 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
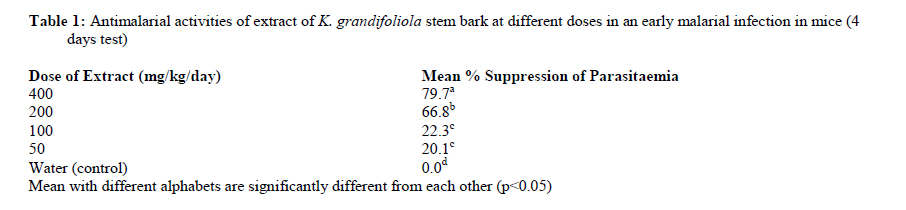
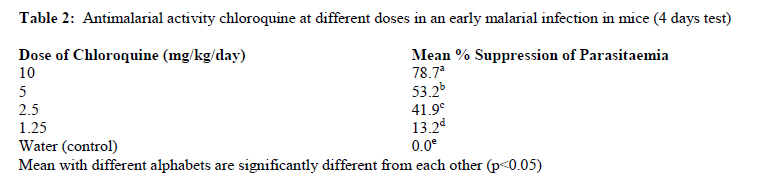
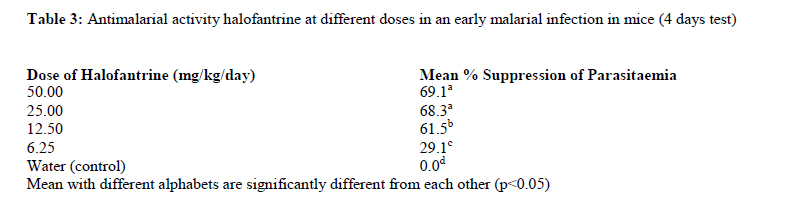
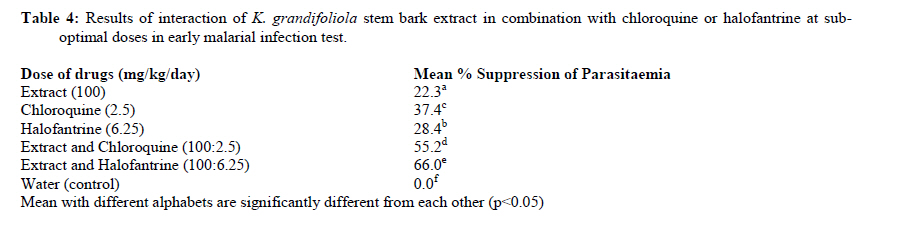
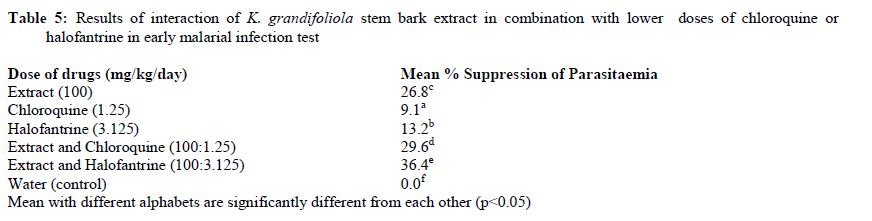
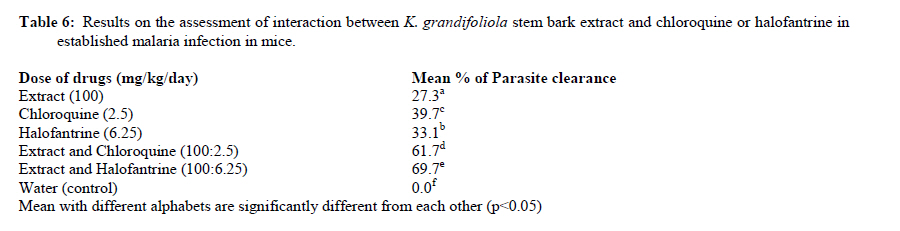
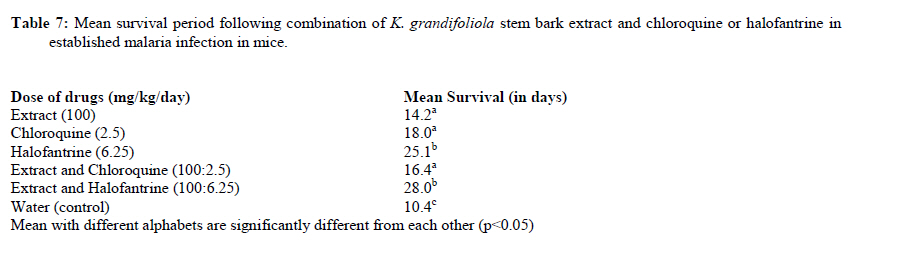
African Journal of Traditional, Complementary and Alternative Medicines, Vol. 7, No. 4, 2010, pp. 370-376 Chemotherapeutic Interaction Between Khaya Grandifoliola (Welw) Cdc Stem Bark Extract And Two Anti-Malarial Drugs In MiceSteve O. Ijarotimi1, Joseph M. Agbedahunsi*1, Cyprian O. Onyeji 2 and Clement O. Adewunmi1 1.Drug Research and Production Unit 2Department of Pharmaceutical Chemistry Faculty of Pharmacy, Obafemi Awolowo University, Ile-Ife, Nigeria * E-mail: jagbedah@oauife.edu.ng / foluagbedahunsi@yahoo.com Code Number: tc10050 Abstract In malarial endemic countries especially in the tropics, conventional antimalarial drugs are used with herbal remedies either concurrently or successively. Khaya grandifoliola is one of such popular herbs used in the treatment of malaria. Various doses of ethanol extract of K. grandifoliola stem bark (50-400 mg/kg/day) were administered orally to Swiss albino mice infected with Plasmodium yoelii nigerense. A dose of 100 mg/kg/day of the extract was also combined with 2.5 mg/kg/day of chloroquine or 6.25 mg/kg/day of halofantrine in both early and established malaria infection test models. The results showed that in the early malaria infection test, K. grandifoliola in combination with chloroquine or halofantrine elicited enhanced antiplasmodial effect in the established infection, there was significantly greater parasite clearance following administration of the combination when compared to the effects of K. grandifoliola or the conventional drugs alone. The mean survival period of parasitized animals was also enhanced by the extract/halofantrine combination. Lower therapeutic doses of halofantrine may be required to potentiate parasite clearance when used in combination with K. grandifoliola. This may constitute great advantage to halofantrine which is associated with cardiotoxicity at high doses. Key words: Khaya grandifoliola, Antimalarial, Chemotherapeutic interaction, Chloroquine, Halofantrine IntroductionAntimalarial drug resistance is one of the greatest challenges of malaria therapy. Resistance accounts for recrudescence and severity of infections in some parts of the world (Peters, 1982). Many commonly used antimalarial drugs are chemically related such that development of resistance to one drug can result in resistance to others. For example, crossresistance between the 4-aminoquinolines, chloroquine and amodiaquine, has been reported (Bloland, 2001) as a result of ineffectiveness of commonly used antimalarial drugs, the use of alternative medicine either exclusively or along with conventional medicines has becomes common feature. This situation is prevalent in developing tropical countries where modern medicines are not affordable to a majority of the rural populations (Kremsner and Kritna, 2004). Up to 80% of African population use traditional medicine especially plant remedies in the management of diseases including malaria (WHO, 2002). Often, antimalarial herbal therapies are used concurrently, prior or after the use of conventional antimalarial drugs in West Africa. Very few reports are available on the interaction of herbal anti-malarial products with synthetic drugs. One of such reports indicates that some local African populations use herbal products in combination with chloroquine for enhancement of activity (Rasoanaivo et al. 1998). Either of pharmacodynamic or pharmacokinetic interactions can result in synergism, additivity or antagonism. It is therefore most desirable to evaluate the interaction between common herbs used in the management of malaria and some of the conventional antimalarial drugs. More so, the use of combination of two or more drugs as a way of delaying or overcoming development of drug resistance is topical in malarial chemotherapy research (WHO, 2000). Combination of Artemisinin derivatives with other antimalarial drugs has become a standard practice in