 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Traditional, Complementary and Alternative Medicines, Vol. 7, No. 3, 2010, pp. 219-224 Research Paper ARE BIOMEDICINE HEALTH PRACTITIONERS READY TO COLLABORATE WITH TRADITIONAL HEALTH PRACTITIONERS IN HIV AND AIDS CARE IN TUTUME SUB DISTRICT OF BOTSWANA Sphiwe E. MadibaSchool of Public health,University of Limpopo, Medunsa Campus, South Africa
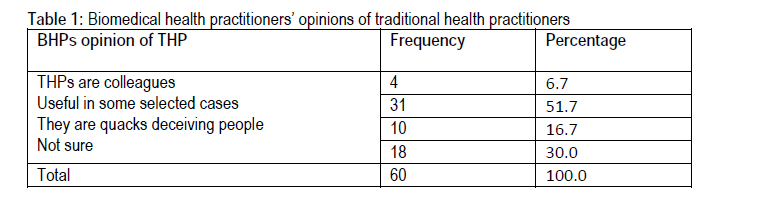
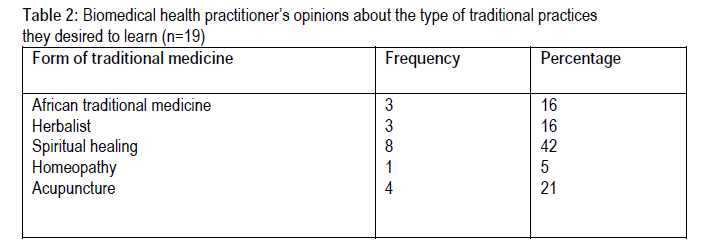
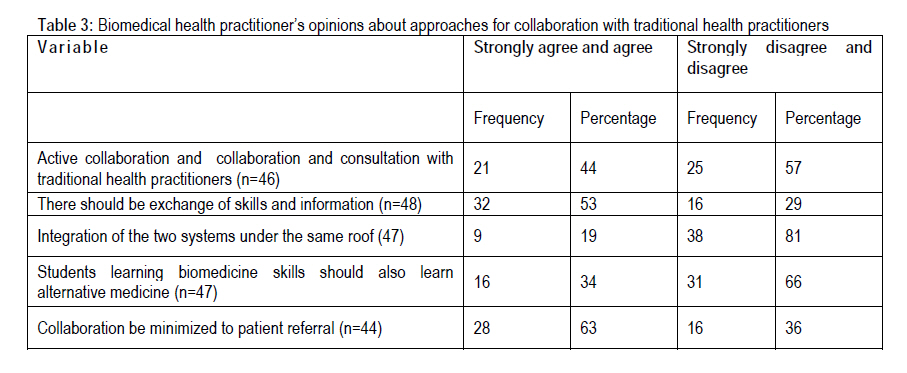
Code Number: tc10031 Abstract The aim of this study was to determine BHPs’ views on collaboration with THPs in Tutume sub district, identify collaboration activities that have been going on and determine approaches to collaboration that are acceptable to BHPs. A cross sectional survey was conducted with a convenient sample of 60 biomedicine health practitioners. The sample was drawn from two primary hospitals and clinics in Tutume Sub-District, Botswana. A pre-tested self administered questionnaire with open-and closed ended questions was used to obtain information. Majority of BHPs were in favour of collaboration despite the low levels of collaboration with THPs and low levels of awareness of the policy on collaboration. Patient referral was the preferred approach to collaboration but majority of BHPs would not refer patients to THPs. Despite the fact that BHPs were not familiar with most traditional practices they were of the opinion that they will not learn anything from THPs but were favourable towards exchange of information and biomedical skills. We conclude that BHPs were not ready to collaborate with THPs in HIV and AIDS care. BHPs wanted collaboration to be on their terms i.e. they prefer the collaboration to be limited to one way referrals from TPHs to BHPs, they will teach THPs but they were not willing to learn from them and they had negative opinions of the traditional health practice. Therefore, lack of specific guidelines on collaboration negatively affected collaborative efforts in the sub-district. IntroductionIn Sub-Saharan Africa, traditional health practitioners (THPs) far outnumber biomedicine health practitioners (BHP), it is estimated that one BHP treats about 20,000 patients while one THP treats about 400 patients (UNAIDS, 2002; WHO, 2002; Burnett et al., 1999; Holmsy and King, 1996). Given WHO‘s estimation that about 80% of the population throughout Africa relies primarily on traditional medicine for their primary health-care needs, and that patients consult both BHPs and THPs for HIV care. It is therefore crucial and rational to consider THPs as partners in the expanded response to HIV and AIDS (Kayombo et al., 2007; Homsy et al., 2004a ; UNAIDS, 2002). However, an effective response to the HIV and AIDS epidemic require renewed and refocused interest in collaboration between BHPs and THPs (Kaboru et al., 2006a). Much more can be achieved in the fight against HIV and AIDS if BHPs recognizes THPs as part of the same team. It is further argued that collaboration with THPs has a potential of fostering value and respect of the contributions of THPs in the prevention of HIV and AIDS and also increase resources for HIV and AIDS prevention (Mngqundaniso and Peltzer, 2008; Burnett et al., 1999). Effective collaboration represented by skilled THPs linked to referral facilities could create a complementary HIV and AIDS care system that will be of great benefit to patients and communities (Kayombo et al., 2007; Homsy et al., 2004a; King and Homsy, 1997). The World Health Organisation’s recommendation for the inclusion of traditional medicine in national responses to HIV and AIDS (WHO, 1990) has resulted in the initiation of collaborative HIV and AIDS programmes in a number of sub-Saharan countries including Botswana (UNAIDS, 2002; King and Homsy, 1997). It has been the policy of the Botswana government to actively promote collaboration and co-operation between THPs and BHPs since 1980, the government through the National Health Policy encourages and promotes active collaboration between the BHPs and THPs (Chipfakacha, 1997). The policy states that the government would promote and foster mutual respect between the two sides and facilitate and maintain dialogue (Botswana Health Policy, 1995). The policy initiative culminated in workshops and seminars on HIV and AIDS and the training of traditional healers as trainers who would pass HIV and AIDS information to other THPs thus further promote collaboration (UNAIDS, 2000; Chipfakacha, 