 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
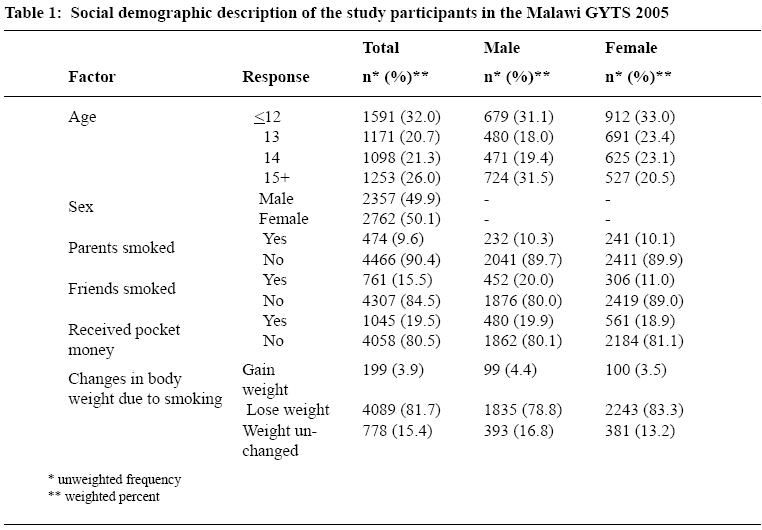
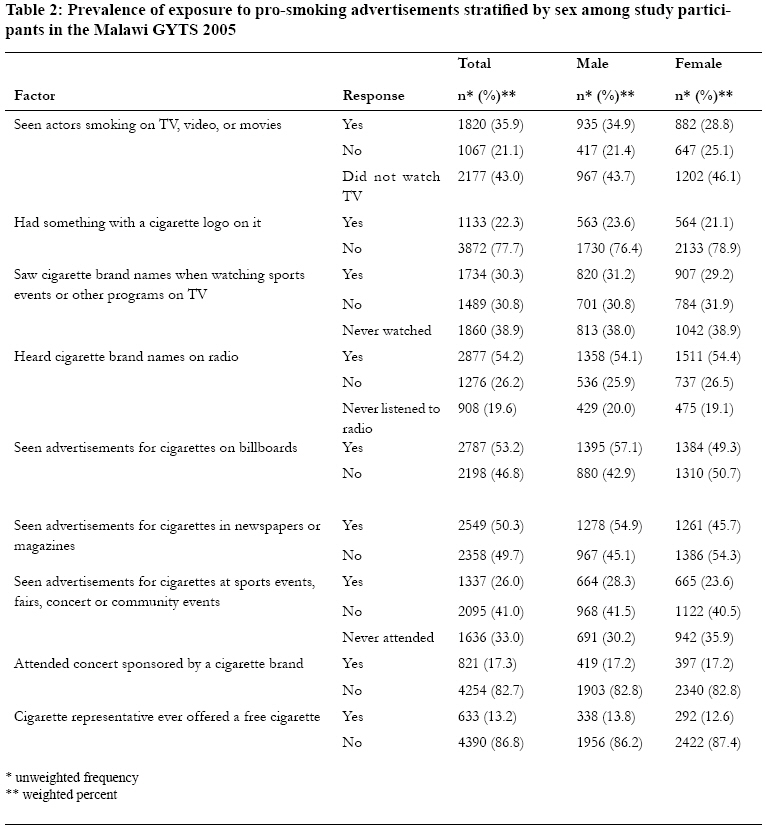
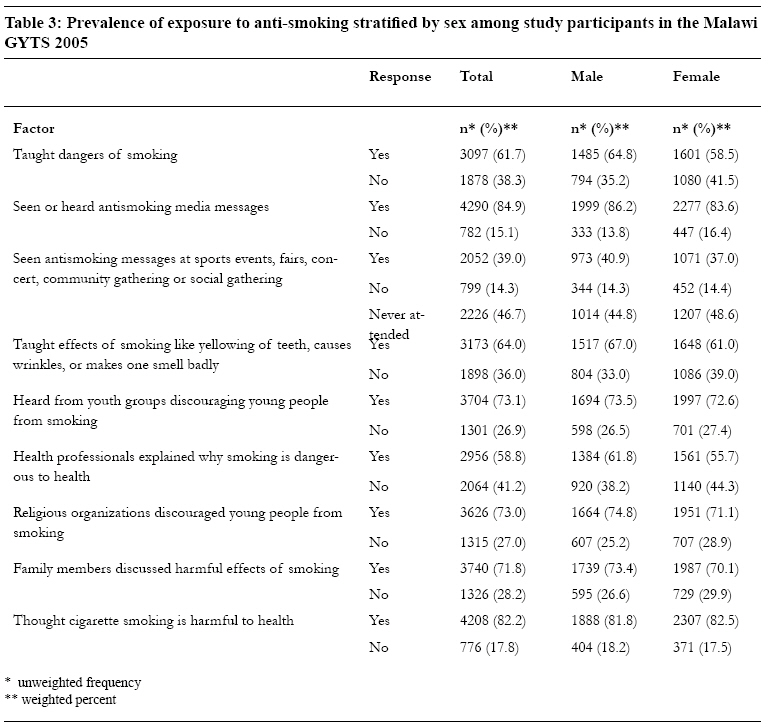
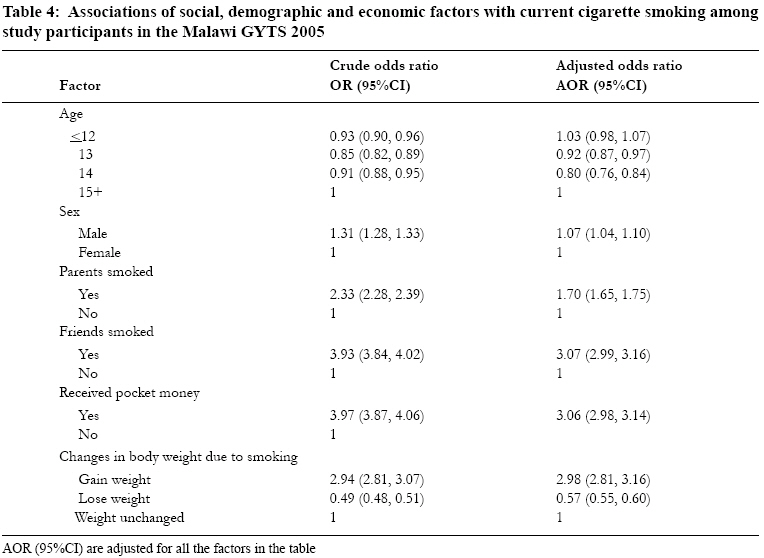
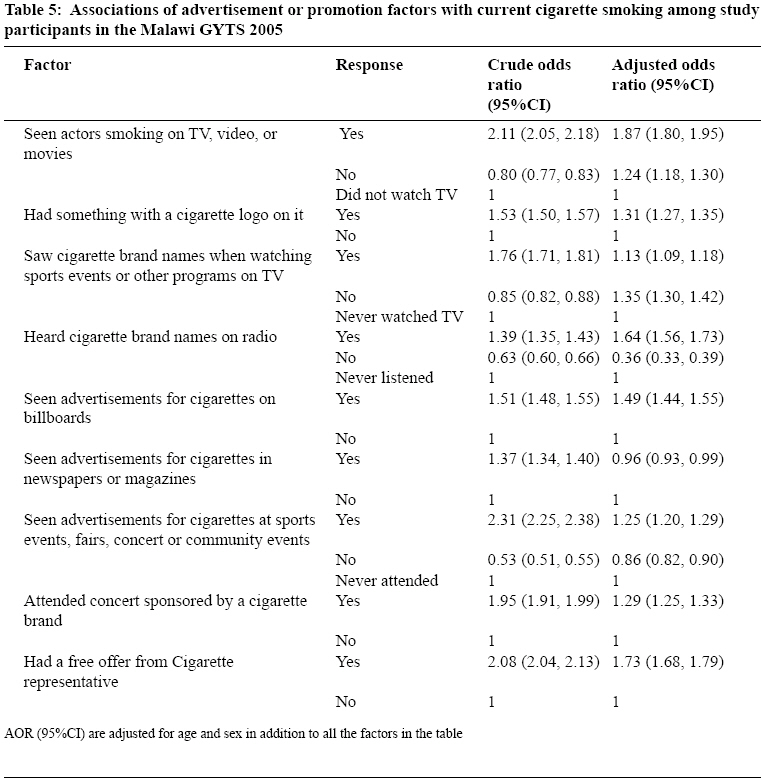
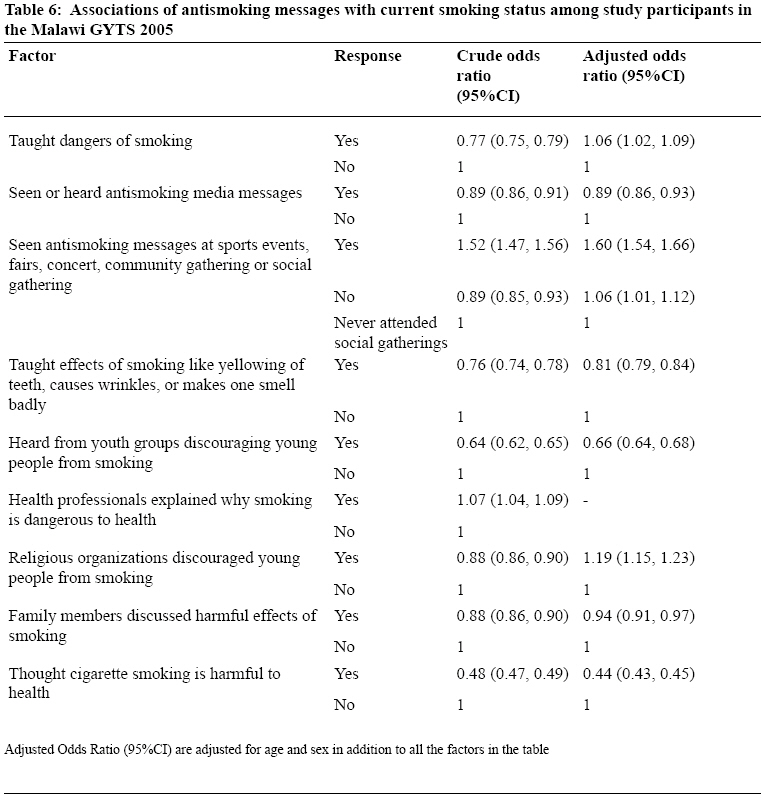
Tanzania Journal of Health Research, Vol. 10, No. 3, July, 2008, pp. 166-176 Prevalence and correlates of cigarette smoking among adolescents in Malawi: results from the Global Youth Tobacco Survey 2005 A.S. Muula1,4, S. Siziya2* and E. Rudatsikira3 1Department of Community Health, University of Malawi, College of Medicine, Blantyre, Malawi Received 11 May 2008 Revised 12 June 2008 Accepted 13 June 2008 Code Number: th08028 Abstract The majority of adults who smoke cigarettes initiated the habit when they were adolescents or young adults. While rates of smoking and associated factors are known among 13-15 year olds in Malawi, correlates of cigarette smoking among adolescents in a national representative sample in Malawi have not been studied. We, therefore, carried out this study to estimate the prevalence of current smoking and determine its correlates in a nationally representative sample of in-school adolescents in Malawi. An analysis of the Malawi Global Youth Tobacco Survey (GYTS) 2005 was conducted. Using logistic regression analysis, we estimated the association between current cigarette smoking and potential explanatory variables. Overall, 2.5% of adolescents (3.2% among males, and 1.8% among females) were current cigarette smokers. Smoking among parents was 9.6% with no significant difference between males and females (10.3% versus 10.1%). Stronger associations with smoking were observed for friends smoking status (AOR=3.07, 95%CI 2.99, 3.16), receiving pocket money (AOR=3.06, 95%CI 2.98, 3.14), and perception that smoking increases body weight (AOR=2.98, 95%CI 2.81, 3.16). Students who thought that cigarette smoking is harmful to health were 56% (AOR=0.44, 95%CI 0.43, 0.45) less likely to smoke than students who thought otherwise. Despite being the world’s second leading grower of tobacco, the prevalence of cigarette smoking among adolescent is lower than has been reported elsewhere. Key words: in-school adolescent, cigarette smoking, Malawi Introduction Tobacco is a leading cause of preventable non-communicable deaths. Mathers and Loncar (2006) projected the total tobacco-attributable deaths to rise from 5.4 million in 2005 to 6.4 million in 2015. Furthermore, tobacco was projected to kill 50% more people in 2015 than HIV/AIDS, and to be responsible for 10% of all deaths globally. Recently, Pampel (2005) using data from the Malawi Demographic and Health Survey of 2000, reported the prevalence of cigarette smoking at 16–18% for men and 1% for women. Muula and Mpabulungi (2007) and Muula (2007) have reported the prevalence of current cigarette smoking among in-school adolescents at 6.2% in Lilongwe and 3.0% in Blantyre in Malawi using data obtained from the Global Youth Tobacco Survey (GYTS) of 2001. Before the 2005 Malawi GYTS, there was paucity of data on a national representative sample of adolescents in Malawi. Following the 2005 survey, a fact sheet (CDC, 2005) has been published outlining rates of a limited list of tobacco use and associated