 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
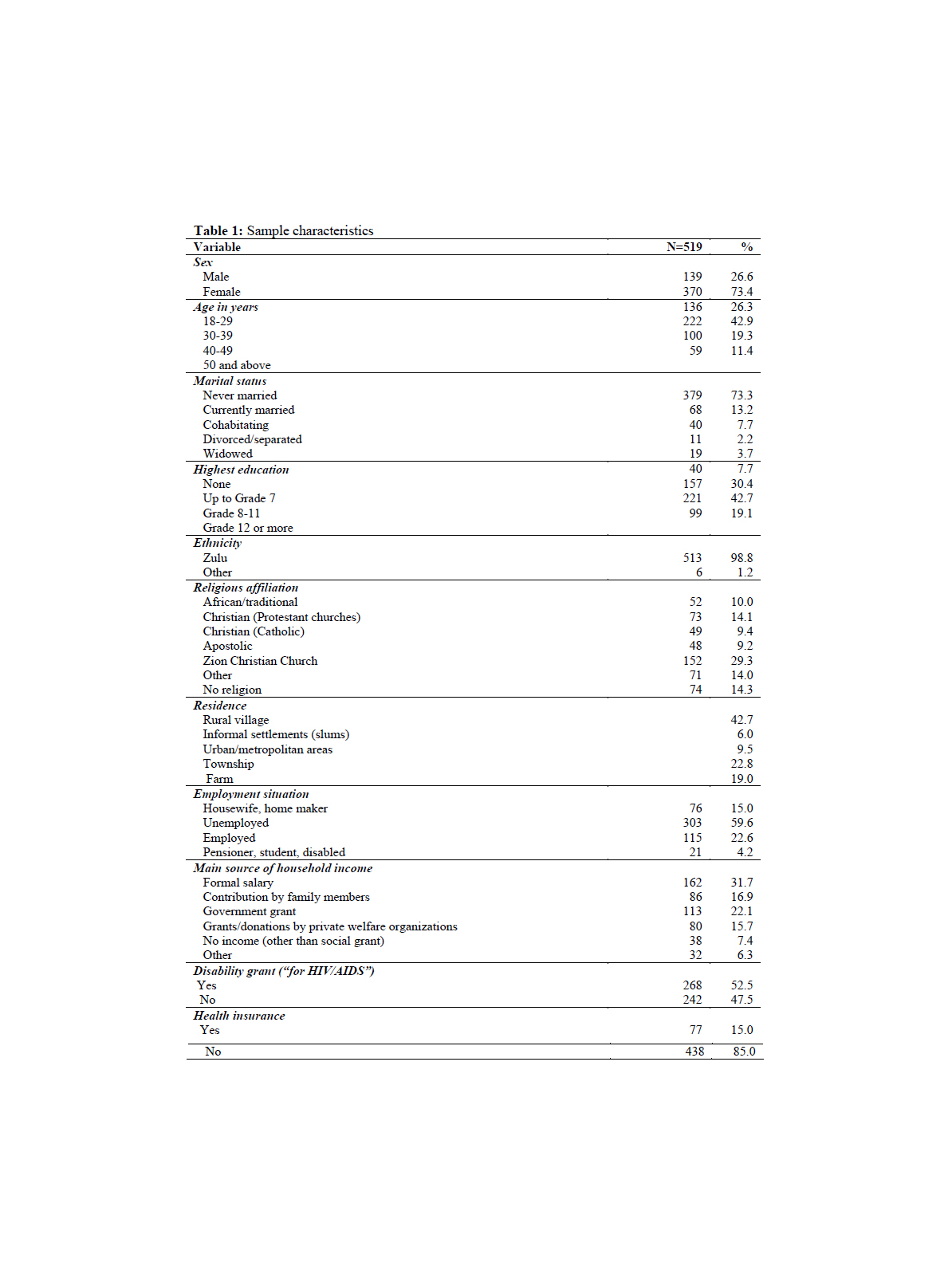
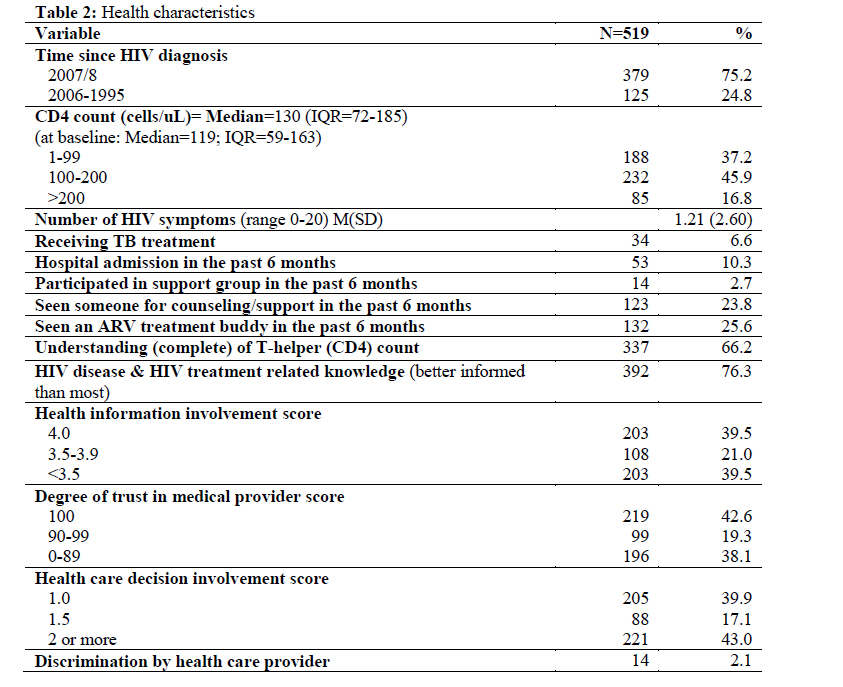
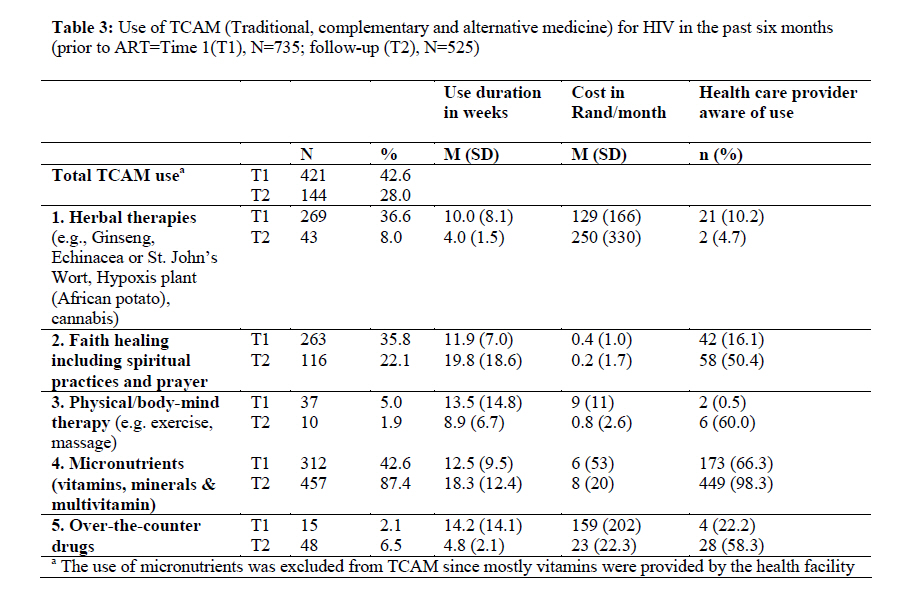
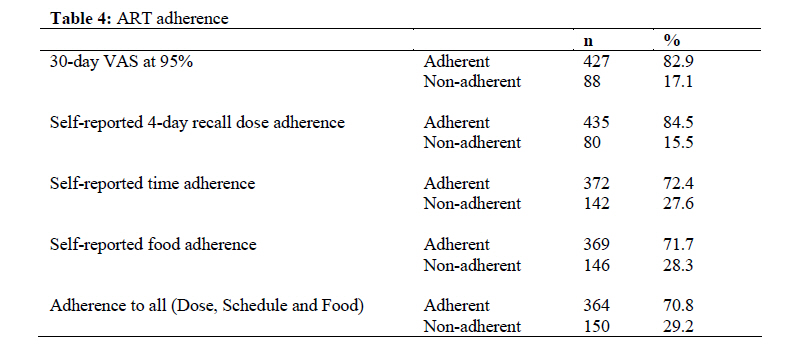
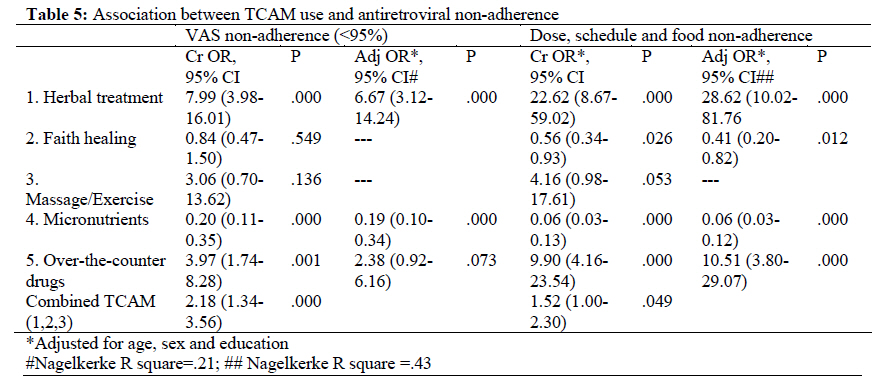
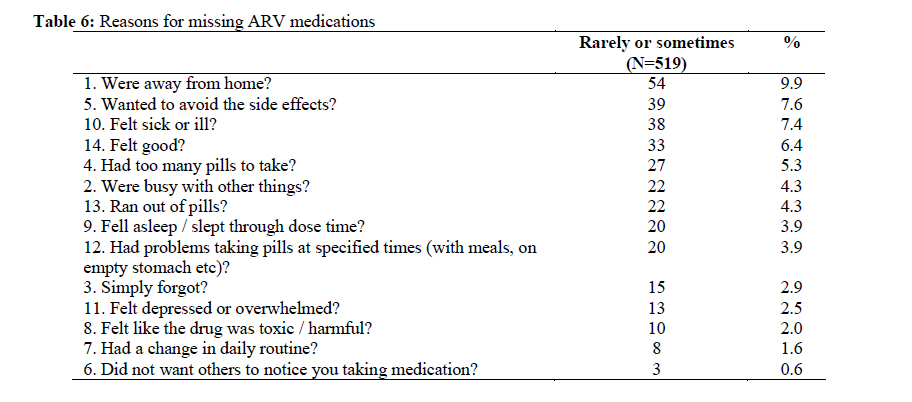
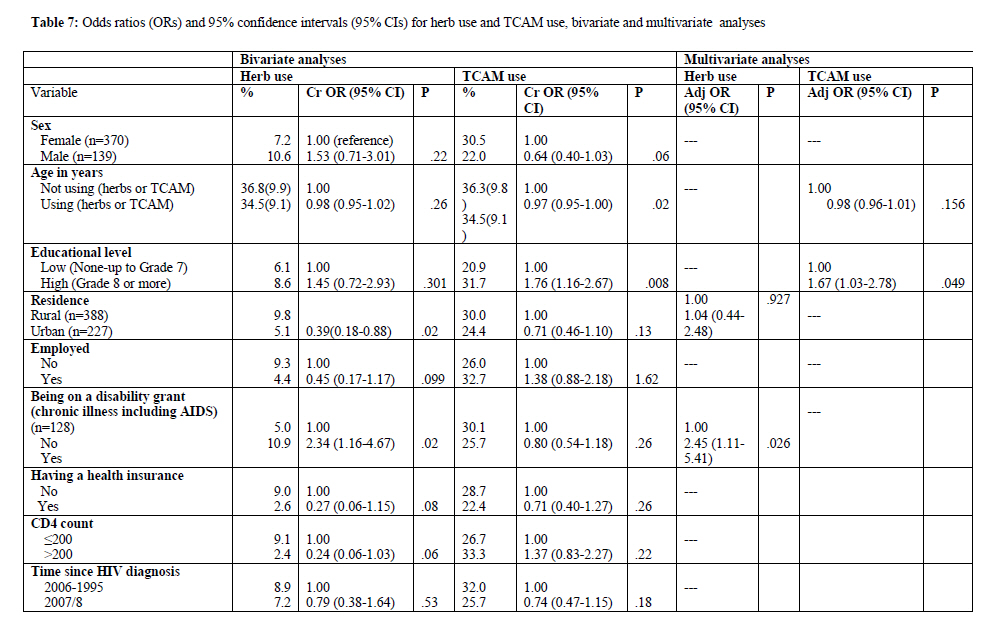
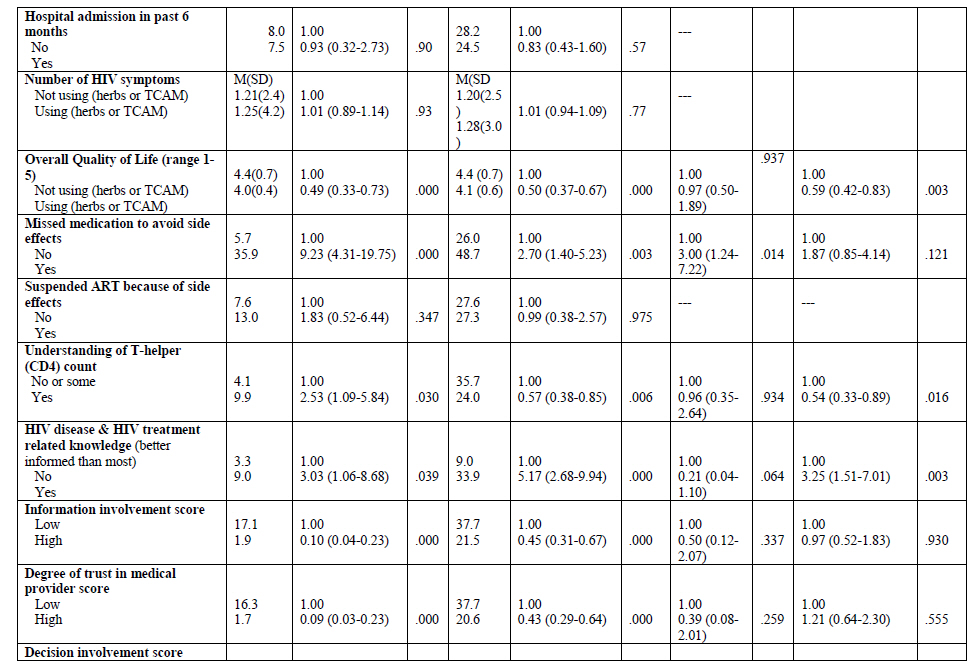
Afr. J. Trad. CAM, Vol. 7, No. 2, April-June, 2010, pp. 125-137 Research Paper TRADITIONAL COMPLEMENTARY AND ALTERNATIVE MEDICINE AND ANTIRETROVIRAL TREATMENT ADHERENCE AMONG HIV PATIENTS IN KWAZULU-NATAL, SOUTH AFRICA Karl Peltzer*1,2, Natalie Friend-du Preez3, Shandir Ramlagan1, Henry Fomundam4 and Jane Anderson5*1Health Promotion Research Unit, Social Aspect of HIV/AIDS and Health, Human Sciences Research Code Number: tc10020 Abstract Adherence to antiretroviral medication in the treatment of HIV is critical, both to maximize efficacy and to minimize the emergence of drug resistance. The aim of this prospective study in three public hospitals in KwaZulu-Natal, South Africa, is to assess the use of Traditional Complementary and Alternative Medicine (TCAM) by HIV patients and its effect on antiretroviral (ARV) adherence 6 months after initiating ARVs. 735 (29.8% male and 70.2% female) patients who consecutively attended three HIV clinics completed assessments prior to ARV initiation and 519 after six months on antiretroviral therapy (ART) Results indicate that the use of herbal therapies for HIV declined significantly from 36.6% prior to antiretroviral treatment (ART) initiation to 7.9% after being on ARVs for 6 months. Faith healing methods, including spiritual practices and prayer for HIV declined from 35.8% to 22.1% and physical/body-mind therapy (exercise and massage) declined from 5.0% to 1.9%. In contrast, the use of micronutrients (vitamins, etc.) significantly increased from 42.6% to 87.4%. In multivariate regression analyses, ARV non-adherence (dose, schedule and food) was associated with the use of herbal treatment, not taking micronutrients and the use of over-the-counter drugs. The use of TCAM declined after initiating ARVs. As herbal treatment for HIV was associated with reduced ARV adherence, patients’ use of TCAM should be considered in ARV adherence management. Key words: Traditional, complementary, alternative medicine, antiretroviral treatment adherence, HIV patients, KwaZulu-Natal, South Africa. IntroductionTraditional, complementary and alternative medicine (TCAM) broadly comprises herbal remedies, spiritual practices and prayer, traditional Chinese medicines, acupuncture, acupressure, chiropractic care, massage therapy, meditation, visualization, therapeutic touch and micronutrients (vitamins, minerals, and multivitamins). TCAM has been demonstrated to be widely used by people living with HIV (PLHIV), both on and off therapy with ARVs in many different settings (e.g., Langlois-Klassen et al., 2007; Ma et al., 2008; Peltzer et al., 2008; Reid et al., 2008). In a study in KwaZulu-Natal, South Africa, TCAM was commonly used for HIV in the past six months by study