1997). A decade after the policy initiatives, anecdotal evidence suggests that there are insignificant activities countrywide concerning collaboration and there has not been much documentation of how the collaboration has unfolded nationally and in the different health districts thus far. This is in contrast with other African countries like South Africa (Pinkoane, 2008; Peltzer and Khoza, 2002; Peltzer, 2001; Peu et al., 2001), Swaziland (Upvall, 1992), Malawi (Chipolombwe and Muula, 2005), Zambia (Kaboru et al., 2006a; Burnettet et al. , 1999) and Tanzania (Kayombo et al., 2007) were reviews on collaborative were conducted with BHPs Lack of documentation of collaboration attempts appear to be a general problem for most sub-saharan countries, according to Kaboru et al. (2006a), there is lack of systematic description of the experiences of and attitudes towards collaboration among THPs and BHPs. There is also a general consensus among researchers that where documentation on collaboration occur, studies often describe and document THPs eagerness to collaborate with and learn from BHPs while the BHPs' views are left out (Kaboru et al., 2006b; UNAIDS, 2000, 2006). The aim of this study was to determine BHPs’ views on collaboration with THPs in Tutume sub district. Collaboration in this paper is taken as measures aimed at enhancing understanding between the two forms of health practitioners with active interaction in form of consultative meetings, seminars and workshops for mutual learning; and referrals from THPs and referrals to THPs by BHPs, as enshrined in the National Health Policy of Botswana (Health Policy, 1995). TPHs in the context of Botswana refers to all types of traditional healers, including herbalists, spiritual healers, bone setters, acupuncture, Ayurvedic medicine, traditional birth attendants, and chiropractors (Unaids 2000, 2006) Materials and methodsA cross-sectional survey was conducted with a convenient sample of 60 BHPs during October 2006. The sample was drawn from two primary hospitals and 7 clinics in Tutume, one of the sub- district of the central district in Botswana. The population size of Tutume is about 123,514 people while the two primary hospitals serve about 78 738 people (Census 2001). The convenience sample comprised of BHP available in the health facilities on the days of the survey. In this study BHPs comprised of nurses, doctors, laboratory technicians, pharmacists and pharmacy technicians. A pre-tested questionnaire was self-administered by respondents. This questionnaire comprising open- and closed-ended questions was used to obtain information on their socio-demographic profile, the questionnaire further obtained information on the following aspects of BHPs interaction with THPs: the form and frequency of interaction activities in the past year; awareness of the National Health Policy on collaboration with traditional healers; familiarity with the types of alternative medicine practiced in the district; types of traditional and alternative medicine they desired to learn; whether they would refer patients to THPs, their views on collaboration with THPs, preferred approaches to collaboration and the popularity of THPs among their patients. A trained field worker delivered the questionnaires and consent forms to BHPs in each health facility. BPHs were informed about the study by the data collector who first explained the study and if they volunteered to participate, they would then sign an informed consent form. The completed questionnaires were collected by the field worker at the end of the day. The study was approved by the National School of Public Health Research, Ethics and Publication Committee of the University of Limpopo (Clearance no NSPH/ST/2006/23), while the Botswana Ministry of Health gave permission to conduct the study. ResultsThe response rate from biomedicine health practitioners was 100%. Of the BHPs who completed the survey, 36(60%) were female and 24 (40%) male and their ages ranged from 25 to 50 years. BHPs comprised of 42 (70%) nurses, 5 (5, 8%) medical practitioners, 5 (5, 8%) pharmacists, 7 (12%) were laboratory staff, and only 1 (2%) was a social worker. The demographic profile of BHPs in the study sample is consistent with the distribution of health care practitioners in the country; there are more nurses than any other professional category. BHPs’interaction with THPsOnly 11 (18.6%) of the BHPs were aware of the Ministry of Health’s policy on collaboration with THPs in HIV and