 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
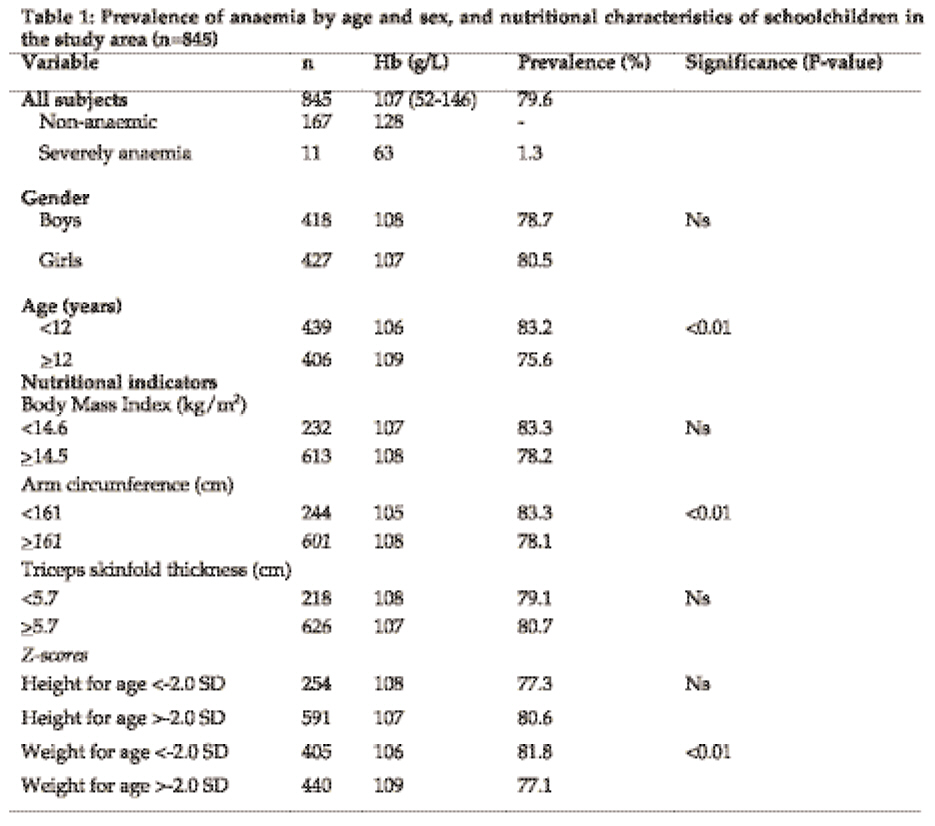
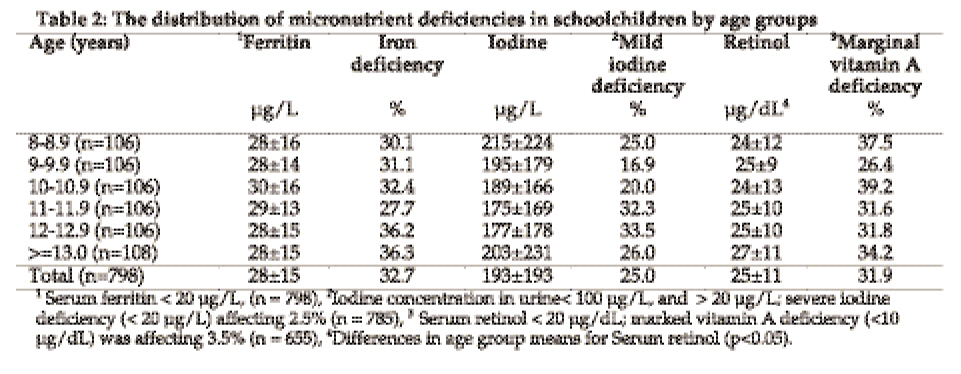
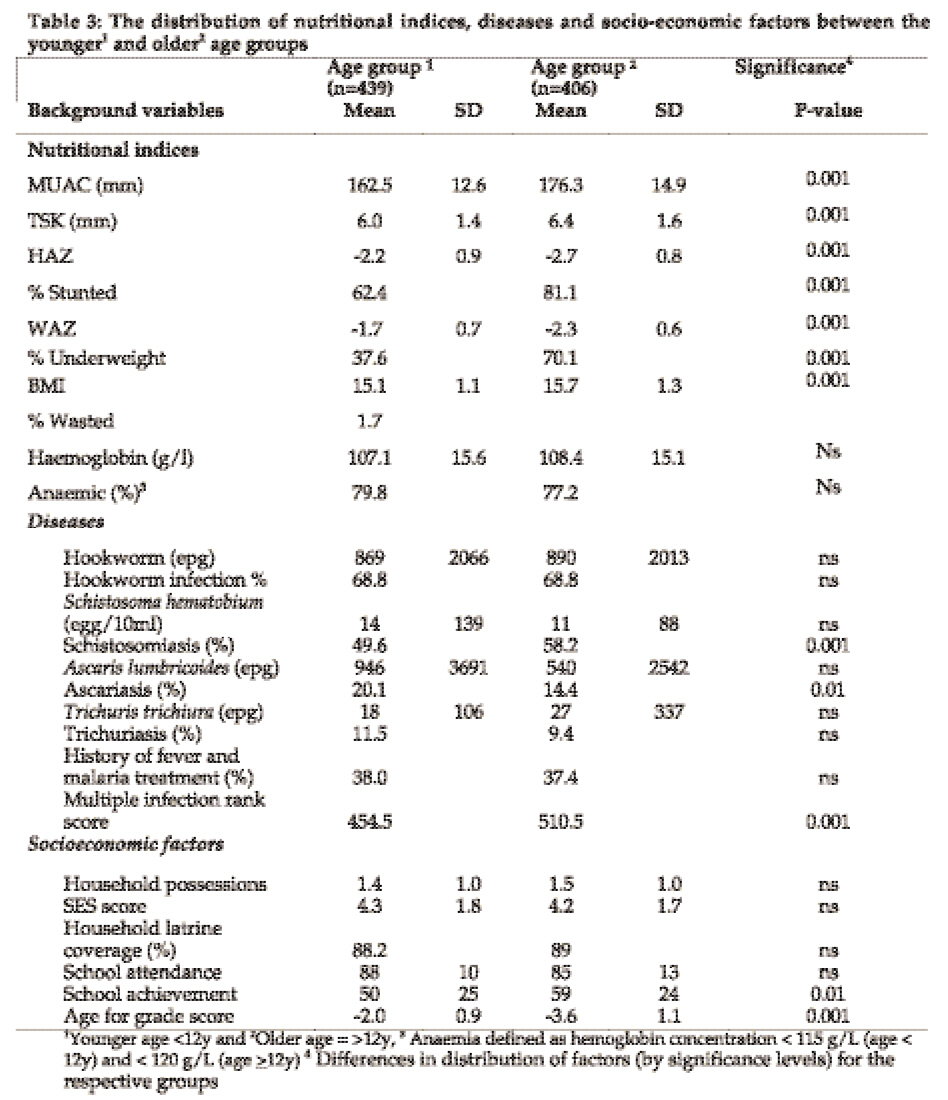
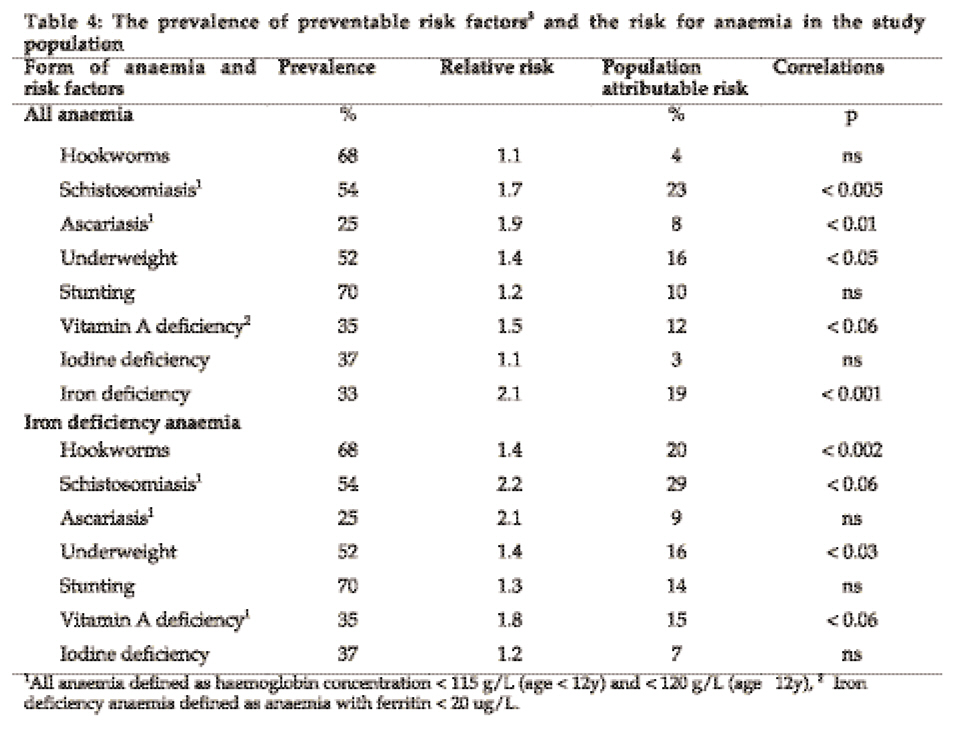
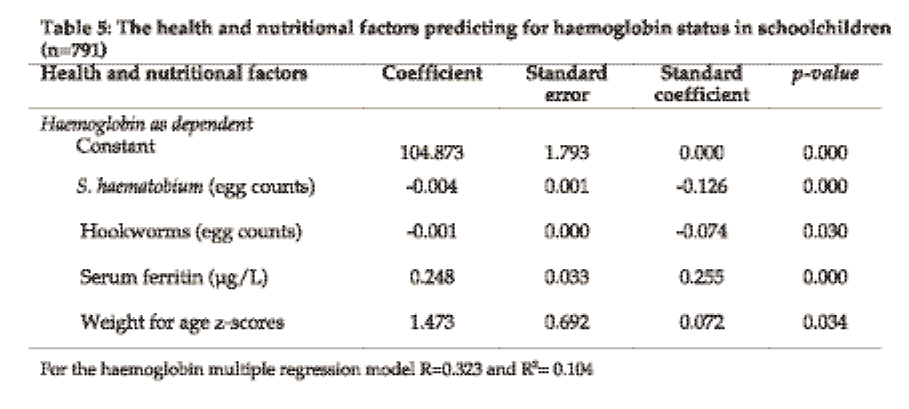
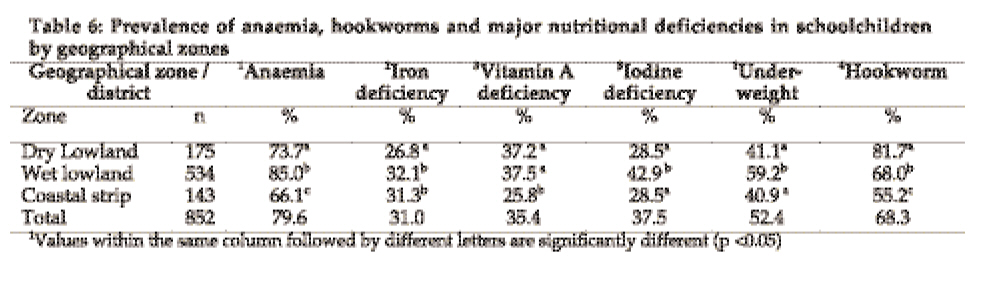
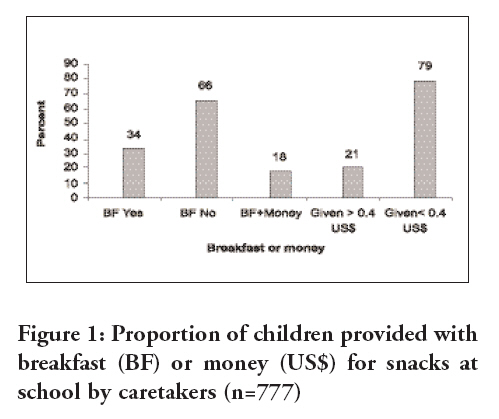
Tanzania Journal of Health Research, Vol. 10, No. 4, Oct, 2008, pp. 189-202 Risk factors for anaemia in schoolchildren in Tanga Region, Tanzania S.R. Tatala1*, C.M. Kihamia2, L.H. Kyungu3 and U. Svanberg4 1Tanzania Food and Nutrition Centre, P.O. Box 977, Dar es salaam, Tanzania Received 23 June 2008 Revised 8 July 2008 Accepted 10 August 2008 Code Number: th08031 Abstract Anaemia is one of the major public health problems affecting more than half of school children along the coast in Tanzania. Due to the multiplicity of its causes it sometimes becomes difficult to find appropriate intervention measures. In order to assist schools in implementing appropriate public health measures for anaemia in Tanga Region of Tanzania risk factors were investigated in school children. A total of 845 schoolchildren age 7-14 years were randomly selected in a cross-sectional survey conducted in 20 randomly selected schools for inclusion in the investigations. Socio-economic, environmental and biological data were collected, as well as academic information, health care and feeding practices. Diagnosis of anaemia was based on haemoglobin concentration below 115g/L determined by HemoCue meter. Serum Retinol was determined by High performance liquid chromatography and serum ferritin by an Enzyme linked immunosorbent assay. Urine from each child was tested for blood using a haematest reagent strip and those testing positive were examined microscopically by filtration method for Schistosoma haematobium ova. A faecal sample collected from them was also examined microscopically for ova and larvae of intestinal worms. To analyse variables associated with anaemia a stepwise multiple regression model was used. The prevalence of anaemia was 79.6%. Micronutrient deficiencies were highly prevalent. Iron deficiency (SF <20 µg/dl) was affecting 33%, vitamin A deficiency (SR < 20 µg/dL) 31.9% and 25% of the children had mild iodine deficiency (UIE < 20 µg/L). Intestinal helminths were also highly prevalent; 68% of children had hookworm and 54% had urinary schistosomiasis. Inadequate diet was a feature in >50% of children. About 10% of households had no latrines and multiple infection rank score was high especially in older age children. The risk of having anaemia was two times higher in children with iron deficiency (RR=2.1) and 49% higher in those with vitamin A deficiency. These deficiencies correlated significantly with the anaemia (P<0.05). Vitamin A deficiency and infections with hookworm and schistosomiasis were the most significant factors predicting for anaemia (r=0.318 and r2=0.101). We therefore conclude that high prevalence of infections and nutritional deficiencies are important risk factors for anaemia in this community. The high attributable fractions for hookworm, schistosomiasis, iron deficiency and vitamin A confirms that these are significant risk factors to be considered when designing public health measures for anaemia prevention in this community. Key words: anaemia, helminthes, nutrient deficiencies and dietary intake Introduction Like in many parts of the developing world anaemia in Tanzania is reported to affect mostly pregnant women and children below the age of five years (Schellenberg et al., 2003; TDHS 2005; Tatala 2004). Of the multiple causes of anaemia iron deficiency, which occurs when the iron in the body is insufficient to meet its requirements, is the major cause of iron deficiency anaemia. Anaemia is a known risk factor for long-term and even permanent impairment in mental and motor development in children (Nokes et al., 1998; Gratham-Mc Gregor et al, 2001) and could result in stunting and lowered resistance to infections when associated with iron deficiency (Gratham-Mc Gregor et al, 2001; Kahigwa et al, 2002). In this context severe anaemia in children is a factor that could affect cognitive function, motor performance and educational achievements as reported by Nokes et al., (1998). Iron and vitamin A deficiencies have been shown to be associated with anaemia in children in many parts of the developing world, in these areas it has been observed that these deficiencies are prevalent in areas where anaemia is also prevalent (Persson et al, 2000; Tarnumihardjo et al, 2004). The primary cause of micronutrient deficiencies includes disease, inadequate food intake, and low bioavailability of certain nutrients. For example when iron absorption is low from cereal-based diets this could be due to a high content of phytate, an inhibitor of iron absorption (Thu et al., 1999). Provitamin A carotenoids which is essential for vitamin A status in developing countries have generally low bio-accessibility due to inappropriate food processing methods that result into low retention and uptake of the vitamin (Mulokozi et al., 2003). In Tanzania the prevalence of anaemia in schoolchildren appear to be highest along the coast and lake zone areas, where over 60% of children are affected. (Hall et al., 2001; Ash et al., 2003). Though the rates of anaemia follow patterns of parasitic infections like malaria and hookworm (Hinderaker et al., 2001), which are also prevalent in respective areas (Premji et al., 1997; Persson et al., 2000), micronutrient deficiencies