participants (317, 51.3%) and herbal therapies alone (183, 29.6%) prior to ART initiation. The use of micronutrients (42.9%) was excluded from TCAM since mostly vitamins were provided by the health facility. Herbal therapies were mainly used for pain relief (87.1%) and spiritual practices or prayer for stress relief (77.6%) (Peltzer et al., 2008). Babb et al. (2007) studied individuals (n=44) with moderate or advanced HIV disease attending a workplace clinic providing ART in South Africa, and found that 32% were using traditional medicines, most frequently African potato (9/14) and Aloe vera (3/14), and Malangu (2007) found among HIV-infected patients on ART (n=180) in Pretoria, South Africa, that 4.4% used African traditional medicine and 3.3% complementary and alternative medicines. There is data to suggest that TCAM impacts on ARV adherence, although the data is variable and findings are not consistent across studies. Littlewood and Vanable (2008) reviewed TCAM use and ART adherence among PLHIV and only two out of the seven studies identified had found an association between TCAM use and ART nonadherence. Jernewall et al. (2005) found that in a sample of HIV-positive Latino gay and bisexual men in the USA, users of Latino complementary and alternative medicines (CAM) were less likely to attend medical appointments and had lower rates of HAART adherence than users of Asian CAM (available within the clinics). The second study, also in the USA, found that HIV infected women (mostly African-American) who used TCAM such as vitamins and immunity boosters were more likely to report ART nonadherence in the past 30 days (Owen-Smith et al., 2007). In the 40 studies reviewed, TCAM use was associated with greater HIV symptom severity and a higher degree of disability among PLHIV (Littlewood and Vanable, 2008). Patients with a greater desire for medical information and involvement in medical decision making and with a negative attitude toward antiretrovirals were more likely to use TCAM (London et al., 2003), and one-third had not discussed such use with their health care provider (Hsiao et al. 2003). TCAM disclosure rates to health care providers varied from 38% to 90% across studies (Littlewood and Vanable, 2008). There seem to be no studies on the use of TCAM and its impact on ART adherence in Africa. Therefore, the aim of this prospective study is to assess HIV patients’ use of TCAM and its effect on ARV adherence 6 months after commencing ARVs at three public hospitals in KwaZulu-Natal, South Africa. MethodsThis is a prospective study of all treatment-naϊve patients (N = 735, Extra patients (ARV-naïve) were recruited to increase the initial baseline cohort sample size of 618) recruited from all three public hospitals in Uthukela health district in KwaZulu-Natal from October 2007 to February 2008. All ARV-naϊve patients who were about to commence ARVs (18 years and above) and who consecutively attended the HIV clinics during the recruitment period were eligible for this study. Details about the setting, sampling procedure and recruitment have been described elsewhere (Peltzer et al., 2008). Patients at six months follow-up were interviewed at the clinic. Patients who failed to attend for planned follow-up were contacted by telephone and up to two home visits. MeasuresPatients were interviewed with an anonymous questionnaire that requests information on sociodemographic characteristics, clinical history and health-related characteristics, TCAM use and health beliefs. Following initiation of ARVs, information on side effects, and changing or interrupting ART was also obtained. Clinical data relating to date of HIV diagnosis, HIV acquisition and transmission risk factors, current CD4 cell count, viral load (Chiron 3.0 bDNA), opportunistic infections, HIV and non-HIV medications was obtained from the medical chart. The use of TCAM was assessed with questions on 8 different TCAM methods over the past six months, the duration of usage, costs and the awareness of the health care provider of using TCAM. The Revised Sign and Symptom Checklist for Persons with HIV DiseaseThe SSC-HIVrev is a 72-item checklist of HIV/AIDS specific physical and psychological symptoms, scored using the following scale: 0 = not present today, 1 = mild, 2 = moderate, 3 = severe (Holzemer et al. 2001). Femalespecific symptoms were removed, reducing the total to 64 (v. Peltzer et al. 2008). An HIV symptom index (symptom intensity) was created which weights each symptom’s presence (0 or 1) by a rating of 1–3 (mild, moderate or severe). Cronbach’s alpha of this scale for this sample was .084. Health-Related Quality of LifeThe WHOQOL-HIV BREF is based on the WHOQOLHIV measure, one of the two World Health Organization’s QoL instruments for use with HIV-infected populations. In this analysis only the individual respondent’s overall QoL and general health perception measured directly with ‘How would you rate your quality of life?’ (ranging from ‘very poor’ to ‘very good’) was used (WHO, 2002). HIV knowledge and patient-provider variablesParticipants' HIV-related knowledge and orientation towards treatment information were assessed with two indicators. Self-assessed knowledge about HIV/AIDS was measured with a single item, "How well-informed do you rate yourself to be about HIV disease and treatment relative to most people who are HIV positive?" Response options were 1 = much better informed than most to 5 = much less informed than most. Responses indicating that they perceived themselves to be "much better informed than most" and "somewhat better informed than most" were categorized as better informed (vs. those who viewed themselves as being "about as well informed," "somewhat less informed", or "much less informed") (London et al., 2003). The desired level of information involvement was assessed with two items, e.g. "I want to take an active role in the medical management of my HIV infection and its complications." Response options were 1 = strongly agree to 4 strongly disagree. These items were combined into a 4-point scale in which higher scores indicate a stronger desire for information (London et al., 2003). Cronbach’s alpha for this information desire index