 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
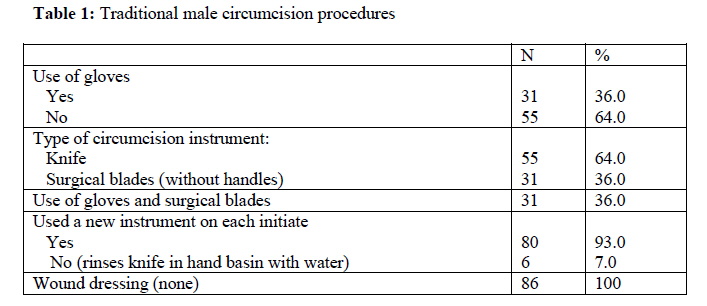
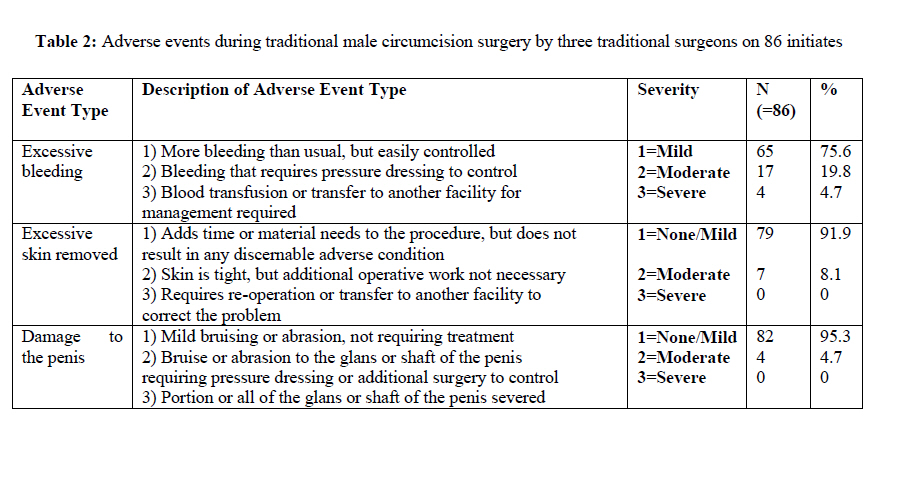
Afr. J. Trad. CAM, Vol. 7, No. 2, April-June, 2010, pp. 153-159 Research PaperEVALUATION OF A SAFER MALE CIRCUMCISION TRAINING PROGRAMME FOR NDEBELE TRADITIONAL SURGEONS AND NURSES IN GAUTENG, SOUTH AFRICA: USING DIRECT OBSERVATION OF CIRCUMCISION PROCEDURES Karl Peltzera, Xola Kantab and Mercy BanyinicaSocial Aspects of HIV/AIDS and Health, Human Sciences Research Council, Pretoria, South Africa& Department of Psychology, University of the Free State, Bloemfontein, South Africa. Code Number: tc10023 Abstract The aim of this study was to assess the safety of traditional male circumcision practices among Ndebele traditional surgeons following a five days training by direct observation of circumcision procedures. The sample included eight Ndebele traditional surgeons and traditional nurses and 86 initiates (abakhwetwa) from two districts in Gauteng province in South Africa. A structured observations tool was administered by a trained research doctor during circumcisions and (wound) care of the initiates of the trained traditional surgeons. Results indicate that from the observations of 86 traditional male circumcisions a high number (37%) of adverse events were recorded (excessive bleeding, excessive skin removed and damage to the penis) and in six cases the use of one instrument for the circumcision was observed. Before scaling up and/or considering integration traditional male circumcision services into medical male circumcision services in South Africa, a careful strategy to minimize unnecessary morbidity, and fundamental improvements on current traditional male circumcision techniques, are required. In addition, legislation and control of traditional male circumcision in Gauteng province, where the study took place, are recommended to make traditional male circumcision safer and to prevent adverse events to happen. IntroductionConnolly and co-workers (2008) found in a national survey in South Africa in 2002 that of a sub-sample of 3025 men, 15 years and older, 35.3% who had been circumcised, the majority (57.2%) had been circumcised traditionally and 42.8% medically. The vast majority of Whites (97.8%), Indians (92.8%) and Coloureds (87.4%) were circumcised medically, compared to only 21.8% of black Africans. The median age of circumcision for black South Africans was 18 years compared to 10 years for Coloureds, 2 years for Whites and 1 year for Indians. The prevalence of traditional male circumcision was found to be 24.8% (more than medical male circumcision=13.2%), and the prevalence of traditional male circumcision was 31.9% among Black African men. Yet, there were stark differences among different African ethnic groups in traditional male circumcision rates, ranging from 71.1% among Venda, 60.5% Northern Sotho, 57.3% Xhosa, 57.0% Ndebele to 2.4% among Swati and 10.7% among Zulu. The age of traditional male circumcision is across ethnic groups mainly 18 years and above (58.2%), followed by 12 to 17 years (33.1%) and 0 to 11 years (8.8%), while there are differences by ethnic groups; for example for the Ndebele, Xhosa, Southern Sotho, and Tswana the age of traditional male circumcision was mainly 18 years and above, and for the Swati, Northern Sotho and Tsonga it was mainly 12 to 17 years, and for the Venda it appears the age of traditional male circumcision was below 12 years (Peltzer, 2009). The “Ndebele male initiation is a post-puberty ritual when boys between ages of 18 to 20 years are circumcised and ‘taken to the bush’ where they are secluded for a period of two months from April to June. At the lodge they are instructed by abarhuki (instructors) in an esoteric (secret) language on a variety of topics: kinship values, male adult responsibilities, how to recite the clan praises, etc… Manhood or male identity seems to be of primary importance in Ndebele communities, rather than the acquisition of any form of ethnic identity. Manhood and man is conceptually contrasted and balanced with no manhood and non-men. To understand male identity one also has to understand the need for male bonding, and how ‘the wisdom of the father’ is replaced by the knowledge and judgment of the peer group, in