such as those due to consumption of diets with low iron bioavailability have been the most implicated cause (Tatala et al., 1998). Biological, socio-economic, cultural and dietary factors seem to be closely associated with anaemia (Szarfarc & Souza, 1997). Adequate nutrition status, which involves a balance between intake, assimilation and loss of respective nutrients, could therefore play a joint role in anaemia causation. In the tropics, infections can be a major cause of nutrient loss, are known to interfere with iron status of the community (Stoltzfus et al., 1997; Dreyfuss et al., 2000). Helminthic infections have a negative impact on micronutrient status of children due to loss of appetite and increased nutrient requirement (Fleming, 1981; Persson et al., 2000). The infections may aggravate the deficiency physically, or by increasing metabolic needs for essential nutrients (Bhargava et al, 2003). In order to investigate on health and nutritional risk factors for anaemia among school children living along the coast a survey was conducted in Tanga a region in Tanzania to form the basis for designing a package to facilitate appropriate school health intervention programmes in coastal areas. Materials and Methods Study area The study was conducted between March and May 1996 (a rain period) in villages in the districts of Tanga, Muheza, Korogwe, Lushoto Handeni and Pangani in Tanga Region of north-east Tanzania. This was part of the main school based public health intervention programme for anaemia and parasitic infections in school children. The area stretches from the coastline as low as 150m to as high as 2000m. The region covers an area of 60,000 km2 and the population of about 3 million people. There are four geographical zones representing different climatic, physical and weather conditions in different parts of the region. These include the coastal strip mostly parts of Tanga and Pangani, a wet hot and humid lowland area in much of Muheza, Korogwe and some areas of Lushoto, a dry lowland area in parts of Handeni and highland areas of Lushoto and stretching to the Usambara Mountains. From annual reports from the healthcare facilities in the study districts among the top ten listed diseases malaria, anaemia, acute respiratory infections and diarrhoeal diseases are common. Study subjects and design The study subjects were recruited among 965 children between 7 and 14 years of age representing a systematic (50%) sub sample from 20 randomly selected schools. Data for blood parameters and administration of questionnaires was obtained from 852 children. Children who were found to be severely anaemic (Hb<7g/dL) and seriously sick were referred to healthcare facilities for management and excluded from the study. A crossectional survey was