHM and acupuncture in treating PCOS. A standard animal model of PCOS should be established to explore the mechanism in the coming years. Cervicitis and vaginitis Cervicitis caused by ureaplasma urealyticum (Uu) is a clinically concurrent disease. Cervicitis caused by mycoplasma belongs to vaginal itching and leukorrhagia in TCM. In TCM, it is believed that this is due to an unrestrained sex life, exogenous excessive Heat, accumulation of toxin, insufficient Kidney Essence, evil Qi taking advantage of such weakness and intruding into the body and dampness, heat interacting with accumulation of toxin in the Lower Jiao, thus resulting in such symptoms as leukorrhagia, reddish and whitish discharge, swollen and itching vulva. A recent research was to observe the clinical therapeutic effect of Jieze No. 1, a Chinese medicinal formula, on cervicitis caused by Uu and its inhibitory effect on Uu in vitro (Wei et al., 2008). The main ingredients in Jieze No. 1 are Cortex phellodendri, Herba taraxaci and Borneolum syntheticum. A total of 393 patients suffering from cervicitis induced by Uu without other complications were randomly assigned to 3 groups, the combined treatment group: 140 patients treated with Chinese herbs Jieze No.1 by vaginal lavage, 30 min each time, once a day for 10 consecutive days and oral administration of Azithromycin, 1.0 g once every 72 h for three times; Jieze group: 115 patients were treated with Jieze No.1 alone by vaginal lavage, 30 min each time, once a day for 10 consecutive days; and the Azithromycin group: 138 patients were treated with oral administration of Azithromycin, 1.0 g once in 72 h for three times. All the patients were treated for 1 therapeutic course and condom were used for contraception during the treatment course. The Uu patients were examined again after 21 days of treatment. The total effective rate of the combined group was 85.3%, showing a significant difference compared with the Jieze group and the Azithromycin group. There was no statistical significance between the latter two groups. The clearing rate of Uu in the combined group, Jieze group and Azithromycin group was 78.4%, 60.9% and 47.9%, respectively. The combined group also showed a significant difference in comparison with the other two groups. The laboratory study confirms that Jieze No. 1 has an inhibitory effect on ureaplasma urealyticum strain and it has a remarkably effective therapeutic effects on drug-resistant strains, which is worthy of further research (Wei et al., 2008). According to TCM, the internal cause of vaginitis is long-term pent-up Liver Qi transforming into