AIDS care, 50% of BHPs stated that THPs were popular among their patients, while 66% acknowledged that their patients consulted THPs before coming to them. When asked about whether BHPs had ever interacted with THPs in the past year, 43 (73%) reported having never interacted with BHPs. Attending seminars or workshops was reported as the most common form of collaboration by 56% of BHPs who had interacted with THPs, but only 6 (11%) reported attending collaborative workshops more than twice a year. BHPs opinions on collaborationWe asked BHPs about their opinions on collaboration, of the 55 who responded, 44 (80%) were in favour of collaboration between the two disciplines. Despite the fact that BHPs reported that they will collaborate with THPs, collaboration will be only for the sake of patients. BHPs additionally reported that THPs might learn safer ways of managing patients from the BHPs. About 11(20%) of BHPs were not in favour of collaboration, the main reason cited was that the two disciplines were unrelated and they (BHPs) were also concerned with toxicities, morbidities and mortalities from traditional medicines BHPs’opinions about THPsTable1 shows the responses of BHPs on their opinions of THPs. We asked BHPs about their opinion of THPs and more than half thought THPs were useful in selected cases, it is to be noted that a small proportion (17%) thought THPs were quacks who were deceiving people. We asked whether BHPs had any desire to learn any form of alternative medicine and of the 59 who responded, 20 (34%) reported having a desire to learn from THPs, while 39 (66%) had no desire to learn from THPs what so ever. Table 2 shows the type of alternative medicine BHPs desired to learn Opinions about approaches for collaboration The table below shows BHPs opinions about suggested approaches to collaboration with THPs. The two commonly preferred approaches to collaboration was patient referral (66%) and exchange of skills and information (65%). Though patient referral was the preferred approach to collaboration, when BHPs were asked if they would refer a patient to THPs, 52 (90%) reported that they would not refer patients to THPs. In particular, all the medical practitioners in the sample said they would not refer patients to THPs. DiscussionThe study findings showed low levels of collaboration between the BHPs and THPs, and that 73% of BHPs have never interacted with THPs. This is despite the government of Botswana’s policy initiatives, strategy and processes for collaboration between the two disciplines. Collaboration between BHPs and THPs was also documented to be low in a study conducted with THPs and BHPs in Zambia, where only 24 % of BHPs reported having contacts with the THPs six months prior to the study (Kaboru et al, 2006b). In Botswana the basis of collaboration between BHPs and THPs is the 1995 health policy on collaboration with traditional medicine practitioners, nevertheless the policy does not specify when and how often the two sides should meet, leaving the responsibility to initiate and facilitate meetings and workshops to the biomedical institutions. Based on this data, we can deduce that the lack of specific guidelines on collaboration has negatively affected the collaboration efforts in the sub district, where only 19% of BHPs were aware of the policy on collaboration with traditional health practitioners and only 27% reporting to ever interacted with THPs, and only 28% to ever attended collaboration workshops in the past year. Similar findings of low interaction between BHPs and THPs were documented in other studies conducted in the country by Motswagole (1993) and Lejowa (1993). The purpose of the policy on collaboration was to promote and foster mutual respect and also facilitate dialogue between BHPs and THPs. Findings from this study suggest that this has not been the case, the findings revealed low interest in alternative medicine by BHPs with 70% having no interest in any form of traditional medicine. Even though these were small proportions of BHPs, it is disturbing that they still had negative opinions of the traditional health practice; they were of the opinion that THPs were quacks who were deceiving people and that the law should be used to stop THPs practice. Kayombo et al. (2007) reported that BHPs especially physicians down play THPs despite their proven popularity and usefulness. This was the case in this study where about half of the BHPs were of the opinion that THPs were not popular among their