this case age-mates who are to become circumcision peers.” (Van Vuuren and De Jongh, 1999: p. 151, 153). Characteristics of contemporary traditional male circumcision procedures in South Africa may include: (1) circumcision is performed in the mountains or forests; (2) The circumcision procedure is done by a lay male person (the traditional surgeon); (3) The traditional surgeon uses a traditional instrument, usually a spear, although recently they have been using knives; (4) Bare hands are used to handle the penis, circumcision instrument and the wound; (5) Often a number of initiates are circumcised using one instrument; (6) Initiates are circumcised without anaesthesia, and (7) The circumcision instruments are washed and cleaned with soap, and sometimes with detergents and no sterilizing solution (Kanta, 2003, 2004). Numerous accounts of complications from traditional male circumcision and initiation into manhood are available, but the rate of adverse events cannot be calculated because none of the reports include a denominator (Bailey et al., 2008). Research indicates many complications and even deaths due to traditional male circumcision (Mayatula and Mavundla, 1997; Magoha, 1999). Examples of these problems include: mutilations as a consequence of botched surgery, infection of circumcision wounds, gangrene of the penis, severe hemorrhage, respiratory infection, dehydration, penile amputation, delayed wound healing, insufficient skin removal, torture and assault resulting in serious injuries, disability or even deaths, and one circumcision instrument may be used for several initiates, leading to speculation that cases of wound sepsis, viral hepatitis B and HIV transmissions occur (Bailey et al., 2008; Crowley and Kesner, 1990; Du Toit and Villet, 1979; Gounden, 1990; Kanta, 2003; Marck, 1997; Mayatula and Mavundla, 1997; Mogotlane et al., 2004; Ngqaza, 1997; Peltzer, et al., 2008b). Prior to promoting traditional male circumcision as part of a public health measure against the spread of HIV, the feasibility and safety of the procedure within target countries should be evaluated to understand what measures need to be taken to ensure access to safe circumcision services (Bailey et al., 2008). There is limited data available on the safety of traditional male circumcision, in particular following a training intervention (Peltzer et al., 2008a; Peltzer et al., 2008b), and few have used direct observation of circumcision procedures (Bailey et al., 2008; Peltzer et al., 2008b). Future studies might include detailed observations of circumcision procedures in different settings combined with prospective studies of adolescent and young adult males in communities where circumcision is common (Brewer et al., 2009). Therefore the aim of this study was to assess the safety of traditional male circumcision practices among Ndebele traditional surgeons following a five days training by direct observation of circumcision procedures. Methods Sample The sample included eight Ndebele traditional surgeons (mean age=51.7 years, SD=11.3, range from 38-76) and 17 Ndebele traditional nurses (mean age= 44.6 years, SD=17.6, range 18-77) and 86 initiates (abakhwetwa) from two districts in Gauteng province. The number of years of formal education among traditional surgeons was 6.8 years (SD=2.7), range 5-12 years, and among traditional nurses 5.2 years (SD= 2.5), range from 5-14 years. Apart from being involved in male circumcision, 50% of traditional surgeons were mostly practicing as traditional health practitioners, while traditional nurses were either unemployed (81.3%), or working as a teacher (6.3%) or working as a labourer (12.5%). The number of male circumcisions performed by traditional surgeons in the past 12 months were on average 75 (SD=73.8), with a range of 5 to 240. The amount of money in Rand charged for performing a male circumcision was on average R70 (SD=25), with a range of 50 to 100 Rand. The number of male circumcisions cared for by traditional nurses in the past 12 months was on average 216 (SD= 238) with a range of 1 to 600 initiates. The traditional surgeons who have had experience of an initiate that became very sick in a life threatening manner or sick were (mean=1.7, SD= 0.44) with a range of 1-2. Traditional surgeons and nurses