was .68 for this sample. Participants' degree of trust in medical providers was measured with two items, e.g. "How much do you trust your doctor or clinic to offer you high-quality medical care?" Response options were from 1 = completely to 5 = not at all. Responses to these questions were reversed, combined, and placed on a scale ranging from 0 to 100, in which higher scores indicate higher trust (London et al., 2003). Cronbach’s alpha for this trust in medical providers' index was 0.76 for this sample. Desired level of decision involvement reflected the extent to which participants wanted to be involved in medical decision making, e.g., "It is better to trust a doctor or a nurse in charge of a medical procedure than to question what they are doing". Response options were 1 = strongly agree to 4 strongly disagree. These items were combined into a 4-point scale in which higher scores indicate a stronger disagreement (i.e., greater desire for involvement in decisions about medical care) (London et al., 2003). Cronbach’s alpha for this desire for involvement in decisions index was .79 for this sample. The experience of discrimination in the health care system was assessed with 3 items, e.g. "Has anyone in the health care system ever exhibited hostility or a lack of respect toward you?" Response options were "yes" or "no". If the participant answered "yes" to any of the three items, he or she was coded has having experienced discrimination (London et al., 2003). Cronbach’s alpha for this health care provider discrimination index was .63 for this sample. Adherence assessmentARV treatment adherence was assessed by two self-reported adherence measures - the Adult AIDS Clinical Trials Group (AACTG) adherence instrument and the 30-day visual analog scale (VAS). The AACTG consists of nine questions that assess adherence from the previous 1-4 days, within the past week, prior to the interview. The instrument also assesses reasons for non-adherence (Chesney et al., 2000). The 30-day visual analog scale (VAS) provided an overall adherence assessment for a longer time interval. Both have been validated in resource-limited settings (Maneesriwongul, 2006; Sarna et al., 2005). Adherence is calculated as the % of doses taken over those prescribed. Adherence levels assessed from the VAS are defined as follows: full adherence = 100%, partial adherence >/= 95% and < 100%, and non-adherence as < 95% of prescribed doses taken since the last refill. Dose adherence was assessed by asking participants to report on how many days they had missed taking all their doses during the past 4 days. Dose non-adherence was defined as having missed all doses on at least one day during the past 4 days. Adherence to scheduling was measured by the question “Most anti-HIV medications need to be taken on a schedule, such as ‘2 times a day’ or ‘3 times a day’ or ‘every 8 hrs.’ The participants were asked to report how closely they followed their specific schedule over the last 4 days using a 5-point Likert scale, ranging from “never” to “all the time.” Schedule non-adherence was defined as having missed scheduling in the past 4 days. Adherence to dietary instructions was measured by first asking “Do any of your anti-HIV medications have special food instructions, such as ‘take with food’ or ‘on an empty stomach’ or ‘with plenty of fluids’?” If the response was “yes,” participants were asked to rate how often they had followed dietary instructions over the last 4 days using a 5-point Likert scale, ranging from never” to “all the time.” Schedule non-adherence was defined as having missed scheduling in the past 4 days. Food non-adherence was defined as not having followed special instructions over the last 4 days. Data analysisData were analyzed using Statistical Package for the Social Sciences (SPSS) for Windows software application programme version 17.0. Frequencies, means, standard deviations, median, interquartile range, were calculated to describe the sample. Bivariate analyses were conducted to examine the relationships between overall TCAM use, herbal remedy use and socio-demographic variables, health characteristics, ART adherence and further healthseeking behaviour variables. Multivariate logistic regression included in the model All variables statistically significant at the 5% level in bivariate analyses were included in the multivariate model. No significant interactions were found between socio-demographic variables health-seeking behaviour and health characteristics. In multivariate regressions, adjustment was made for site of care, to account for variations in practice patterns and demographic differences across sites. ResultsOf 735 patients (29.8% male and 70.2% female) who completed assessments prior to initiation of ARVs, 525 were able to complete the assessment at six months follow-up. Of the original cohort, 75 had died, 57 had been transferred, 54 could not be traced, 23 refused the interview and 1 interview was incomplete. At six months following proposed ARV initiation, 519 patients started therapy and six failed to start treatment. Over the six month period 24 patients (4.6%) had temporarily suspended ARVs because of side effects, and three (0.6%) had changed their ARVs. HIV medications for 411 (79.8%) patients included Lamivudine (3TC), Starivudine (d4T) + efavirenz (Stocrin) and for 107 (20.8%) Lamivudine (3TC), Starivudine (d4T) + nevirapine. Socio-demographic characteristicsNearly three-quarters (73.5%) of the 519 patients who had initiated ARVs in this sample were female, 62.2% of whom were between 30 and 49 years old. Nearly three-quarters (73.3%) were never married, 61.9% had Grade 8 or higher formal education, almost all (98.8%) were Zulu and the largest religious affiliation was charismatic churches (38.5%). The majority of the sample (61.7%) lived in rural areas and was unemployed (59.6%). Only 31.7% of respondents had a formal salary as their main source of household income, 52.5% was in receipt of a disability grant and 15% had health insurance (Table 1). Health characteristicsMost patients (75.2%) had been diagnosed with HIV in the year prior to study recruitment. The median CD4 count at follow-up was 130 cells/cu.mm compared