patients, despite evidence that THPs enjoys more popularity worldwide than BHPs (Kayombo et al., 2007; Peltzer et al., 2006; Homsy et al., 2004a; UNAIDS, 2002; Chipfakacha, 1997). BHPs opinions on collaborationThe majority (80%) of BHPs in our study was in favour of collaboration between the two disciplines; however results show that collaboration will be on the terms of the BHPs, they did not trust or believe in traditional medicine and will collaborate for the sake of the patients. In Malawi BHPs wanted collaboration so that THPs refer patients to BHPs, while others wanted collaboration so as to educate THPs on the dangers of their medicine (Chipolombwe and Muula, 2005). In our study BHPs were willing to collaborate so that THPs might learn safer ways of managing patients from them. Nevertheless, our findings are contrary to findings by Addis (2002) in Ethiopia, where majority 86% of BHPs and THPs were in favor of collaboration, the findings further showed mutual respect and recognition among BHPs and THPs. While BHPs in this study were favourable towards exchange of information and biomedical skills, they were less willing to learn traditional medicine skills. Kayombo et al. (2007) reported similar attitude from BHPs who often dominate the collaboration process, resulting with THPs receiving training from BHPs, rather than the two groups learning together and from each other. This was also the case in Malawi where Chipolombwe and Muula (2005) reported a tendency of BHPs to consider themselves superior to the THPs. According to Kaboru et al. (2006b), BHPs in favour of collaboration were of the opinion that collaboration is possible only if it is well designed, while acknowledging that collaboration with THPs is not easy but require nurturing of the process (Kayombo et al., 2007; Kaboru et al., 2006a). One of the key elements recommended for successful collaboration is building mutual respect between BHPs and THPs through dialogue, consistent exchange of information and eagerness to learn from one another (King, 2005). Given the above, it is imperative that BHPs and THPs learn from each other for successful collaboration, therefore the findings from our study suggests that the low level of collaboration could be attributed to the lack of desire to learn from THPs by the BHPs. Opinions about approaches for collaborationIn spite of the fact that patient referral was the preferred collaborative approach, 90% of BHPs were not willing to refer patients to THPs, referral as a collaboration approach was seen as a way of encouraging patient referral from THPs to BHPs. The results show that the most common reasons for not referring to THPs were concerns with toxicities, morbidities and mortalities resulting from traditional medicines. Kaboru, et al. (2006b) reported various reasons for poor referral between BHPs and THPs; most of the reasons documented were associated with lack of belief in THPs, in addition lack of referral guidelines was also reported as a reason for not referring to THPs. While lack of referral guidelines was not mentioned as a reason for not referring to THPs in this study, it might be a barrier to collaboration, given the lack of specific guidelines on collaboration in the country. ConclusionIf the health policy of Botswana describes collaboration as measures aimed at enhancing understanding between BHPs and THPs with active interaction in the form of meetings, referrals, and other activities, given the findings of the study, we conclude that BHPs are not ready to collaborate. While the majority of BHPs are in favour of collaboration with THPs in HIV and AIDS care, the description of collaboration as enshrined in the health policy of the country is not actualized. This is also true of the key conditions for collaboration as set out by King (2005). In the current study BHPs wanted to collaborate on their terms i.e. they prefer the collaboration to be limited to one way referrals from TPHs to BHPs, they will teach THPs but they were not willing to learn from them and they had negative opinions of the traditional health practice. We also conclude that the lack of specific guidelines on collaboration has negatively affected the collaboration efforts in the sub district; this is evident by low levels of interaction between BHPs and THPs. References
Copyright 2010 - Afr. J. Trad. CAM The following images related to this document are available:Photo images[tc10031t1.jpg] [tc10031t3.jpg] [tc10031t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}