entered the field of traditional male circumcision and initiation into manhood and acquired their knowledge and skills through an apprenticeship, e.g. traditional surgeons (50%) had been trained by another traditional surgeon, 62.5% were trained by relatives and 92.9% of traditional nurses had learnt from observation of other traditional nurses. Procedures Traditional surgeons and nurses A database of (all) known traditional nurses and surgeons both trained and untrained were accessed from the Department of Health, Gauteng Province. The Department of Health personnel (district and provincial coordinators) together with the research project staff identified 8 untrained traditional surgeons and 17 untrained traditional nurses from Ndebele ethnic background in the selected study district. They were then contacted and enrolled in the study after informed consent had been obtained (to conduct a pre-and post -training assessment, to conduct training of a safer male circumcision, and to observe male circumcision) transported to the training venue. The pre-post training assessment found satisfactory results, as in a study reported elsewhere (Peltzer et al., 2008a) and is therefore not reported here. InitiatesThe research team obtained the scheduled circumcision dates from the eight trained traditional surgeons. Prior to the male circumcision conducted by a particular traditional surgeon, initiates register or book for this particular traditional surgeon. Initiates were then accessed by the researcher through this particular traditional surgeon. Only initiates 18 years and above (age were checked by self-report) were included. Informed consent was obtained from 86 initiates prior to male circumcision to observe the traditional circumcision procedure by a research doctor. Eighty six initiates, circumcised by three different trained traditional surgeons, were observed during their circumcision. A forth trained traditional surgeon conducted circumcision on six initiates with one surgical instrument only. He claimed that the ancestors have not blessed the surgical blades provided hence he was not going to use them or use one blade or circumcision tool for each initiate as he had only such circumcision tool. This was reported as an adverse event to the ethics committee, the study was suspended, and no further observations were made. The six initiates who were circumcised with one instrument were informed of the risk of transmission of HIV and other blood borne infections such as viral hepatitis B and were referred to an HIV counselling and testing centre after discharge from the initiation school. By then 289 initiates had been circumcised in that particular initiation school by the same traditional surgeon allegedly using the one instrument method for many initiates. The research protocol was approved by the Human Sciences Research Council (HSRC) Research Ethics Committee, the Provincial Health Department of Gauteng, and traditional authorities in the study area. Training interventionDr Xola Kanta conducted one intensive training in 2009 over five days to eight traditional surgeons and 17 traditional nurses. Topics that were covered during the training included: Introduction into initiation rites; Social, legal and cultural context of the practice; Roles and responsibilities of stakeholders; Normal anatomy and physiology of the male genital, with emphasis on structure of the penis; Congenital and acquired abnormalities of the male sex organs; Traditional circumcision instruments and their care; Recommended procedure of safe traditional male circumcision; Infection control measures; Sexually transmitted infections and blood borne infections, e.g. viral hepatitis B; HIVand AIDS; Aftercare of the initiate including after care of the circumcision wound and initiate as a whole; Detection and early management of common complications of circumcision; Nutrition and Fluid Management; Code of conduct and ethics for traditional health practitioners; Sexual health education; Role of alcohol and drugs; Human rights issues (Kanta, 2004). The training method included didactic, group discussion and simulation, including demonstrations of various instruments and techniques of traditional male circumcision. In particular, a disposable instrument (surgical