factors. However, the possible associations of any explanatory variables to cigarette smoking have not been reported at a national level. The majority of adult smokers initiated the habit as adolescents or young adults. This therefore makes the monitoring and prevention of adolescent smokers a critical public health exercise. Our understanding of adolescent smoking is enriched when we also explore the socio-demographic variables that are associated with smoking at both the personal and the societal level. We therefore carried out this study to estimate the prevalence of current smoking and associated variables in a nationally representative sample of in-school adolescents in Malawi. We also assessed associations between relevant explanatory variables and current cigarette smoking among the adolescents. Materials and Methods This study was based on a secondary analysis of data from the 2005 Malawi Global Youth Tobacco Survey. A comprehensive description of the GYTS purpose and methodology has been reported elsewhere (Warren et al., 2008). In brief however, the GYTS uses a questionnaire survey, recruits in-school adolescents from classes and the majority of students are aged between 13-15 years. A two-stage clustered sampling approach is used in which the primary sampling units are schools. In the second stage of sampling, classes within the school are randomly selected. All students within the selected classes are eligible to participate in the study, regardless of their actual ages. However, students are free not to participate although identified as eligible for participation. Study participants self-complete a questionnaire that has standard “core” questions, and a few other country-specific questions that are included by the specific country team. The core questions enable meaningful comparisons on responses between countries. Completion of the questionnaire is estimated to take about 40 minutes, and is done within a class session. There is no recording of student names or any person identifiers on the questionnaire. Questions are asked to collect information on the following variables: age, history of having ever smoked, sex, current smoking status, parental smoking, having friends who smoked, exposure to environmental tobacco smoke and tobacco advertisements, perception that smoking is harmful to health and amount of pocket money usually received per month. In the Malawi GYTS, permission to conduct the study was obtained from the Ministry of Education. Completed questionnaires were scanned by computer and a data file was generated in Access. Overall response rate was 92.5%. As per GYTS methodology, current cigarette smoking was defined as having smoked even a single puff of cigarette within the last 30 days preceding the survey (Warren et al., 2000). Data were analyzed using SPSS software version 14.0 (Chicago, Illinois, United States). To assess associations between variables that were identified from the literature as possibly associated with current cigarette smoking, logistic regression analysis was conducted both at bivariate and multivariate level (Rudatsikira et al., 2008; Siziya et al., 2007). Backward logistic regression analysis was conducted to identify variables that are independently associated with smoking. Associations of cigarette advertisement or