Heat, typically complicated by a vacuous Spleen not moving fluids. When body fluids stop flowing, they gather, accumulate and transform into Dampness. Liver Heat and Spleen Dampness become mutually entangled and pour downward, invading and soaking the vagina. With the passing of time, toxic evils are usually engendered internally. The external causes of vaginitis mostly have to do with poor vaginal hygiene and toxic evils. Evil toxins burn and damage the vagina causing inflammation. Modern TCM gynecology texts typically divide vaginitis into three distinct patterns: trichomonas vaginitis, hemophilus vaginitis, and senile vaginitis. CHM has good curative effects in treating the disease (Du et al., 2002). For those who suffered from trichomonas vaginitis, Wu Mei Yin Chen Tang (consisting of Fructus mume, Fructus zanthoxyli, Flos lonicerae, Herba artemisiae scopariae, Herba polygoni avicularis, Sclerotium poriae cocos Rhizoma atractylodis, Cortex phellodendri, Radix gentianae) is advised to be orally administered, and a Chinese medicinal formula composed of Radix sophorae, Fructus cnidii, Radix stemonae, Rhizoma coptidis and Herba euphorbiae helioscopiae was used for external wash (Decoct and use both as a fumigant and a wash. In other words, the patient should squat over the steaming decoction exposing