used to assess the magnitude and causes of anaemia in the study population. Laboratory investigations Five millilitres of venous blood sample was collected using disposable sterile syringes from each of the 852 children. Part of the blood sample was used for the determination of haemoglobin, and the rest for serum ferritin (SF) and serum retinol (SR). The blood sample was left to clot at room temperature and then separated by centrifuging at 5000 rpm for 5 minutes to obtain sera. Haemoglobin (Hb) concentration was determined on whole blood from a venous sample and was directly measured in the field using a HemoCue haemoglobinometer (HemoCue, Angelholm AB, Sweden). The serum samples were stored at -400C until analyses were done within a month. The SF was quantitatively determined by Elegance Amplified Enzyme linked immunosorbent assay system using kits from Bioclone Australia Pty Ltd. SF samples were assayed in duplicates to measure within run precision, and an aliquot of pooled serum sample was used to measure interassay precision. Lymphochek control serum was used to assess accuracy and precision; the coefficient of variation was < 5%. Assay of SR concentration was done using High Performance Liquid Chromatography (HPLC) on Shimadzu RF 535 equipment with a fluorescence detector using C18 reverse phase column of 5µ (Speek, 1986). Serum CRP was analysed by the ELISA system based on the method developed by Naik & Voller (1984). The lower limit of detection was 7.8 mg/l. Fresh urine samples were collected from each child in a 20ml chemically clean universal glass bottle. Iodine concentration was determined using the persulphate digestion method (Pino et al., 1996). The urine samples were analysed in duplicates to check precision and the interassay coefficient of variation (CV) was <5%. For assessment of helminthic infections, containers were distributed to each child and were asked to bring a sample of their faeces to school the next school day. These samples were stained the same day and examined within one hour of staining using the Kato-Kartz method (WHO, 1994). Hookworm, Ascaris lumbricoides, Trichuris trichiura and Schistosoma mansoni ova were counted. Egg counts >8,000 per gram faeces (epg) the samples were re-examined after dilution of the sample and examined by Stoll concentration technique. Urine samples collected on the day of the survey were tested for micro-haematuria with Hemastix test strips (Ames Laboratories, Elkhart, IN). The haematuria positive samples were examined microscopically for determining egg counts for Schistosoma haematobium (Savioli & Mott, 1989). Physical examination and anthropometry A physician conducted physical examination and children were examined for pallor, fever, and splenomegally, signs of vitamin deficiencies