malaria chemotherapy. Antimalarial combination chemotherapy is widely advocated because combination therapies can increase efficacy, shorten duration of treatment hence improve compliance in addition to reduction in the risk of resistant parasites arising through mutation during therapy (WHO, 2001). Aqueous decoction of K. grandifoliola (Benin Mahogany or timber) is commonly used by traditional medical practitioners in West Africa in the management of malaria. This plant has been scientifically evaluated for its anti-malarial activity (Makinde et al 1989; Agbedahunsi et al, 1998), anti-inflammatory and toxic effects (Agbedahunsi et al, 2004), effects on red blood cells and bone mineral content in rats (Bumah et al, 2005a) and on some biochemical parameters in rats (Bumah et al, 2005b). A bicyclo (3, 3, 1) nonane derivative of phragmaline named grandifolioline, has been isolated from the anti-malarial fraction of this plant by Agbedahunsi et al. (1998). The present study evaluates the in vivo antimalarial activities of aqueous extract of the plant alone and in combination with two commonly available anti-malarial drugs (chloroquine and halofantrine) against rodent malaria parasite in mice Materials and Methods Animals and Parasite Swiss Albino mice (male and female) of weight range of 18 to 22 g were used for this study. The animals were obtained from Central Animal House, University of Ibadan, Ibadan, Oyo State, Nigeria and were kept in well ventilated animal house in the Faculty of Pharmacy Obafemi Awolowo University Ile-Ife. The animals were allowed to acclimatize for 7 days prior to the commencement of the experiment, kept at normal room temperature in a group of five per cage. They all received animal chow and water ad libitum throughout the duration of the experiment. The “Principle of Laboratory Animal Care” (NIH publication No 85-23) guidelines and procedures were followed in the study (NIH publication. 1985). Rodent Plasmodium yoelii nigerense (chloroquine resistant strain) obtained from the National Institute of Medical Research, Lagos, Nigeria, was used to inoculate the animals. Collection, Preparation and Extraction of the stem bark of K. grandifoliolaThe stem bark of K. grandifoliola was collected at Igasi village near Ikare Akoko, Ondo State, Nigeria in January 2005 by Mr A. Akanle. Specimen of the stem bark was authenticated by Dr. C. Illoh of Botany Department, Obafemi Awolowo University, Ile Ife, Nigeria. A herbarium specimen with voucher specimen number IFE 15320 was deposited at the University herbarium located in the Botany department. The barks were chopped, dried in an oven for 48 hours at 60 oC and then powdered using a grinding machine (Christy Norris, UK). The powder was kept in a well closed, amber-coloured bottle until when needed. K. grandifoliola stem bark powder (600 g) was extracted with 50% aqueous ethanol in a Soxhlet extractor for 72 hr. The resulting extract was concentrated in vacuo to reduce the volume and finally freeze dried using an Edward Pirani 10 lyophylizer, UK. The dried powder extract was then stored in well sealed amber bottle for further analyses. In vivo antimalarial studies using the early malarial infection model Assessment of Antimalarial actions of K. grandifoliola, chloroquine and halofantrineThe early malarial infection test according to Peters et al (1975) as modified by Makinde et al (1989) was used. Sixty five Swiss Albino mice were divided into 13 sub groups (n=5). Group A consisted of four sub-groups. Each sub-group separately received different doses of K. grandifoliola stem bark extract at the doses of 50, 100, 200 and 400 mg/kg body weight/day Group B consisted of four such groups. Each sub group received different doses of halofantrine at 6.25, 12.5, 25.0 and 50.0 mg/kg /day. Group C also consisted of four sub groups. Each sub group received separately different doses of chloroquine at 1.25, 2.5,5 and 10 mg/kg/day Group D consisted of a single group of five mice. This served as the control group. The mice in this group received 0.2 ml distilled water. All the mice tested received standard inoculums of 1 x 107 chloroquine resistant Plasmodium yoelii nigerense infected erythrocytes by intraperitoneal (I.P) route