 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
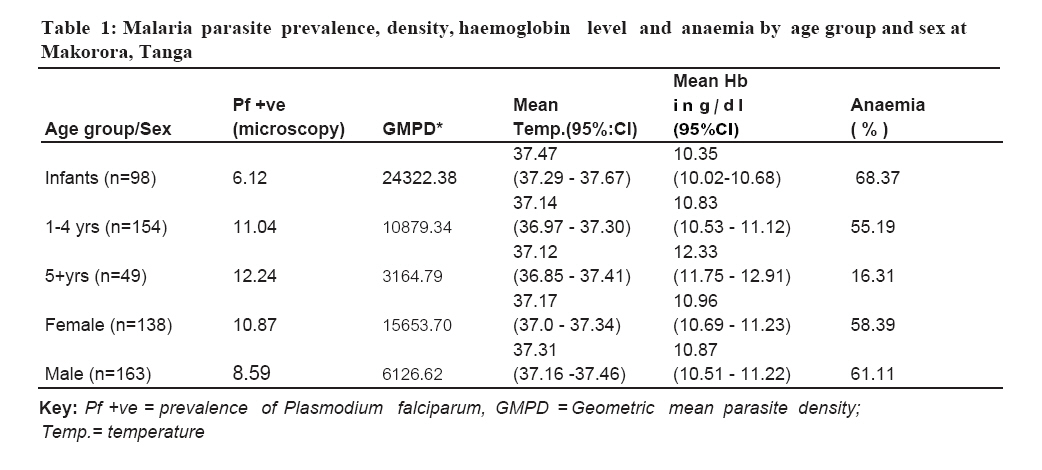
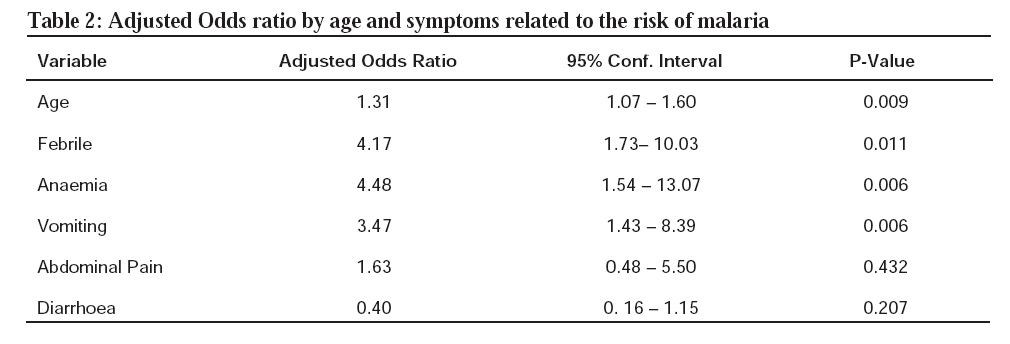
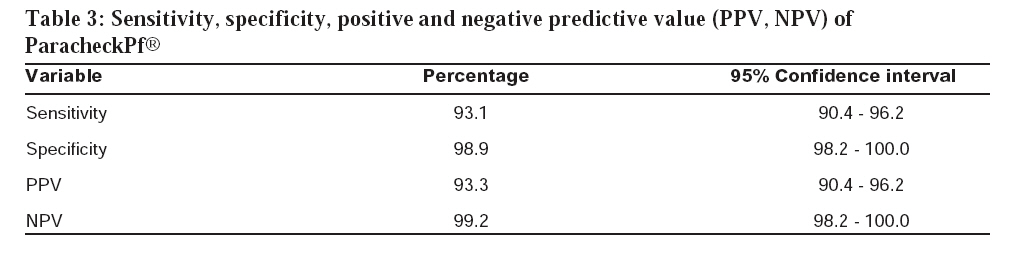
Tanzania Journal of Health Research, Vol. 10, No. 1, January, 2008, pp. 14-19 Paracheck Pf® compared with microscopy for diagnosis of Plasmodium falciparum malaria among children in Tanga City, north-eastern Tanzania M.L. KAMUGISHA12*, H. MSANGENI1, E. BEALE2, E.K. MALECELA1, J. AKIDA, D.R.S ISHENGOMA1 and M.M. LEMNGE1 1National Institute for Medical Research, Tanga Medical Research Centre, P.O. Box 5004, Tanga, Tanzania 2Morehouse College, Atlanta, Georgia, United States Received 21 December 2006 Revised 12 December 2007 Accepted 13 December 2007 Code Number: th08004 Abstract Malaria is a major public health problem particularly in rural Sub-Saharan Africa. In most urban areas, malaria transmission intensity is low thus monitoring trends using reliable tools is crucial to provide vital information for future management of the disease. Rapid diagnostic tests (RDT) such as Paracheck Pf® are now increasingly adopted for Plasmodium falciparum malaria diagnosis and are advantageous and cost effective alternative to microscopy. This cross sectional survey was carried out during June 2005 to determine the prevalence of malaria in an urban setting and compare microscopy diagnosis versus Paracheck Pf® for detecting Plasmodium falciparum. Blood samples from a total of 301 children (<10 years) attending outpatient clinic at Makorora Health Centre, in Tanga, Tanzania were examined for the presence of malaria. Twenty-nine (9.6%) of the children were positive to malaria by microscopy while 30 (10.0%) were positive by Paracheck® test. Three out of 30 positive cases detected by Paracheck® were negative by microscopy; thus considered to be false positive results. For the 271 Paracheck Pf ® negative cases, 2 were positive by microscopy; yielding 2 false negative results. Paracheck Pf ® sensitivity and specificity were 93.1% and 98.9%, respectively. P. falciparum was the only malarial species observed among the 29 microscopy positive cases. The prevalence of anaemia among the children was 53.16%. These findings indicate a low prevalence of malaria in Tanga City and that Paracheck Pf ® can be an effective tool for malaria diagnosis Key words: malaria, rapid diagnostic test, microscopy, anaemia, urban,Tanzania Introduction Malaria is a worldwide public health problem that continues to challenge researchers and health professionals alike. The disease affects approximately 300400 million people (6-8% of the global population) and causes 1-2 million deaths every year (Snow et al. 2006;). It accounts for 10% of all hospital admissions and 20-30% of all doctors’visits annually, worldwide (WHO, 2004). Proper management of malaria cases within the first 24 hours of onset is considered to be the best way to reduce its morbidity and mortality (Malimbo et al., 2006; Hopkins et al., 2007). This would be adequately achieved if most of the patients had access to laboratory facilities. Like in many countries in Africa (Petti et al., 2006), in most areas of Tanzania, even where health facilities are available, most of them do not provide laboratory services. In these areas, treatment of malaria and other febrile conditions is usually based on clinical symptoms and guidelines such as the Integrated Management of Childhood Illness (IMCI) (Amstrong et al., 2004). Yet the use of such guidelines without laboratory confirmation has lead to high levels of over-diagnosis and misuse of drugs (Reyburn et al., 2004, 2007). Microscopy is the golden standard diagnostic tool for malaria diagnosis in many areas of sub-Saharan Africa. However, use of microscopy requires well trained personned and capital investment in terms of equipment (Petti et al., 2006). Moreover, in cases where immediate diagnosis is necessary, microscopy is a drawback due to slightly time consuming methods involved in slide preparation and reading. In light of these, rapid diagnostic tests (RDTs) have been recommended for use in recent years (Petti et al., 2006). These tools are easy to apply and provide immediate results even at rural setting (Mboera et al., 2006a). Of the available RDTs, Paracheck Pf® has been proven advantageous due to its high reliability and low cost as