promotion factors with the outcome were adjusted for age and sex in addition to the other factors in the model. Messages against cigarette smoking were also adjusted for age and sex in addition to factors in the model. We report crude odds ratios (OR) and adjusted odds ratios (AOR) together with their 95% confidence intervals (CI). Results Sample description A total of 5135 students participated in the Malawi GYTS 2005. However, data on sex were available for 5119 students of whom 46.0% were male, and 54.0% were female students. About a third (32.0%) of the students was aged 13 years. The proportions of participants whose parents and friends smoked were 10.3% and 15.5%, respectively. The overall prevalence of current smoking was 2.5% (1.8% among females, and 3.2% among males). The majority (86.0%) of the students felt that smoking makes one lose weight. One in five (19.5%) of the students recently received pocket money. Distributions of these factors by sex are shown in Table 1. Overall, a third (31.8% and 30.8%) of the respondents had seen actors smoking on television (TV), video or movies, and saw cigarette brand names when watching sports events or other programmes on TV, respectively. About half (54.2% of the students had heard about cigarette brand names on radio, 53.2% had seen advertisements for cigarette on billboards, and 50.3% had seen advertisements for cigarettes in newspapers or magazines) were subjected to smoking advertisements through the media. About a quarter (26.0%) of the students had seen advertisements for cigarettes at sports events, fairs, concerts, or community events (Table 2). Main sources of antismoking messages were media (84.8%), youth groups (73.1%), religious organizations (73.0%), and family members (71.8%). The majority of the respondents (82.2%) thought cigarette smoking is harmful (Table 3). Between 22.3% and 54.2% of the participants had seen actors smoking on television, had an item with a tobacco brand logo, seen tobacco brands while watching games, heard about tobacco brand names on radio, seen tobacco advertisements in magazine and newspapers, and had seen adverts at sports or community events. About 17.3% and 13.2% had attended a concert promoted by a tobacco company and offered a free cigarette by a tobacco company representative respectively. Social, demographic, and economic correlates for current smoking status are summarised in Table 4. Stronger associations with current smoking status were observed for friends smoking status (AOR=3.07, 95%CI 2.99, 3.16), receiving pocket money (AOR=3.06, 95%CI 2.98, 3.14), and perception that smoking increases body weight (AOR=2.98, 95%CI 2.81, 3.16). All the factors in Table 5 were positively significantly associated with current smoking, except for the factor ‘seeing advertisements in newspapers or magazines’. Students who had seen advertisements for cigarettes in newspapers or magazines were 4% (AOR=0.96, 95%CI 0.93, 0.99) less likely to have been current smokers. Respondents who had seen actors smoking on TV (AOR=1.87, 95%CI 1.80, 1.95), those who had heard of cigarette brand names on radio (AOR=1.64, 95%CI 1.56, 1.73), and those who were offered free cigarettes by a cigarette representative were more likely to smoke cigarettes than those who never watched TV, never listened