at the commencement of the experiment. Single oral doses of the test drugs or extract were administered to the animals 3 hr after each inoculum’s for four consecutive days. On the fifth day, tip of each mouse was cut with sharp dissecting scissors to withdraw drops of blood from the animal’s tail onto scratch free slides, stained with Giemsa stain and examined microscopically. The level of parasitaemia (%) was evaluated from the equation: Total number of PRBC X 100 Where PRBC: Parasitized red blood cells; RBC: Red blood cells. Assessment of antimalarial effects of K. grandifoliola stem bark extract in combination with chloroquine or halofantrineThirty mice were divided into six groups (n=5). The experiment was carried out as described above. Mice in Group E received 100 mg/kg body weight/day of the ethanol extract; Thin films of blood from the mice were prepared on the fifth day after inoculation with the P. yoelii nigerense and the percentage parasitaemia determined as described above. Assessment of interaction of K. grandifoliola stems bark extract in combination with low doses of chloroquine and halofantrineThirty mice were divided into six groups (K to P, n=5) and the experiment was executed as described above but with lower doses of chloroquine and halofantrine in the combination treatments. Group K mice received 100 mg/kg/day dose of the extract alone Mice in group O received extract/halofantrine mixture in combination dose of 100:3.125 mg/kg /day Mice in group P served as the control, they received 0.2 ml water. Assessment of percentage parasitaemia was as described above. In vivo antimalarial experiments using the established malarial infection model Assessment of interaction between K. grandifoliola stem bark extract and chloroquine or halofantrine A modified Ryley and Peters (1970) method was used. Thirty mice were divided into six groups (Q-V, n=5). Each mouse was inoculated with 1x107 Plasmodium yoelii nigerense infected erythrocytes on the first day of the experiment (Day 1). The mice were not treated until the parasitaemia was developed and established. On day 4, (72 hr after inoculation), the mice were treated orally with the extract and the drug, singly and in combinations. Group Q mice received 100 mg/kg /day) of the extract. All the animals were treated daily for five days and were assessed daily for the five days of treatment. On each day of the assessment, percentage parasitaemia and percentage parasite clearance for each of the mice relative to the control was determined. The percentage suppression of parasitaemia and parasite clearance for the plant extract and/or drug treatments were calculated as follows: [(Mean % parasitaemia in the negative control group – Mean % parasitaemia in the tested group) / Mean % parasitaemia in the negative control group] x 100 After the five days of drug and/or extract administration, the mice were observed till day 28. Any death that occurred during this period was noted and the mean survival time was determined. Data and Statistical analysisThe data were as analyzed using Statistical package for Social Scientists (SPSS) version 12 computer software. Level of significant differences between the groups receiving different treatments was determined using one-way ANOVA followed by Duncan multiple range test. P < 0.05 was considered significant. ResultsEffects of various doses of the extract of K. gradifoliola, chloroquine and halofantrine on P. yeolii nigerense when administered separately in the early malarial infection tests are presented in Tables 1, 2 and 3, respectively. The percentage chemosuppression was dose-dependent. The highest dosages of the extract and the conventional drugs gave about 70 percent chemosuppression. K. grandifoliola at 400 mg/ kg /day gave 79.9%, while chloroquine at 10 mg/kg body weight / day and halofantrine at 50 mg/kg body weight/day resulted in 78.8 % and 69.1% chemosuppression, respectively. Based on these results, the sub optimal doses were obtained for the extract and the conventional drugs. Dose of K. gradiofoliola extract (100 mg/ kg /day) gave 22.3 % suppression of parasitaemia. The sub-optimal dose for chloroquine was found to be 2.5 mg/kg body weight/day (41.9%) while halofantrine