to 119 cells/cu.mm prior to ARV initiation. The mean number of HIV symptoms reported at follow-up was 1.21, 6.6% of patients were receiving TB treatment, 10.3% had at least one hospital admission in the past six months, and 25.6% had seen an ARV treatment buddy at least once in the past six months. Over three-quarters of patients (76.3%) felt that they were better informed than most about HIV and HIV treatment, with 66.2% reporting to have a complete understanding of T-helper (CD4) count. The majority of respondents (60.5%) had a high health information involvement score (3.5 or above), 61.9% had a high degree of trust in their medical care provider (90 or more), and 43% reported a moderate health care decision involvement score. Only very few (2.1%) reported any experience of discrimination in their health care system (Table 2). TCAM useThe use of herbal therapies for HIV declined significantly from 36.6% prior to ARV initiation to 7.9% after 6 months on ARVs. Faith healing methods (including spiritual practices and prayer) declined from 35.8% to 22.1% and physical/body-mind therapy (exercise and massage) declined from 5.0% to 1.9%. In contrast, the use of micronutrients (vitamins, etc.) significantly increased from 42.6% to 87.4%. At baseline, only 10.2% of patients reported that their health care provider was aware of their herbal remedy use. This figure declined to 4.7% after 6 months on ARVs. Patients were more willing to disclose faith healing methods than herbal remedies to their health care provider, with the disclosure rate increasing from 16.1% at baseline to 50.4% at follow-up (Table 3). At follow-up the main reason for using herbs for HIV was for immune supplementation (66.7%). Faith healing methods were mainly used to improve overall well-being (51.1%) and for stress relief (22.1%). Only 8 (1.5%) respondents believed that it was possible to treat HIV with TCAM alone. ART adherenceUsing the 30-day visual analog scale (VAS) 427 patients (82.9%) were 95% adherent in the month prior to the survey. Results from the AACTG adherence instrument found that on the 4-day recall dose adherence, 15.5% of patients were non-adherent (having missed at least one full day of medication in the past four days). 70.8% of patients were adherent to all parameters (dose, schedule and food) (Table 4). Bivariate and multivariate regression analyses found that the use of herbal treatment, not using micronutrients (available from clinics), the use of over-the-counter drugs and overall TCAM use (herbs, faith healing and massage/exercise) were associated with VAS as well as dose, schedule and food non-adherence. The use of faith healing methods and massage/exercise was associated with neither VAS nor dose, schedule and food non-adherence (Table 5). The main reasons for having missed ARV medications were “being away from home” (9.9%), followed by “wanted to avoid side effects” (7.6%), felt sick or ill (7.4%) and felt good (6.4%) (Table 6). Bivarate analysis found that herbal treatment use for HIV was associated with rural residence, being on a disability grant, lower reported