including skin, thyroid gland enlargement, xerophthalmia, malnutrition and ill health. All those who reported to have been treated in the past one week or were on treatment for malaria were recorded. Children were weighed wearing light clothing and without shoes, and heights were taken at a specific place in the village where all children were assembled. A Soenhle 600 electronic scale (CMS Weighing Equipment, UK) and a fixed base portable stadiometer were used for weight and height measurement, respectively. Measurements for kg and cm were made to the nearest 0.1 unit. Age was calculated from the birth date on school records, based on birth certificates. Height for age and weight for age were expressed as z-scores with the US National Centre for Health Statistics (NCHS) median as the reference (Hamil et al., 1979). Dietary survey The school children were asked to recall the types of food consumed over the previous 24h and these were used to classify main foods and frequency of intake and according to their iron bioavailability as presented by De Maeyer et al. (1985) into meals with low (<30g meat or <25g ascorbic acid), medium (30-90g meat or 25-75g ascorbic acid) and high (>90g meat or >75g ascorbic acid) iron bioavailability. A questionnaire was used to obtain information on the knowledge, attitudes and practices of children on environmental sanitation, worms and dietary habits. For each child special data was collected for educational achievement and school performance. Data analysis Data entry and management were done using Epi Info programme. A statistical association between the different variables was made using SPSS 8.0. The z-scores were calculated using the anthroEpi-Info programme. Means of normally distributed variables were tested for significance by the Student’s t-test. Stunting was defined as a height for age z-score <-2. To define wasting body mass index less than 5th centile (BMI; weight (kg)/height (m2) was used. Hb defined anaemia by levels below 115g/L for age less than 12 years and below Hb 120 g/l for age 12 years. Mild anaemia was defined by Hb levels from these cut-off levels to 100g/l. Levels less than 100 g/l and 70g/l or above were categorised as moderate. Severe anaemia was Hb <70g/l. SR levels <20 µg/dl was used to define vitamin A deficiency, and SF <12µg/l defined depleted iron stores while SF < 20 µg/l defined iron deficiency erythropoiesis. Iodine deficiency was defined as urinary iodine concentration of less than 100 µg/l (moderate to mild deficiency) and severe deficiency as <20 µg/l. Infection status was defined by a positive finding in stool or urine, and a serum CRP above 5.5 mg/l (Hjortdahl et al., 1991). All children found with severe anaemia and a serious ill health was referred to a nearby