at 6.25mg/kg/body weight/day had 29.1 % (Tables 1, 2 and 3) These sub-optimal doses were used to assess the interaction of K. grandifoliola stem bark with the conventional antimalarial drugs in subsequent combination treatments. Table 4 shows the results of the combination treatments of K. grandifoliola stem bark extract with conventional drugs at sub-optimal doses using the early malarial infection test model. Extract/ chloroquine combination resulted in 55.2% suppression, while extract/halofantrine combination gave 66% suppression. The results of the combination studies at low dosages of the conventional drugs are presented in Table 5. Half the sub-optimal doses of chloroquine (1.25 mg/kg /day) and halofantrine (3.13 mg/kg /day) were used in combination with the sub-optimal dose of K. grandifoliola ethanol extract (100 mg/ kg /day). The suppression for the extract/chloroquine combination was 29.6% and 36.4% for the extract/halofantrine combination. The interaction of the ethanol extract with Chloroquine and halofantrine drugs were assessed for parasite clearance when the parasites were already established in the mice at sub-optimal dose levels and the results was presented in Table 6. There were significant increases in percentage clearance for the extract/chloroquine and extract/halofantrine compared to the effects of the drugs or extract given separately. As part of the established infection test, the mean survival period of the parasitized mice treated with the drugs singly or in combination were determined and presented in Table 7. Discussion The stem bark of K. grandifoliola is widely used as decoction by traditional healers in Nigeria however some traditional healers soak the stem bark along with some other herbs with dilute ethanol to manage febrile conditions. As such 50 percent ethanol / water (v/v) was used as extraction solvent. Beside, ethanol being an organic solvent should possess better extractive capability than water (inorganic polar solvent) to extract the putative organic material. The adult human therapeutic dose for chloroquine and halofantrine in the management of malaria are 10 mg/kg and 50 mg/kg respectively. Based on this fact two fold serial dilution of 10mg/ kg i.e. (5, 2.5 and 1.25) mg/kg was prepared and used for chloroquine while 25, 12.5 and 6.25 mg/kg doses were used for halofantrine respectively. Based on these concentrations sub-optimal doses were determined for the two drugs. Sub-optimal doses were chosen as doses that produced less than 50% suppression or parasite clearance in the early malarial infection or established malarial infection respectively. The spread of malaria parasite resistance to commonly available antimalarial drugs especially the monotherapeutic drugs such as chloroquine, amodiaquine, halofantrine etc is posing increasing problems for the provision of suitable treatment of malaria. This has resulted in high level of malaria treatment failure which serves as one of the basis for the replacement of firstline treatment. Resistance has emerged to all classes of antimalarial drugs including artemisinine and its derivatives (WHO, 2003a). Combination therapy (CT) which enhances efficacy and reduces the emergence of resistant parasite strains is now recommended (WHO, 2003a; White 2004; WHO, 2006). This entails the simultaneous use of two or more blood schizontocidal drugs with independent modes of action and different biochemical targets in the parasite (WHO, 2006). CT can be fixed therapy in which the components of the drugs are co-formulated or multi-drug therapy in which the components are co-administered separately. CT could lengthen the effective life span of chemotherapeutic agents by reducing the chances of emergence of resistant mutants (WHO, 2003a). Chemotherapeutic interaction studies involving the combination therapy have been used to evaluate compounds in the management of malaria (Price et al, 1996; Attaran et al, 2004). A dose-dependent suppression of parasitaemia was observed in the extract and the standard drugs tested (Tables 1, 2 and 3). However, increase in halofantrine dosage up to 50 mg/kg/day resulted in marginal activity which implied that absorption of halofantrine has a maximum limit dose (25 