 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
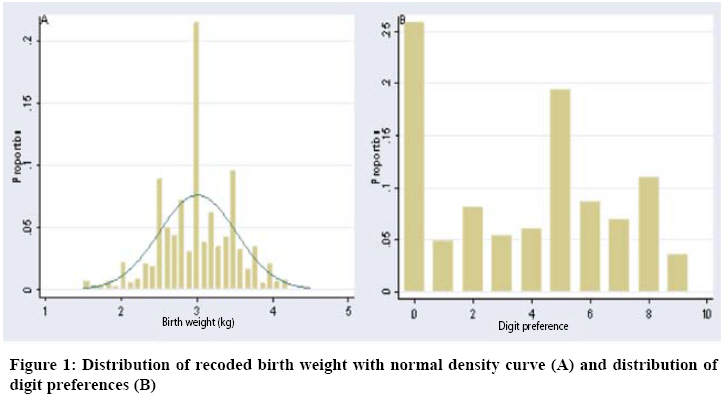
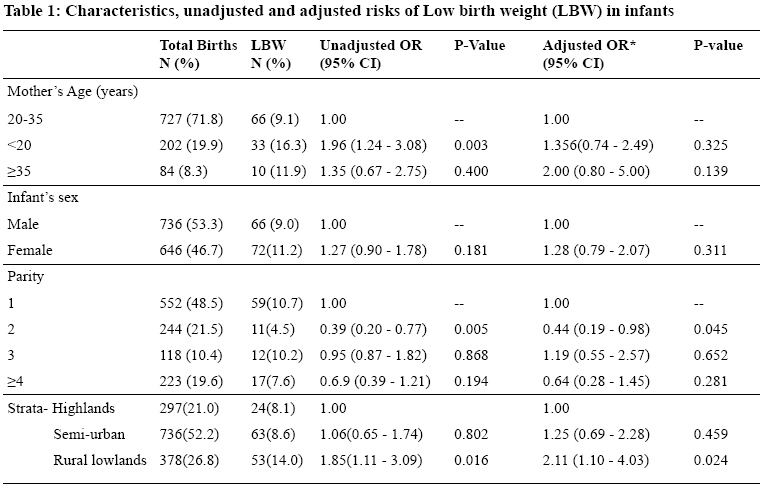
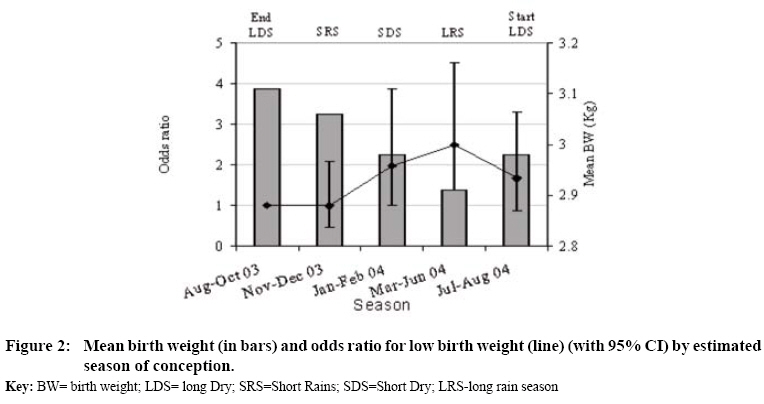
Tanzania Journal of Health Research, Vol. 10, No. 3, July, 2008, pp. 137-143 Risk factors for low birth-weight in areas with varying malaria transmission in Korogwe, Tanzania: implications for malaria control B.P. Mmbando1*, H. Cole-Lewis2, S. Sembuche1, M.L. Kamugisha1, T. Theander3, J.P.A. Lusingu1 and M.M. Lemnge1 1National Institute for Medical Research, Tanga Medical Research Centre, Tanzania Received 14 February 2008 Revised 17 June 2008 Accepted 18 June Code Number: th08024 Abstract Low birth weight (LBW) is a risk factor for infant mortality, morbidity, growth retardation, poor cognitive development, and chronic diseases. Maternal exposure to diseases such as malaria, HIV, and syphilis has been shown to have a significant impact on birth weight (BW). This study was aimed at determining whether there was a difference in rates of LBW in areas of varying malaria transmission intensity in Korogwe, Tanzania. Retrospective data for one year (June 2004-May 2005) in three maternal and child health (MCH) clinics in the district were analysed. Villages were stratified into three strata: lowlands-semi urban (average altitude of 320m), lowlands-rural (below 600m) and highlands (≥600m). There was a significant decreasing trend of rate of LBW from rural lowlands to highlands (χ2 trend =7.335, P=0.007). Adjusting for covariates, women in parity-two were at reduced risk of delivering LBW babies compared to first parity women (OR=0.44, 95% CI 0.19-0.98, P=0.045). Similarly, the risk of LBW was higher in women who had delayed MCH gestational booking and in women who conceived during high malaria transmission seasons. There was high degree of preference of digits ending with 0/5 in reporting BW in the studied MCHs. In conclusion, a rate of LWB was high in rural lowlands where malaria is also endemic, and was associated with high malaria transmission seasons. Keywords: Low birth weight, malaria, transmission intensity, Tanzania Introduction Low birth weight (LBW) is a risk factor for infant mortality, morbidity, growth retardation, poor cognitive development (Wang et al., 2008), and chronic diseases (Hughson et al., 2003). It is defined as birth weight <2500g irrespective of gestational age. LBW is mostly common in developing countries, where the burden of malnutrition and infectious diseases is heavy, and the incidence is estimated to be more than twice that of developed countries (Dreyfuss et al. 2001). In sub-SaharanAfrica, estimated rate of LBW is 14 per 100 live birth based on statistics derived from health facilities, which constitute about 35% of all live births occurring in the region. Similarly, based on health facility statistics of 1999, which included only 45% of infants weighed at birth, incidence rate of LBW in Tanzania was 13 per 100 live births (UNICEF 2004). LBW is a result of limited intrauterine growth as well as preterm birth (Shulman et al. 2001). It can be the result of many factors related to the infant, mother, and environment. These factors include multiple delivery, nutrition, age, lifestyle, body type, and socioeconomic class of the mother. Exposure to diseases such as malaria, HIV, and syphilis also affect birth outcomes (Watson-Jones et al., 2007; Iroha et al., 2007) Malaria especially due to Plasmodium falciparum which affects about two-third of the world is associated with high rates of LBW and causes harmful complications in pregnancy including anaemia, pre-term delivery, foetal and peri-natal mortality and maternal mortality (Wort et al., 2004). In malaria endemic areas, 19% and 6% of cases and deaths of LBW respectively are attributable to malaria (Guyatt & Snow, 2004). P. falciparum poses the greatest risk to children and pregnant women. Population residing in highland areas experience lower rates of malaria transmission than in the lowlands, mainly because low temperatures in the highlands do not favour mosquito breeding and prolong the development of parasites in mosquitoes (Drakeley et al., 2005; Martens, 1995). Pregnant women, especially from malaria endemic areas, do not necessarily develop symptoms when they become infected, however the persistent infection increases the risk of placental parasitaemia and maternal anaemia which are among the leading causes of low birth weight and