overall quality of life, missing ARVs in order to avoid side effects, an understanding of CD4 count, better self-reported HIV disease and treatment knowledge, lower health care information involvement score, higher health care decision involvement score and having seen an ARV treatment buddy or a counsellor at least once in the past six months. In multivariate analysis having missed ARV medication in order to avoid side effects and being on a disability grant were significant predictors of the use herbal treatment for HIV. In bivariate analyses overall TCAM use was associated with younger ages, higher educational level, lower self-reported quality of life, missing ARVs in order to avoid side effects, better self-reported HIV disease and treatment knowledge, lower health care information involvement score, lower degree of trust in medical provider score, higher decision involvement score and having seen an ARV treatment buddy or counselor. In multivariate analysis, higher education, lower self-reported quality of life, a lack of understanding of CD4 count, higher selfreported HIV disease and treatment related knowledge and higher health care decision involvement were significant predictors of TCAM use for HIV (Table 7a & b). Discussion In this South African HIV patient cohort, the use of herbal therapies for HIV prior to initiation of ARVs declined significantly from 36.6% prior to ART initiation to 8.0% after being on ARVs for 6 months. The level of reported use of herbal therapies by PLHIV in Africa varies across studies, however, the decline in use of herbal remedies after initiating ARVs appears to be a consistent finding. In Uganda for example, Langlois-Klassen and colleagues (2007) found that the use of traditional herbal remedies had declined from approximately 90% prior to HIV diagnosis to 53% amongst patients with HIV-related symptoms on ARVs. For patients on supportive treatment and not ARVs, this figure was higher at 63%. In a small cross-sectional study (N=44) of workplace clinic attendees in South Africa, only 23% of the 30 people taking ARVs reported current use of traditional medicine, despite 84% reporting use of traditional medicine in the past (Babb et al., 2007). Outside of Africa, similar results have been found. Agnoletto, Chiaffarino, Nasta and colleagues (2006) for example, reported that TCAM use was less common among respondents taking ARVs compared to those not on ARVs. The reason for a reported decline in use of herbal medicine after initiating ARVs may in part be due to patients’ reluctance to disclose their use of herbal remedies, particularly as their physician’s advice against concomitant medicine use. In addition, ART naïve patients receive once they have been identified as possible ART candidates in South Africa, especially at our sample hospitals, training on correct ART adherence which discourages the use of herbal medicines (Ramlagan and Peltzer, 2008). In the present study most (95%) of the health care providers were not aware that their patients were taking herbal treatments. Similarly, Langlois-Klassenet al. (2008) found in