to radio, and never offered free cigarettes from cigarette representatives. We found that being taught dangers of smoking (AOR=1.06, 95%CI 1.02, 1.09), seeing antismoking messages at sports events, fairs, concerts, community gathering, or social events (AOR=1.60, 95%CI 1.54, 1.66), and religious organizations discouraging young people from smoking (AOR=1.19, 95%CI 1.15, 1.23) were positively associated with current cigarette smoking. The rest of the factors in Table 6 were negatively associated with current cigarette smoking. While explanation by health workers that smoking is dangerous was positively associated with current cigarette smoking in a bivariate analysis, this factor was not significantly associated with current cigarette smoking in a multivariate analysis. The largest magnitude of association was observed for the factor ‘thinking that cigarette smoking is harmful to health’. Students who thought that cigarette smoking is harmful to health were 56% (AOR=0.44, 95%CI 0.43, 0.45) less likely to smoke than those who thought otherwise. Discussion To our knowledge, the Malawi GYTS 2005 is the first ever nationally representative sample of in-school adolescents studied on tobacco use, including cigarette smoking. Previous surveys have been limited to specific geographic areas such Lilongwe and Blantyre (Muula, 2007; Mpabulungi & Muula, 2007). The overall prevalence of current cigarette smoking was 2.5%. The gender difference may be related to societal tolerance of smoking among males compared to females. Compared to the estimate obtained in the GYTS 2001 for Blantyre (3.0%) and Lilongwe (6.2%), the national prevalence is much lower. The reasons behind these differences are not known. However, we can suggest a few possibilities. Both studies in Blantyre and Lilongwe were conducted only in the urban areas of these districts. It is possible that smoking prevalence may be higher in urban commercial centres than the national estimates that also include rural areas. Secondly, it is possible that smoking prevalence has gone down. However, we do not have data for a national estimate for 2001 to verify if this assumption is correct. Nevertheless, between 2001 and 2005, there have been public health efforts, save for legislated changes, aimed to raise awareness among schoolchildren on the harmful effects of smoking. In the developed world, adolescents may be motivated to initiate smoking in order to lose weight, which is perceived as a desirable outcome in these settings. Bean et al. (2008) have reported that adolescent non-smokers believed that smoking would result in weight loss, while smokers believed that they would gain weight if they stopped smoking. However, Bentley et al. (2005) reported that heavier built bodies were desirable among women in Malawi, in contrast to leaner bodies in the United States. Whether adolescents in Malawi hold different or similar views as theirAmerican counterparts deserve further study. The low prevalence of smoking is also reflected in a low smoking prevalence among parents of the study participants. Slama (2008) has reported smoking prevalence rates of 49% and 8% among men and women in low-and mid-income countries. Our estimates are much lower, especially for men (10.3% for Malawi versus 49% globally), but higher for Malawian