poor survival for infants in Africa (Guyatt & Snow, 2004). Studies have shown that as gravidity increases, the incidence of LBW due to malaria infection decreases, hence primigravidae births have the highest rate of LBW (Mutabingwa et al., 2005). In a study done in Tanzania, the risk of delivering a baby with LBW was found to increase five months after a malaria epidemic, implying that the foetus is at high risk during the first few months of pregnancy (Wort et al., 2004). However, the period for which the foetus is at high risk and that malaria interventions should be instituted is not clear. The objective this study was to determine the seasonal variation in prevalence of LBW between areas of varying malaria transmission in Korogwe, north-eastern Tanzania, using altitude and urban as a proxy measure of transmission. Secondary objectives were to determine the effect of Maternal and Child Health (MCH) clinic booking gestational age on birth weight. Material and Methods Study area and population Korogwe district (5°9 S, 38°29 E) is located in northeastern Tanzania and spans 3756 km2. It has a population of 260,238 and a growth rate of 1.2% per year (URT, 2003). It is divided into 4 divisions, 20 wards and 133 villages lying at 250 to 1200 m. There are two rainy seasons; short rains between November and December and long rains between March and June. The district is served by two hospitals, four health centres and 47 dispensaries, and all provide maternal and child health (MCH) services. This study was done in three MCH clinics, namely Korogwe District Hospital (300m), Lewa Dispensary (~600m) and Bungu Health Centre (1200 m). The major ethnic groups in the district are Sambaa and Zigua. The main economic activity of the district is agriculture where maize, beans, and cassava are the subsistence and cash crops. Small-scale animal husbandry is practiced by a few inhabitants. Study design and data collection This was a health facility based retrospective review of data of pregnant mothers who delivered in the three health facilities in Korogwe district. Records of women who delivered a singleton in the three MCH clinics from June 2004 to May 2005 were extracted from the registers. Maternal information collected included age, village of residence, parity (number of births), gestational age at first booking, place of booking and number of days the mother was hospitalised. Infant information collected included birth weight, sex and vital status of the baby at delivery. In all MCH clinics birth weight was measured by using analogue scales. For the purpose of relating birth weight with the spatial data, the study area was stratified into three strata. Villages with altitude below 600m and located in the rural areas were categorised as rural-lowland stratum, villages located above 600m were referred as highland stratum, and those within Korogwe township were referred as semi-urban lowland (URT, 2003). Data analysis Data were double entered and validated using Microsoft Access software. Statistical analysis was done using STATA version 8.0. Gestation period of 40 weeks was considered as full term. LBW was defined as any weight at birth below 2.5kg irrespective of gestation age according to WHO (UNICEF 2004). Booking gestation age was stratified into two categories, early booking (<25 weeks) and late booking (≥25 weeks). In the analysis, seasons of a year were grouped into four categories: (i) July-October as the long dry season, (ii) November-December as the short rainy season, (iii) January-February as the short dry season and; (iv) March-June as the long rainy season. Categorical data was compared using χ2-test, continuous variables were compared using t-test and analysis of variance tests. Regression methods (logistic and linear) were used to determine covariates with elevated risks. A P-value less than 0.05 were considered significant. Results During the period under review, June 2004 to May 2005, data on a total number of 1458 women who delivered infants with birth weight recorded was extracted from the registers and analysed. The birth ratio for female to male was 1:1.1. Most mothers were recorded in Korogwe 1225 (84.4%), and the remaining were from Bungu 144 (9.9%) and Lewa 82 (5.7%). Over 70% of the mothers were 20-35 years old, with mean age of 24.7 years. Women residing in semi-urban areas made up 52.2% while those in the rural lowlands represented 26.8% of the studied population. About 