Uganda that only 16% of respondents had informed their conventional medical practitioners about their use of herbs. According to the South African National ARV Treatment Guidelines (Department of Health, 2004) patients must disclose any over-the-counter drugs and traditional medicines due to the possibility of contraindications and adverse drug interactions. Caution is noted that TCAM use has the potential for adverse effects (Hsiao et al., 2003). In the present study, a decline was also seen however in less controversial practices such as faith healing methods (including spiritual practices and prayer) and physical/body-mind therapies (exercise and massage), despite an increase in disclosure rates to providers. An alternative explanation may, therefore, be that improved physical well-being as a result of ARVs and improved understanding of adherence may have reduced the need for use of TCAM. In the present study, the use of herbal treatments was associated with ARV non-adherence, which is confirmed from some other studies (e.g., Owen-Smith et al., 2007) as were the major self-reported reasons for nonadherence ( “were away from home”, “wanted to avoid side effects”, “felt sick or ill” and “felt good”, (Golin et al., 2002). In this study “having missed ARV medication to avoid side effects” and being on a disability grant were significant predictors for the use of herbal treatment for HIV. Agnoletto et al. (2006) also found that TCAM use was more common in outpatients who reported HAART-related side effects (specifically neuropathy). Higher education, lower quality of life, higher HIV disease and treatment related knowledge and higher health care decision involvement were significant predictors for TCAM use. These factors associated with TCAM use suggest that TCAM use may be associated with heightened awareness regarding the availability of such therapies, as found in other studies (Josephs et al., 2007). ConclusionHigh use of TCAM prior to ART seems to decline when starting ART. Herbal treatment for HIV was associated with non-adherence to ART and should be considered in ART adherence management. LimitationsOne limitation of this study is that the data have only one time adherence data, thereby limiting our ability to be certain about the temporal relationship between TCAM use and HAART adherence. Future longitudinal cohort studies are needed to provide evidence for temporality. A second limitation is the self-report data for both TCAM use and HAART adherence. Finally, the findings are derived from a sample of men and women residing in one district in one province in South Africa. Thus caution is urged in generalizing the findings to other districts and provinces in the country. Acknowledgement We thank the TIBOTEC REACH initiative for funding this study. References
Copyright 2010 - Afr. J. Trad. CAM The following images related to this document are available:Photo images[tc10020t4.jpg] [tc10020t3.jpg] [tc10020t7c.jpg] [tc10020t1.jpg] [tc10020t6.jpg] [tc10020t5.jpg] [tc10020t7a.jpg] [tc10020t2.jpg] [tc10020t7b.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}