women (10.1%) compared to the global estimates (8%). It is possible that the Malawi estimates may in fact be underestimates as these (the estimates) were based on reports by smokers’ children. Comparisons with data obtained when adults are surveyed need to be made with this caveat in mind. Factors such as seeing actors smoking on television, having an item with a tobacco brand logo, seeing tobacco brands while watching games, heard about tobacco brand names on radio, seeing tobacco advertisements in magazine and newspapers, and having seen adverts at sports or community events have been reported in previous studies to be associated with smoking among adolescents (Laugesen et al., 2007; Scragg & Laugesen, 2007; Siziya et al., 2007). Exposure to anti-tobacco initiatives such as being taught the dangers of smoking, having seen anti-smoking messages, discussed with family members on smoking and heard anti-smoking messages on the media may have led to the majority (81.8%) believing that smoking is harmful to health. In general, being exposed to pro-tobacco media was associated with increased likelihood of being a smoker. This observation is in keeping with the Social Cognitive Theory (Bandura, 2001; Glanz et al., 2002). The theory proposes that environment, people, and behaviour are constantly influencing each other in influencing behaviour. Of relevance to adolescent smoking is the recognition that the social environment that the adolescent is exposed to may influence when he or she initiates and/or maintains smoking. We note some unexpected findings regarding smoking and explanatory variables. We found that adolescents who reported exposure to anti-tobacco advertisements were more likely to be current cigarette smokers. Study participants who reported being taught the dangers of smoking, had heard religious groups discouraging smoking, seen anti-smoking messages at public events or social gathering, had a health professional discuss smoking with them were more likely to be smokers. We are unable to obtain reasons for these paradoxical associations. However, potential explanations can be suggested. It is possible that adolescents who were smokers were more likely to have a discussion about smoking with a health professional as part of usual clinical care or due to illnesses associated with smoking (e.g. asthma or chronic cough). Schools with high smoking prevalence among students may also be more likely to have lessons aimed at discouraging students from smoking. Another alternative explanation is that the anti-tobacco messages were yet to be effective. Henriksen et al. (2006) have reported that tobacco industry sponsored anti-tobacco messages may not result in decreasing tobacco use. These authors have reported that anti-tobacco messages from tobacco firms were more effective in building corporate image rather than preventing smoking. In Malawi, anti-tobacco message are likely to come from tobacco firms on radio advertisements aimed to promote smoking. Malawi is the second leading grower of tobacco and no other country in the world is economically dependent on tobacco as Malawi (Davies, 2003; Otañez et al., 2007; Diao et al., 2002; FAO, 2003; Jaffe, 2003). However, it appears that such a leading role in tobacco farming has not been translated into the country being