blade) with a handle was recommended to be used for each initiate during traditional male circumcision; alternatively the surgeon will have to have several traditional circumcision instruments so that each initiate is circumcised by an unused cleaned and sterilized instrument; they were taught and compelled to use disposable latex gloves for each initiate when performing circumcision; a proper cleaning and sterilizing procedure for the re-usable traditional circumcision instrument were taught and demonstrated. Traditional surgeons were provided with a tool box which contained surgical (scalpel) blades, scalpel handles, latex hand gloves, sterilization chemicals and disinfectants, and paper towel rolls, and traditional nurses also received a tool box including latex hand gloves, sterilization chemicals and disinfectants, and paper towel rolls. Attendance certificates were issued at the end of the training session. More details of the training intervention have been described elsewhere (Peltzer et al., 2008a). MeasuresThe structured observations tool (Male circumcision adverse event form, WHO, 2008) administered by a trained research doctor during circumcisions and initial post – circumcision wound care of the initiates of the trained traditional surgeons and traditional nurses, assessing adverse events including excessive bleeding, excessive skin removed, and damage to the penis. Data analysisDescriptive statistics was used to desribe the proportions of traditional male circumcision procedures and adverse events during traditional male circumcision surgery using SPSS version 17.0. ResultsIn all, 86 traditional male circumcision procedures by three traditional surgeons were observed (surgeon 1=31 initiates, surgeon 2 = 49 initiates and surgeon 3=6 initiates). In only one-thirds (36%) of the initiates, surgical blades were used, while in the majority of cases (64%) a knife was used as circumcision instrument. In cases where surgical blades were used, the traditional surgeons had used gloves (36%), while in cases where a knife was used no gloves were used (64%). When surgical blades were used, they were used without the provided scalpel handles, but the traditional surgeon did not cut himself because previously he was using a razor blade and a razor does not have handles, so he did not encounter any problems. On the 80 initiates, a new instrument was used on each initiate, while on six initiates the same knife was used for all six circumcisions without sterilization (Table 1). From all 86 traditionally circumcised initiates, four (4.7%) were observed to have had severe excessive bleeding; they were referred to hospital for treatment, 17 (19.8%) had moderate bleeding. If the bleeding did not stop the traditional surgeon and nurse applied to the wound unspecified and unknown traditional medicines to control the bleeding for the initiate not to lose more blood. Seven (8.1%) had moderate excessive skin removed and four (4.7%) had moderate damage to the penis, not requiring treatment. In addition, examination found that one initiate had cellulites of the leg and another had severe Eczematous Lesion of the skin; they were taken to the hospital the same day. In all 32 initiates (37%) had some form of adverse event (see Table 2). Discussion The observations made on 86 traditional male circumcisions reviealed that in a number of cases (37%) adverse events were recorded (excessive bleeding, excessive skin removed and damage to the penis). In addition, in one large initiation school the traditional surgeon in charge used, as a routine, one instrument to circumcise several initiates at the same session without sterilizing the instrument, thus increasing the risk of transmission of HIV and other blood borne infectious diseases such as viral hepatitis B. Failure to observe basic universal infection control poses a serious occupational health risk to the traditional surgeons and nurses themselves as well as the initiates, with respect to the risk of transmission of HIV and other blood born infectious diseases such as viral hepatitis B, among other things. In the only other reported study (Bailey et al., 2008) where traditional male circumcisions were observed (n=12) a similar number of adverse events (35%) were found: four (33%) had permanent adverse