compared to other RDTs (Proux et al., 2001). Para-check Pf® specifically detects P. falciparum histidine rich protein-2 (PfHRP- 2) in whole blood specimens. Only a few studies have assessed the performance of Paracheck Pf® dipstick in detecting malaria parasites in different levels of endemicity in Tanzania (Mboera et al., 2006a; Reyburn et al., 2007), and most of them involved rural population. In most urban areas of African countires malaria transmission intensity is low (Robert et al., 2003). However, with the rapid growth of towns and cities which does not match with the infrastructure, there is concern of the expansion of malaria into the urban areas. In Tanzania, only a few published studies have been carried out on urban malaria in Dar es Salaam, Dodoma and Iringa (Yamagata, 1996; Wang et al., 2006; Mboera et al., 2006b). Thus, more information on the actual burden of urban malaria in different geographical areas of the country is urgently required to accurately determine its trend and provide necessary data for planning interventions. Thus, this study was conducted to determine the level of malaria burden using Paracheck Pf® dipstick and microscopy among children clinically diagnosed with malaria and attending a healthcare facility in Tanga City, Tanzania. Materials and Methods Study site The study was conducted at Makorora Health Centre in Tanga City in north-eastern Tanzania. The City lies at about 5.170, 5.330S and 38.170, 38.33°E along the Indian Ocean. The area receives two seasons of rainfall; short rains during October – November and long rains in March–May, with relative humidity of about 100%. Temperature ranges between 270C and 320C. Tanga City covers an area of about 600km2 and has an estimated human population of 248,696. Malaria accounts for over 50% of all out-patient visits and admissions and malaria-specific deaths are estimated to be about 31% of all reported deaths (MoH, 2006). Study design and data collection A cross-sectional study was conducted for six weeks beginning the second week of June 2005. It involved a simple random cluster sample of 301 children aged ≤10 years attending Outpatient department (OPD) at the Health Centre. All the children had history and symptoms suggestive of malaria and were requested by the attending clinicians to be tested for malaria. The study was explained to children parents or caretakers and an oral consent was obtained before enrolment in the study. Following examination, results were communicated to the caretakers and Health Centre clinicians on duty. Finger prick blood specimens were collected from each participating child. The collected specimens were used for preparation of blood smears and Paracheck Pf® dipstick test (Orchid Biomedical Services, India). Thick and thin smears were prepared on the same slide and stained with 10% Giemsa solution for 30 minutes after fixing the thin smear with methanol. The blood smears were carefully examined by skilled microscopists using an oil immersion lens. Smears were deemed negative if there was no evidence of any parasites observed after reading 200 high power fields. In the event of the presence of parasites, the thick smear was used to determine the number of parasites present, while the thin smear was used to determine malaria species composition. Parasitaemia was specifically measured for asexual forms per 200 white blood cells (WBC) and gametocytes were counted per 500 WBC. For detecting malaria parasites using Paracheck Pf®, fresh blood sample was transferred directly to the sample pad and results were read after 15 minutes as recommended by the manufacturers. Presence of both the control and test lines indicated a positive result. A negative result was indicated by the appearance of the control line alone. The result was considered invalid where both the control and test lines did not appear in which case the test was repeated. Axillary temperature was measured with a digital thermometer. Using the same prick, a sample of blood was collected for haemoglobin (Hb) concentration determination using Haemocue machine. Anaemia was considered when Hb level was < 11g/dl. Statistical analysis Data were entered in Epi Info (Centers for Disease Control & Prevention, Atlanta, GA, USA) and thereafter transferred, and analysed using STATA Version 8 for Windows. In order to