Health Centre or Hospital for treatment. Data for general socio-economic status, multiple parasitic infections, and a summary of knowledge on general health were aggregated to form composite scores. Chi square tests were used to test differences in proportions and risk ratios within 95% confidence interval. If data were normally distributed differences in means were tested for statistical significance using Student’s t-test. The non-parametric data were calculated using the Mann-Whitney U-Test. To assess the effect of independent variables a multivariate analysis was used using a general linear model. Ethical considerations The study was fully explained to subjects before verbal consent was obtained from parents and the research and ethical committee at the Tanzania Food and Nutrition Centre approved the study. Results Anaemia and nutritional characteristics The prevalence of anaemia in study children was 79.6% (n=852) with a mean haemoglobin (Hb) concentration of 107± 15 g/L. The female to male ratio was 1:0.98 and the mean age of younger children was 9.5± 1.0 years and of older children was 12.7± 0.6 years (Table 1). The overall prevalence of anaemia did not differ by gender and overall 1.3% children were severely anaemic. There was a significant difference between mean Hb in children below 12 years (n=439) and those above (n=406), 106 vs 109 g/L respectively. Prevalence of anaemia was 83.2% in young and 75.6% in older age group. Mean haemoglobin concentrations was significantly lower in the younger age group and in children with low weight for age z-scores as well as low arm circumference were significantly lower than in children with normal values (P<0.01). Over 80% of the children were stunted (low weight for age) but mean Hb in stunted was not significantly different (107 vs 108 g/L) from that of non-stunted children. Distribution of iron, vitamin A and iodine deficiencies The overall prevalence of iron deficiency was 32.7% and that of vitamin A deficiency was 31.9% with 3.5% schoolchildren having marked deficiency (Table 2). Mean serum ferritin concentration was 28± 15 µg/L and mean serum retinol was (25± 11µg/L) and was significantly lower in children below age 12y (24± 11 vs 26± 10µg/L respectively; P=0.036). Nutrition, diseases and socio-economic factors The distribution of nutritional indices such as underweight and stunting were different between the younger and older age groups (P<0.05). The proportion of children who were stunted was higher in older than in younger age (81% vs 62%) (Table 3). For helminthic infections the younger children had significantly higher prevalence of ascariasis than older children (20% vs 14%) who had a higher prevalence of schistosomiasis than their younger counterparts (58 vs 50% respectively) P=0.001. Overall