their genitalia to the steam rising off it. After the liquid has cooled to be bearable to the skin, the genitalia should be washed with this decoction. This should be repeated once each morning and night for seven consecutive days) (Du et al., 2002). For those who suffered from hemophilus vaginitis, Long Dan Xie Gan Tang Jia Jian (consisting of Radix gentianae, Radix scutellariae, Cortex phellodendri, Fructus gardeniae, Rhizoma atractylodis, Fructus kochiae, Radix rehmanniae, Caulis akebiae and Semen plantaginis) is advised to be orally administered, and a Chinese medicinal formula composed of Fructus cnidii, Radix sophorae, Cortex phellodendri, Fructus zanthoxyli, Alumen and Cortex dictamni was used for external wash (the usage as above) (Du et al., 2002).. For those who suffered from senile vaginitis, Zhi Bai Di Huang Wan Jia Jian (consisting of Radix rehmanniae, Cortex moutan, Fructus corni, Rhizoma alismatis, Sclerotium poriae Cocos Radix dioscoreae, Rhizoma anemarrhenae, Cortex phlellodendri, Rhizoma smilacis glabrae, Flos lonicerae, and Radix paeoniae rubra) is advised to be orally administered, and a Chinese medicinal formula composed of Radix sophorae, Fructus cnidii, Herba mercurialis leiocarpae, Radix glycyrrhizae, Herba taraxaci, and Radix paeoniae rubra was used for external wash (the