mg/kg/day) in this experiment (Table 3). This result confirmed the findings of Karbwang and Na Bangchang, 1994 wherein it was reported that due to halofantrine poor aqueous solubility, its absorption after oral administration even after increasing drug doses was limited. The effect of combination of the extract with halofantrine at sub-optimal dose levels in both early malaria infection and the established infection models showed that the effect of the combination was higher than the sum of the effects of the extract and halofantrine acting separately (Tables 4 and 6). Thus, parasite suppression and clearance for K. grandifoliola/halofantrine combination (100:6.25 mg/kg body weight/day) were significantly higher (p<0.05) when compared to the sum of the effect of the extract and halofantrine separately. These observations tend to suggest a synergistic interaction between the extract and halofantrine. On the other hand, the effects of combination of the extract with chloroquine in both infection models were indicative of additive interaction since the effects of the combination were comparable to sum of the separate effects of the extract and chloroquine. At very low doses of the conventional drugs (chloroquine 1.25, and halofantrine, 3.13 mg/kg body weight/ day), the suppression of parasitaemia was equally very low. Additive effect was still observed at these low doses in the extract/halofantrine combination. The increase in percentage suppression in the extract/chloroquine combination was just marginal. In spite of these low values, the differences were still significant (p< 0.05) which is an evidence of the effect of the interaction (Table 5). Results of mean survival period do not parallel those of parasite clearance. For example, the mean survival period of the extract/chloroquine combination was not significantly different from the survival period of animals treated with chloroquine or extract alone (Table 7) inspite of the significant increase (p<0.05) in the parasite clearance due to the combination (Table 6). In a study by Nwafor et al. (2003), it was reported that concomitant administration of chloroquine sulphate and aqueous extract of Azadirachta indica impaired the bioavailability of chloroquine resulting in antagonist effect between chloroquine and the plant extract. A .indica and K. grandifoliola belong to the Meliaceae family and contain similar constituents limonoids. The decrease in the mean survival period of the extract/chloroquine combination could be due to this bioavailability theory or otherwise. Therefore, further studies are required to verify the toxicological implications of combinations of K. grandifoliola with chloroquine or halofantrine In this study, it was observed that chemosuppresion or parasite clearance in the early or established infection tests respectively was below 80%. This is due to the resistant strain of the parasite used for the study. In spite of this observation the K. grandifoliola/ halofantrine combination ensured survival of all the infected animals throughout the 28 days of the experiment. ConclusionIn response to wide spread multidrug resistance of malaria parasites to monotherapies, this study shows that K. grandifoliola bark extract in combination with halofantrine is associated with enhanced efficacy. The combination with halofantrine resulted in 100 % survival of the infected animals throughout the 28 days of study in the established antimalarial infection test. This study underscores possible merits in combining conventional antimalarial drugs with herbal remedies. Acknowledgment The authors are grateful to the Third World Academy of Science (TWAS) for providing the research grant (RGA) No. 07-020 LDC/ BIO/AF/AC-UNESCO FR: 3240144813 to the Drug Research and Production Unit; part of which was used in this research that led to the award of M.Sc degree in Phytomedicines of the Obafemi Awolowo University, Ile-Ife, Nigeria to Mr. S.O. Ijarotimi. References
Copyright 2010 - Afr. J. Trad. CAM The following images related to this document are available:Photo images[tc10050t7.jpg] [tc10050t6.jpg] [tc10050t5.jpg] [tc10050t3.jpg] [tc10050t1.jpg] [tc10050t4.jpg] [tc10050t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}