46% of the women were first-time mothers. Birth weights were normally distributed, however there was a high rate of digit preference in reporting the birth weights, especially to the nearest terminal digit 0 and 5 (Figure 1 A and B). The overall rate of low birth weight was 9.9% (95% CI: 8.4-11.5) while mean birth weight was 3.01 kg (95%CI: 2.98-3.04). Univariate analysis showed that the frequency of LBW was significantly higher in lowlands rural (14.0%) compared to semi-urban (8.6%) and highlands (8.1%), χ2 trend =7.335, P=0.007. There was no significant difference in rate of LBW between the lowlands rural and semi-urban (Table 1). Similarly, mean BW was significantly different in the three strata; highlands (3.11kg; 95%CI 3.05-3.17), semi-urban (3.0 kg; 95%CI 2.97-3.04), while in the lowlands was (2.94 kg; 95%CI 2.89-3.00), P<0.001. The risk of delivering a baby with LBW was two folds higher for women aged below 20 years of age compared to women in age group 20-34 years; while the difference was not significant for women aged 35 and above. Moreover, the odds of delivering a baby with LBW decreased with increased parity, whereas the risk in primiparity was two fold as high as in second parity. From the linear regression analysis where highlands was reference group, mean birth weight decreased with strata, whereby in semi-urban the decrease was by 0.16kg (95%CI 0.08 - 0.24, P<0.001) while in lowlands rural decrease was 0.25kg (95%CI 0.14-0.36, P<0.001). Increase in parity was associated with increase in birth weight by 0.05kg (95% CI 0.02-0.09, P=0.003), while boys were 0.08kg (95%CI 0.01-0.15, P<0.029) heavier than girls. There was no significant difference in the mean birth weight between mothers’ in the three age groups. Women who booked early had babies with a significantly higher mean birth weight (2.99kg) than those who booked late (2.89kg), P=0.040. Adjusting for effect of strata, sex, parity and age, women with delayed booking the rate of LBW was higher (OR=1.78, 95%CI 0.91-3.47, P=0.092). Risk of delivering a LBW baby was significantly higher during short dry season (OR=1.97, P=0.044) and long rainy season (OR=2.485, P=0.002) compared to end of long dry season (Figure 2). Odds ratios of LBW in short rains and beginning of the long dry season were not significantly different from that at the end of the long dry season (P=0.966 and P=0.133), respectively. There was a significant difference in mean BW between the seasons (F=6.41, P<0.001). Furthermore, in months where the mean birth weight was highest, the odds ratio was lowest and vice versa (Figure 2). Women who booked early had babies with a significantly higher mean birth weight (2.99kg) than those who booked late (2.89kg), P=0.040. Adjusting for effect of strata, sex, parity and age, women with delayed booking the rate of LBW was higher (OR=1.78, 95%CI 0.91- 3.47, P=0.092). Risk of delivering a LBW baby was significantly higher during short dry season (OR=1.97, P=0.044) and long rainy season (OR=2.485, P=0.002) compared to Risk of delivering a LBW baby was significantly where the mean birth weight was highest, the odds ratio higher during short dry season (OR=1.97, P=0.044) and was lowest and vice versa (Figure 2). long rainy season (OR=2.485, P=0.002) compared to end of long dry season (Figure 2). Odds ratios of LBW in short rains and beginning of the long dry season were not significantly different from that at the end of the long dry season (P=0.966 and P=0.133), respectively. There was a significant difference in mean BW between the seasons (F=6.41, P<0.001). Furthermore, in months where the mean birth weight was highest, the odds ratio was lowest and vice versa (Figure 2). Discussion In this study the relationship between LBW and areas with varying malaria transmission, where altitude and urban were used as a proxy of transmission was investigated in children born to women living in Korogwe, Tanzania. The results of this study indicate that there is a higher rate of LBW in the lowlands rural than in semiurban and highlands. Malaria epidemiology studies have shown low rates of malaria transmission in the urban and semi-urban lowlands areas (Modiano et al. 1999; Wang et al. 2006) and urban highland areas (Mboera et al., 2006); therefore, the observed different in rates of LBW and mean birth weight in the three strata could be attributed to malaria infections (Wort et al., 2006a; Steketee et al., 2001; Dreyfuss et