usage as above) (Du et al., 2002). In conventional Western medicine, gynaecological disorders/conditions are often treated with surgery, hormones, non-steroidal anti-inflammatory drugs (NSAID), antibiotics and so on. Though the efficacy of these treatments is rapid and widely accepted, there are many potential side effects such as nausea and vomiting related to surgery/anaesthetics; sexual problems after hysterectomy; skin rash or digestive problems related to drugs, or more seriously liver, kidney, and heart impairment related to some drugs, especially when taken for an extended period. Furthermore, some women may not respond to these treatments. The goal of any treatment is to relieve symptoms as well as to improve and restore the patient’s general health, and to improve their quality of life. This may be achieved by integration of complementary or alternative therapy such as TCM into conventional medicine. In China, there is a long history of treating gynaecological disorders/conditions with TCM. In modern times, the integrated medical care of combining conventional Western medicine with TCM has been safely provided by doctors as part of their routine medical practice in China and other Asian countries and part of western world. Thousands of case reports have shown the efficacy of TCM in the treatment of dysmenorrhoea and other symptoms/conditions associated with menstruation, PCOS, endometriosis, vaginal discharge, and many more. TCM can provide a safe and effective complementary or alternative to conventional medicine in treating gynaecological disorders. Acknowledgements Dr. Jue Zhou is funded by China Postdoctoral Science Foundation (No.20080441265), Zhejiang Traditional Chinese Medicine Foundation (No.2008YA015) and Zhejiang Province Postdoctoral Science Foundation. Dr. Fan QU is funded by the National Natural Science Foundation of China (No.30800390), China Postdoctoral Science Foundation (No.20070421188), Outstanding Young Medical Scientist Foundation of Zhejiang Province (No. 2008QN022) and Zhejiang Traditional Chinese Medicine Foundation (No. 2008YB010). References
© Copyright 2009 - African. Journal. Traditional, Complementary and Alternative Medicines The following images related to this document are available:Photo images[tc09040t1e.jpg] [tc09040t1c.jpg] [tc09040t1b.jpg] [tc09040t1a.jpg] [tc09040t1d.jpg] |
| |||||||||

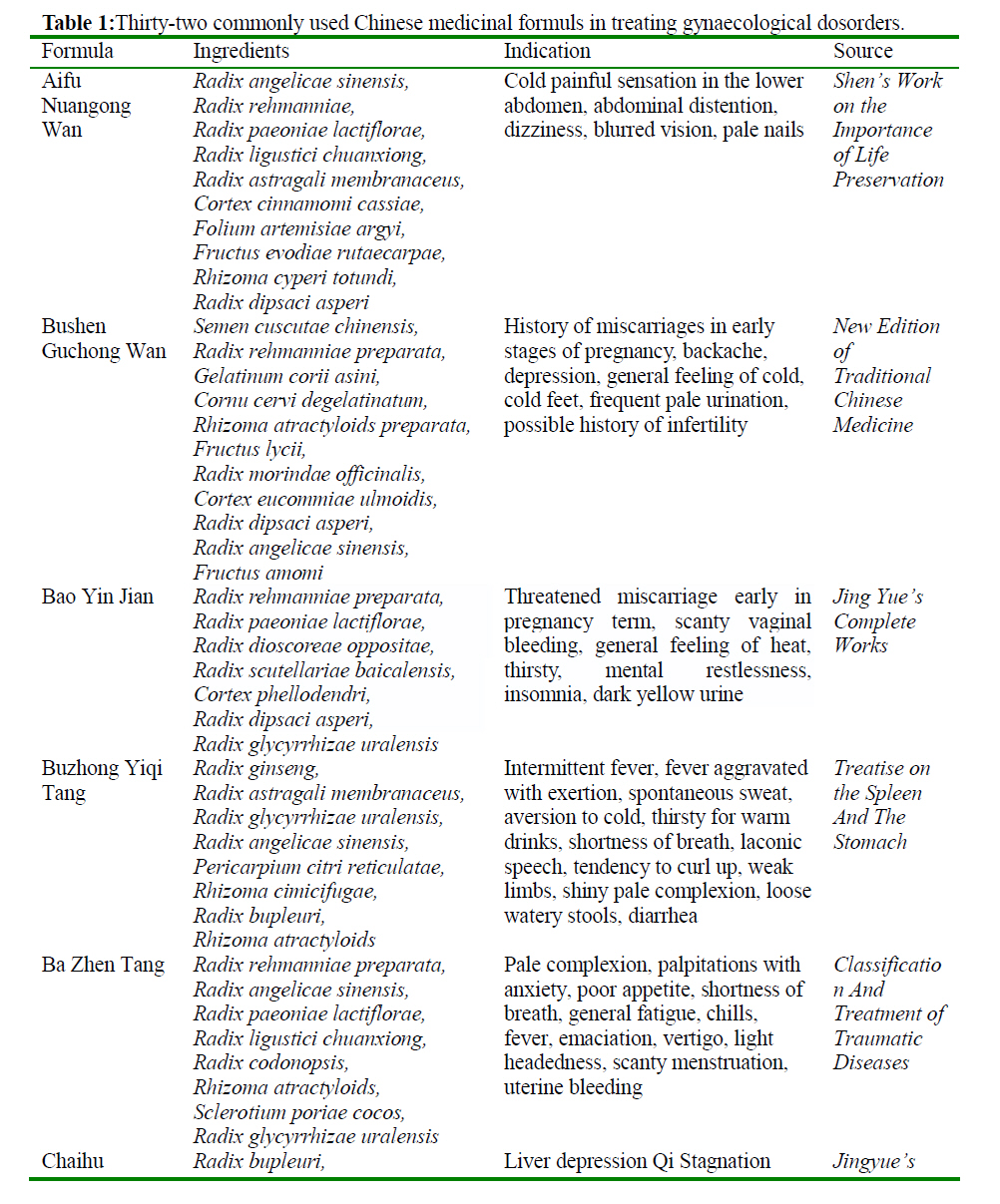{kind=link}
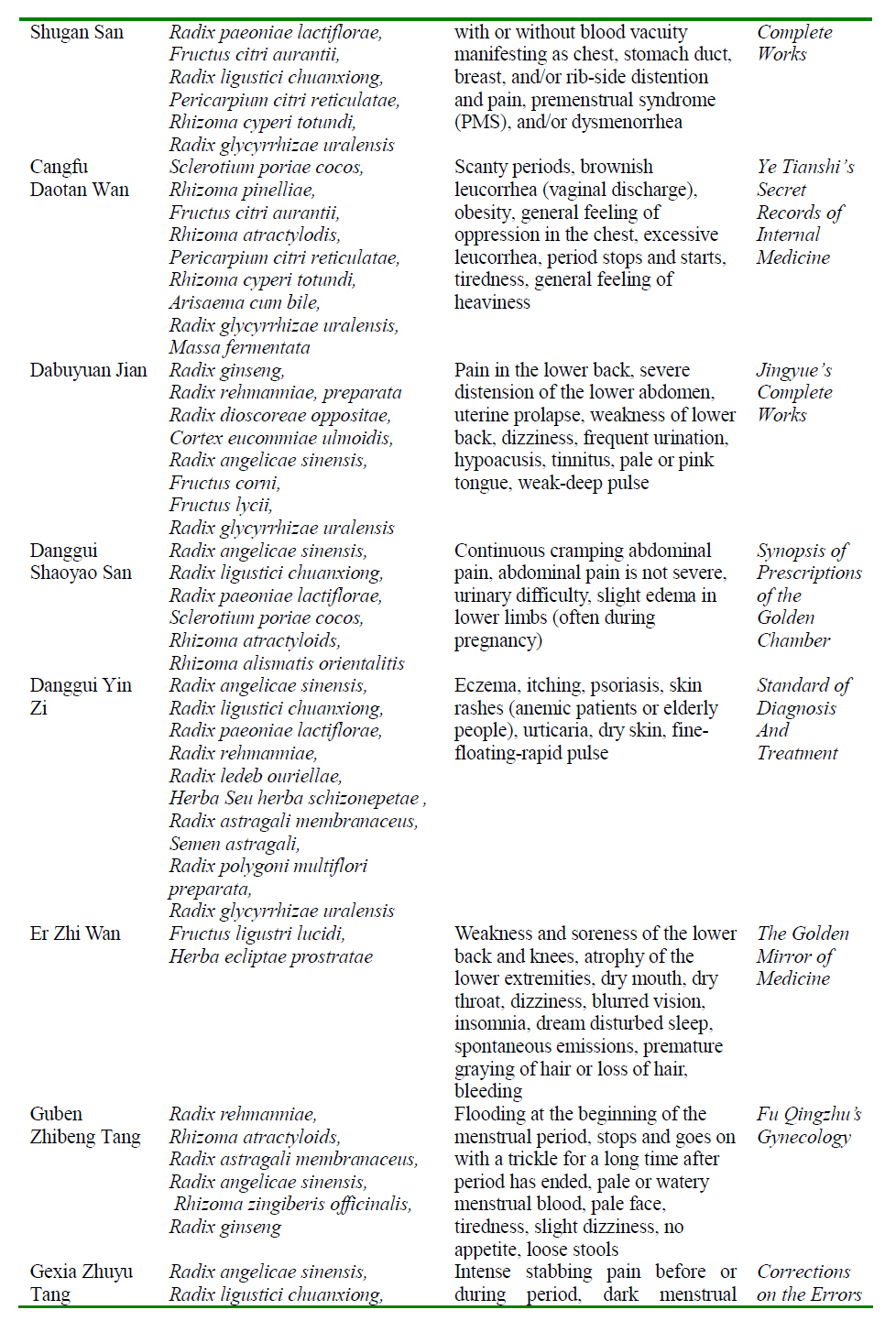{kind=link}
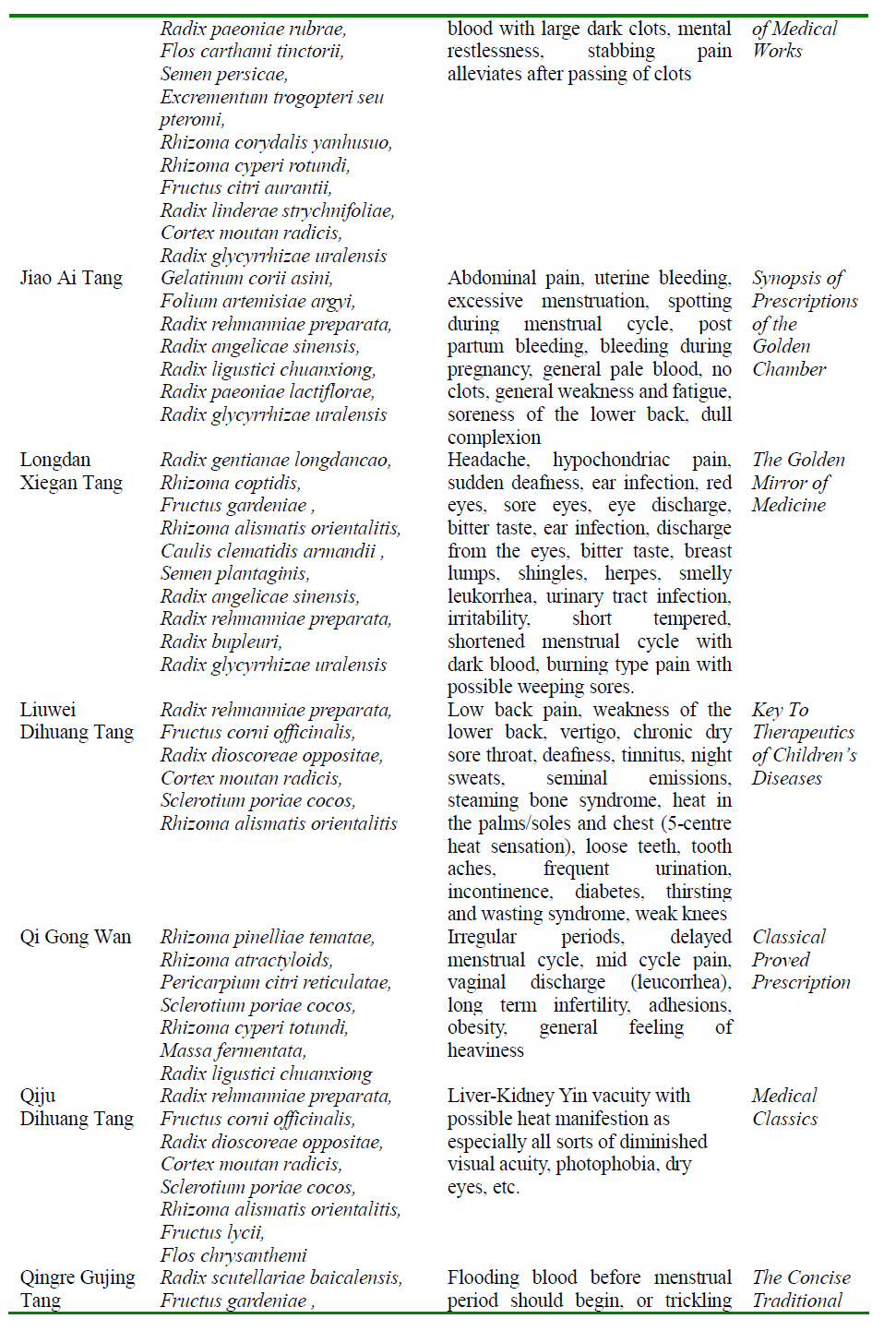{kind=link}
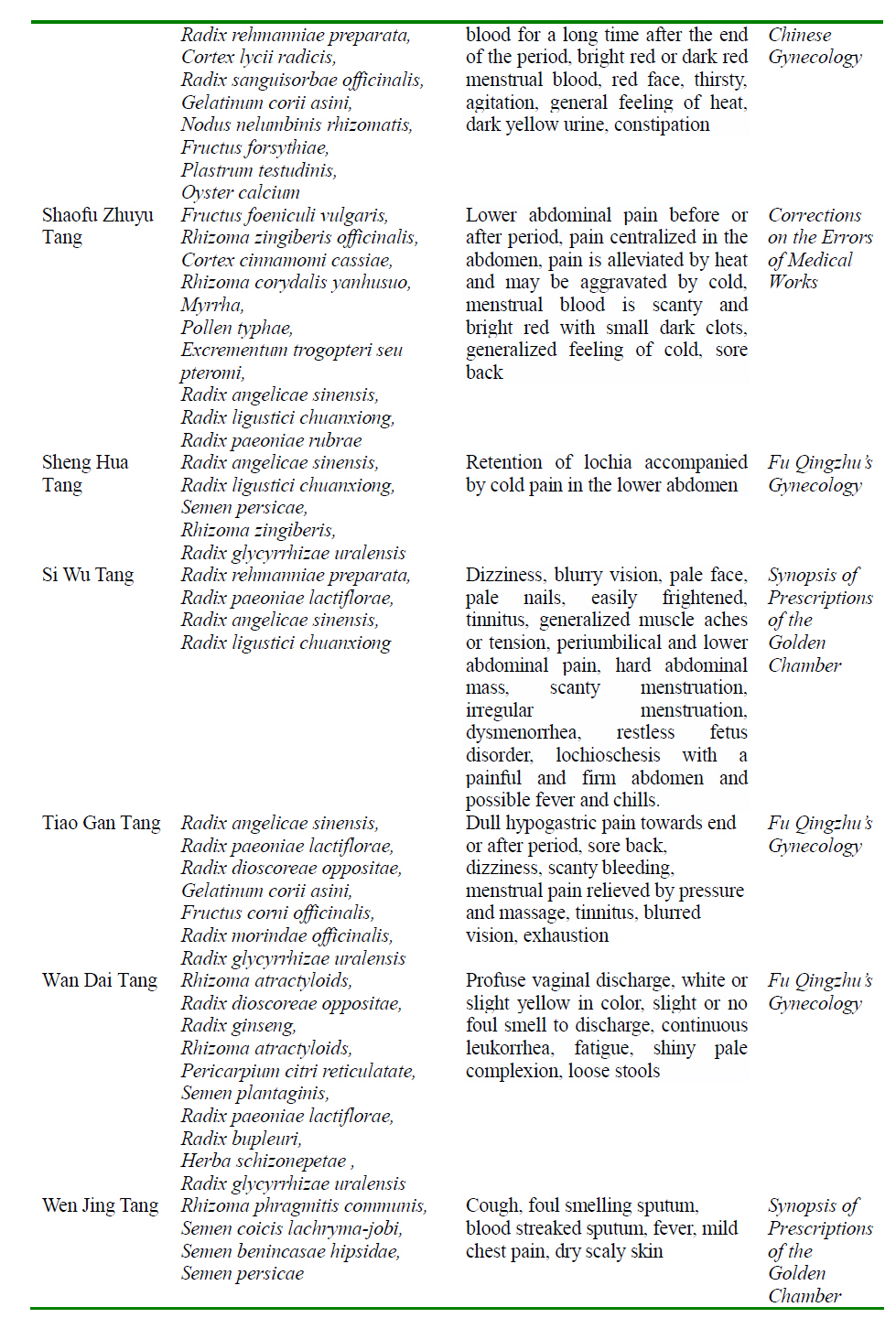{kind=link}
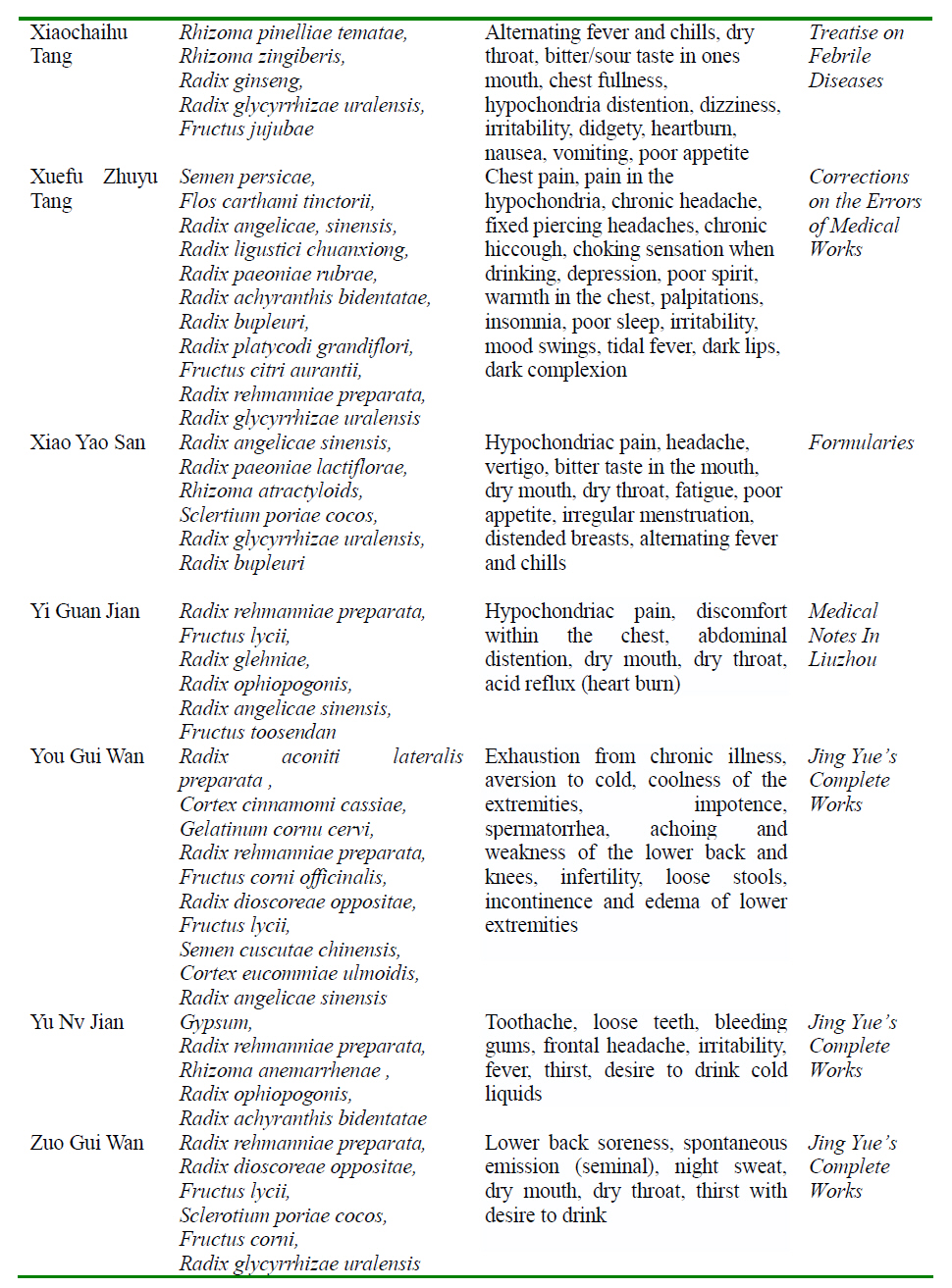{kind=link}