sequelae including torsion and mutilation of the glans, five (42%) incomplete foreskin removed, four (33%) required recircumcision and five (42%) had an infection requiring antibiotics. The use of one instrument for several or many circumcisions has been reported (through observations by initiates) as common elsewhere in South Africa (Mayatula and Mavundla, 1997; Mogotlane et al., 2004). Concerns have been raised that such unhygienic traditional male circumcisions may increase risk of HIV in Africa (Moszynski, 2007). In this study, we found some aspects of the male circumcision adverse event form (WHO, 2008) were not user friendly for traditional male circumcision and therefore we recommend modifications as described in appendix 1 to more accurately assess the circumcision procedure. We further recommend that safe practices and infection control measures such as use of a pair of gloves and separate circumcision instrument for each initiate be a standard part of assessment of traditional male circumcisions. The levels of morbidity and perhaps mortality from traditional male circumcisions and initiation into manhood documented as occurring in this study and other studies (Bailey et al., 2008) are unacceptable. Roughly one-third of South African men are circumcised, the majority (65%) by traditional circumcisors or surgeons in the informal sector (Peltzer, 2009). Before traditional surgeons and nurses, already accustomed to performing male circumcision, could help meet the demand for male circumcision they would need to receive more training and regulation on how to perform the procedure more safely. Medical and traditional circumcision services could work together. According to the Clearinghouse on Male Circumcision (2009) “Traditional and clinical providers can collaborate to improve the safety and acceptability of circumcision, reduce complications, enhance the health education content of civic education and rituals, and improve the sexual and reproductive health of men and women, while preserving the socio-cultural importance of the circumcision process. Examples of such collaboration include: Training traditional providers in anatomy, aseptic technique, control of blood loss and wound closure; Ensuring supply of necessary instruments and dressings to reduce complications from circumcision; Cooperating on the information provided and training given to circumcision initiates to maximise good health outcomes for the participants and their current or future partners and family members; Ensuring a smooth and rapid transfer to, or intervention by, clinical services if a medical complication associated with the circumcision arises; Developing models by which clinical and traditional providers can cooperate and share responsibility for the tasks involved in the circumcision process, while respecting the different skills that each contributes; and Understanding more about the cultural and social significance of circumcisions performed by traditional providers according to the setting and age of the initiate.” ConclusionDespite a one week long training and the provision of surgical equipments and other materials to traditional surgeons a number of adverse events including the use of one instrument on more than one initiate were observed. Before scaling up traditional male circumcisions and/or integrating traditional male circumcision into medical male circumcision services in South Africa, a careful strategy to minimize unnecessary morbidity, and fundamental improvements on current traditional male circumcision techniques, are required. In addition, implementation or /and enforcement of legislation (the Mpumalanga Ingoma Bill, Mpumalanga Provincial Legislature, 2006) and control of traditional male circumcision in Gauteng province, where the study took place, are recommended to prevent adverse events to happen. Competing interests The authors declare that they have no competing interests. AcknowledgementWe thank Emseni trust for funding this study, and we thank the traditional surgeons and initiates for participating in the study. References
Copyright 2010 - Afr. J. Trad. CAM The following images related to this document are available:Photo images[tc10023t2.jpg] [tc10023t1.jpg] [tc10023appendix1.jpg] |
| |||||||||

{kind=link}
{kind=link}