al., 2001;Ticconi et al., 2005). There was high rate of digit preference in recording birth weights in these health facilities, a phenomenon which has been reported in other areas (Sone et al., 1993; Edouard & Senthilselvan 1997) and this introduces recording bias which eventually bias rate of LBW. Regular training of MCH staff could minimise recording bias, however its feasibility and variation between staff and between facilities possess another challenge. So, introducing digital weighing scales remains the feasible and sustainable solution in minimising such errors (Sone et al. 1993). Although regression analysis showed non-significant results of effect of maternal age on birth weight which could be due to low statistical power, the trends observed still indicate that women with lowest risk of LBW are those between the ages of 20-35 years. The trend falls in line with previously reported studies, which found that adolescent mothers had infants with lower mean birth weight and increased risk for LBW than those born to older mothers (Borja & Adair, 2003; Wort et al., 2006b). Like previously published studies, this study records a noticeable decrease in the risk of LBW as well as the rate of LBW in multiparity when compared to primiparity (Wort et al., 2004; Rosenberg 2004). In this study, women who booked before the gestational age of 25 weeks reported higher mean birth weight and lower odds for LBW. However, this was not statistically significant because of low power due small sample in women with delayed booking. Nonetheless, the findings of this study are consistent with studies that found antenatal care can lower chances of suffering from pregnancy complications such as anaemia and pregnancy-induced hypertension (Mohamed et al., 2006). It is obvious that women who had late or no antenatal care were less likely to have received interventions such as IPTp and ITNs, since these are given during the second trimesters (Wort et al. 2006b). The odds ratio of LBW showed an increase in the short rainy season (November to December) and peaked during the long rainy season (March to June). The long rainy season was also the period with the lowest recorded mean birth weight. A decrease in LBW odds was observed from the long rainy season to the end of the long dry season (August to October). The mean birth weight at the end of the long dry season was also the highest recorded. The pattern showed that birth weight was lowest in the long rainy season and increased gradually throughout the year and peaked at the end of the dry season. This corresponds to malaria transmission pattern in the area which fluctuates with season (Lusingu et al., 2004). This is also likely to be true to the observation that women who conceived during months of low malaria transmission were at lower risk of delivering infants with LBW. In Tanzania, prevention of malaria in pregnancy by IPTp using sulfadoxine-pyrimethamine (SP) is done during the second and third trimester (Wort et al., 2006b) while use of ITNs through subsidised voucher scheme is instituted following the first booking (Kweku et al., 2007) which in most cases happens after the first trimester. The findings indicate the need for more studies on IPTp strategy and exploration of the best time of providing ITNs to pregnant mothers. The study was limited in terms of observation time and sample size covered, which resulted in less statistical power in some of parameters. Moreover, in tropics there are many factors which can contribute to seasonal variation in LBW, such as inadequate food and human activities such as farming which could not accounted for in the model. Acknowledgements We would like to acknowledge Eva Nyenza and Beatrice Semng’indo for data collection, Neema Barua, Annette Goso, Silas Msangi and Benson Swai for data entry. Allen Mrango is acknowledged for driving the team. Godfrey Mubyazi is thanked for critical comments on the earlier version of the manuscript. Korogwe District Hospital authority is acknowledged for permission to use the MCH data. This work was financially supported by the National Institute for Medical Research-Morehouse College students exchange programme and Danish International Development Agency. References
© Copyright 2008 - Health User's Trust Fund (HRUTF) The following images related to this document are available:Photo images[th08024f2.jpg] [th08024f1.jpg] [th08024t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}