a large cigarette consumer. The limitations of the GYTS methodology has been reported elsewhere (Siziya et al., 2008; Warren et al., 2008). Firstly, data was collected from a selfcompleted questionnaire. For the main outcome of the current analysis, students were asked: During the past 30 days (one month), on how many days did you smoke cigarettes? Students may have intentionally miss-reported. It is also possible that some students may have genuinely forgotten whether they had smoked within the past 30 days. Another limitation is the GYTS definition of current smoking, defined as having smoked, even a single puff within the last 30 days. It should be clear that some students who may have smoked a single puff might have never smoked again. As to how many of such students there were in our sample is not known. Nevertheless, if the proportion of students who experimented with a single puff was high, our estimates lead us to exaggerate the public health importance of adolescent smoking in Malawi. The GYTS methodology recruits study participants from schools. Our findings may not be applicable to out-of-school adolescents. Many secondary schoolage adolescents are not enrolled in school. As school attendance is not compulsory and the out-of-school adolescent population is large, the overall prevalence of smoking among adolescents in the country may be assessed if both in-school and out of school adolescents are sampled. Furthermore, the GYTS methodology administers the questionnaire only to those students who are available in school on the day the survey is conducted, and as such, the findings may not be representative of all age-eligible students. However, the response rate was relatively high (84.3%) suggesting that most of the students who were eligible to participate did actually participate in the survey. In addition, the smoking status of the study participants was not validated by biomarkers such as salivary or urine cotinine. Even if these were used, they would have only been useful to determine the smoking status of students within the past few days. A student who had smoked for instance 29 days ago, may not exhibit biomarkers of smoking. Analysis of other bio-samples such as hair or finger nails for tobacco bi-products would also not distinguish between adolescents own smoking and environmental tobacco exposure. In conclusion, we have estimated an over all prevalence of current cigarette smoking of 2.5% among in-school adolescents in Malawi, despite the country being the second leading grower of tobacco. This prevalence estimate is among the lowest in-school adolescents when compared to other estimates reported from similar settings. Acknowledgements We thank all the study participants for their involvement in the study. We are also grateful to the Centres for Disease Control and Prevention (CDC) for making the data from the Malawi GYTS available to us for analysis. The CDC had no influence regarding the analysis that we conducted, nor the decision to have these findings published. References
© Copyright 2008 - Health User's Trust Fund (HRUTF) The following images related to this document are available:Photo images[th08028t5.jpg] [th08028t2.jpg] [th08028t1.jpg] [th08028t6.jpg] [th08028t4.jpg] [th08028t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}