investigate whether there was relationship between malaria status and other risk factors, Shapiro-Wilk test was used to test normality of continuous variables (age, haemoglobin level and measured body temperature). Chi-square test was done to determine whether there was an association between malaria status and other categorical variables, while ANOVA was used to determine the mean levels of each continuous variable in respect to other categorical variables under study interest. The effect modifier of the potential confounder value (age) with other risk factors, was also assessed. Akaike Information Criteria (AIC) method of comparing deviance of the two models that were nested was used, and the model with the least AIC value was selected as the best model. Hosmer-Lemeshow goodness-of-fit test was carried to assess the adequacy of logistic regression model obtained. The significance of the test was considered if p-value was ≤ 0.05. The sensitivity, specificity, predictive positive and negative values of Paracheck Pf ® were calculated using microscopy as the gold standard. Sensitivity was measured based on the number of true positive malaria cases identified correctly by Paracheck Pf® divided by the total number of those diagnosed as positive malaria cases by microscopy plus false negative results. Specificity was measured based on the number of true negative malaria cases identified correctly by Paracheck Pf® divided by the total number of those diagnosed as negative malaria cases by microscopy plus false positive results. Positive Predictive Value (PPV) was measured based on the number of true positive malaria cases identified correctly by Paracheck Pf® divided by the total number of true positive cases and false positive cases obtained from the infected and non-infected cases. Negative Predictive Value (NPV) was measured based on the number of true negative malaria cases identified correctly by Paracheck Pf® divided by the total number of true negative cases and false negative cases obtained from the infected and the non-infected cases. Results A total of 301 children were involved in the study and were divided into three age groups: <1year, 1-4 years, and ≥5 years. Most of the children (51.1%) were in the age group of 1-5 years and majority (54%) were males (Table 1). The mean and median age of the children was 2.54 and 1.7 years, respectively. Twenty-nine percent of the children were febrile (with temperature above 37.50C). Eighty nine percent of parents/guardians reported using bednets out of whom 52.2% were using insecticide-impregnated nets. Of the examined children, 29 (9.6%) were positive for malaria by microscopy while 30 (10%) were positive by Paracheck Pf®. Plasmodium falciparum was the only malarial species observed among the 29 microscopy positive cases. Children aged 1-5 years comprised 58.6% of those diagnosed with malaria. Geometric mean parasite density of P. falciparum asexual forms (calculated by multiplying parasite count/200WBC) was highest in infants and lowest in children ≥5 years age group (Table 1). Geometric mean parasite density was not significantly different between age groups (F = 1.49, P= 0.24) and sex of the patients (F = 1.46, P= 0.23). Seven children (2.3%) had gametocytes (detected by microscopy). Two patients with gametocytes were microscopically negative but positive to Paracheck Pf® while other two patients had gametocytes but were negative for both microscopy and Paracheck Pf®. The overall mean haemoglobin level was 10.92g/ dl (95%CI 10.70 -11.14) and ranged from 4.7016.00g/dl. The prevalence of anaemia was 53.16% and children less than 5 years of age accounted for 60.32% of all anaemia cases. Over 72% of the children diagnosed with malaria were also anaemic and anaemia was significantly associated with malaria (P =0.029, χ2=4.8). When the effect of malaria status was controlled, a five-fold increase in age was associated with decrease in anaemia by 93.85% (95% CI: 60.68 - 99.06, P= 0.004). The risk of anaemia among children under five years decreased by 36% with an increase in age. Six variables were observed to fit well in predicting malaria status for the study children. These included age of the children, febrile status, being anaemic, and having symptoms of vomiting, abdominal pain and diarrhoea (Table 2). The risk of being a positive case was observed to be 4.17 times more likely among febrile patients, and was also 4.48 times among anaemic patients (adjusted by other factors) (Table 2). This model indicated a predictive probability ability of model with these six variable to be 0.77 (95% CI: 0.66 – 0.88). Among the 30 positive cases detected by Paracheck Pf®, three were found to be negative by microscopy; yielding three false positive results (sensitivity = 93.1%). Also, among the 271 negative cases observed by ParacheckPf®, two cases were detected as positive by microscopy; yielding two false negative results (specificity = 98.2%) (Table 3). Discussion In general, the results from this study show that the performance of Paracheck® was comparable to microscopy. The prevalence of malaria by both microscopy and Paracheck® was similar. Only a small proportion of the children had measured fever (Temperature ≥37.5ºC), indicating that most likely the children had received antimalarials/antipyretics prior to attending the health facility. Using microscopy as the standard, Paracheck® had a sensitivity of 93.1% and specificity of 98.9% with positive and negative predictive values of 93.3% and 99.2%, respectively which are similar to recent findings from other areas of Tanzania (Mboera et al., 2006a). Taking into account the fact that all the cases enrolled in our study were clinically diagnosed as malaria cases with intention to treat, it means that 90% of the patients would have received courses of antimalarials despite having no malaria parasites in their blood. Such overdiagnosis has been reported in northern Tanzania by Reyburn et al. (2004) who found that only about half of the patients treated for malaria had negative results by microscopy. The results of this study have shown that Para-check Pf® is both a sensitive and specific test for P. falciparum. However, the test failed to detect three cases, which were positive and two cases, which were negative by microscopy, respectively. Too low levels of parasitaemia are likely to be reasons for the false negative results (Mboera et al., 2006a). The false positive cases are likely to have been of patients who took antimalarials a few days prior to seeking care from the health facility. Anaemia was prevalent among children attending the healthcare facility. Similar findings have been reported elsewhere in the country. For instance, recently, in a community-based study in southern Tanzania, Schellenberg et al. (2003) reported higher prevalence of anaemia (87%) among children under five years of age. In our study, the risk of anaemia was observed to be about 5 times more likely in children with positive blood slides for malaria parasites than those without malaria parasites. Studies have already shown that malaria is an important cause of anaemia in endemic countries (Robert et al., 2003). Therefore it is likely that most of the anaemia cases observed in our study were malaria related. In conclusion, Paracheck Pf® is comparable to microscopy is detecting malaria in clinical cases. Malaria prevalence among children in Tanga City is low. Similarly, recent studies in Dar es Salaam (Wang et al. 2006) Dodoma and Iringa in Tanzania (Mboera et al., 2006b) have shown low malaria prevalence among children living in urban areas.The low malaria prevalence observed in this study could be attributed to high mosquito net coverage as shown by the response of the caretakers. It could also be due to availability of few breeding sites for malaria mosquitoes. However, basic healthcare delivery systems providing early diagnosis and treatment and preventive actions such as the promotion of insecticide-treated mosquito nets for the rapidly growing numbers of the urban population needs to be promoted. Acknowledgements We are grateful to the children and their parents/ caretakers for participating in the study. We also thank the Tanga City authority for the permission to conduct the study. All staff of the Makorora Health Centre are thanked for their support. This study received financial support from the National Institute for Medical Research, Tanzania References
© Copyright 2008 - Health User's Trust Fund (HRUTF) The following images related to this document are available:Photo images[th08004t1.jpg] [th08004t3.jpg] [th08004t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}