nutritional indicators showed significant lower mean values in younger children than older. Underweight and stunting were highly prevalent in older groups who also had a high prevalent of schistosomiasis. Multiple infection rank score was higher in older than in young children. Socioeconomic conditions and school achievement were similar for all children. Risk factors for anaemia The risk of all anaemia forms had strong associations with iron deficiency, ascariasis, schistosomiasis, vitamin A deficiency and underweight in descending order of relative risk (Table 4). However, population attributable risk (PAR) percent was highest with schistosomiasis, iron and vitamin A deficiencies and underweight. Again when iron deficiency anaemia was considered the risk was highest for schistosomiasis, ascariasis, hookworm, and underweight. Schistosomiasis and hookworm had the highest PAR percent followed by underweight and vitamin A deficiency. In a stepwise multiple regression analysis with haemoglobin as the dependent factor (Table 5) schistosomiasis and hookworm were further confirmed to be significant factors influencing the haemoglobin status (P<0.05). Low weight for age z-scores and serum ferritin were the nutritional risk factors retained in the regression model and were also significantly predicting for haemoglobin status (P<0.05). The regression coefficient (R) for the dependent factor haemoglobin in the model was (R=0.323, R2=0.104) and (R=0.256, R2=0.07), respectively. In the model both schistosomiasis and hookworm were significant factors. Prevalence of nutritional deficiencies The proportion of children with anaemia was significantly higher in the wet lowland area (Table 6). A similar distribution was reflected for nutritional deficiencies and the coastal strip was having the lowest prevalence of these factors. Hookworm prevalence was lower in children in the coastal strip than in wet and dry lowland areas. The prevalence of iron deficiency and underweight were, however, significantly higher in the wet lowland areas (P<0.001). The intensities of hookworm ova (eggs counts per gram (epg) faecal matter) in specimens of children living in the lowland areas were significantly higher than in children from other areas (874 vs 604 epg; P<0.06). Feeding habits of schoolchildren The 24-hour dietary recall showed that majority (n=695 {89.4%}) of these children depended on cereal and vegetable based diets. Red meat intake was less frequent and fruits were not common in their meals. More than 60% of children were coming to school without taking breakfast (Figure 1). While at school none had lunch or snacks arranged or prepared by the school (i.e. no school feeding programme). There were no statistically significant differences between caretakers (i.e. guardians or parents) for the provision of breakfast or money (P>0.05). Discussion The objectives of the present study were to determine the risk factors for anaemia among schoolchildren living along the coast in rural Tanzania. This was to assist in designing appropriate measures. In accordance with the available data from literature anaemia is highly prevalent among school children and this study confirms that. The baseline characteristics show that nutritional deficiencies are also equally prevalent. It should be borne in mind that this was a convenient sample drawn from a group of children who are in schools. This could have underestimated the true prevalence of anaemia since these children being in schools are in a better position to understand the health and nutritional risk factors since this could be taught in schools. In other aspects the rate could be explaining the effects of short-term hunger and inadequate dietary intake, since many of these children came to school without taking breakfast and spent most of their day in school. A synergistic effect of micronutrient deficiencies and hunger could be responsible for the high prevalence of anaemia in them. Similar findings have been reported from studies in Bangladesh and South African school children (Persson et al., 2000; Jinabhai et al., 2001). Since nutritional anaemia is caused by a diet containing low amounts of bioavailable iron or inadequate dietary iron intake it is possible that the anaemia observed could be originating from nutritional causes as shown by the irregularities on food intake and the type of iron mostly consumed. Intake of diet with a high amount of non-haem iron could have been the reason for such an inadequate intake. The 24-hour dietary recall revealed a predominant intake of cereal and vegetable based diets. The net effect of different dietary factors for such diets is either enhancing or inhibiting the absorption of non-haem iron, and this could have an impact on iron nutrition and hence anaemia status. Phytate and tannins in food inhibit the non-haem iron absorption while ascorbic acid and meat influence that absorption positively (Hallberg & Hulthen, 2000). Haem iron absorption does not depend on the composition of diet in a similar manner and thus up to 30% of this iron in diet can easily be absorbed (Layrisse et al., 1984). Looking at the diet of these children as reported in the 24 hour dietary recall, it can be categorised as the moderate to low iron bioavailability diet (De Maeyer et al., 1985). From all the above, it can be drawn that iron deficiency could be a significant cause of the anaemia in them. Our findings of low mean Hb in the younger children and the history of short term hunger, especially for those who misses their breakfast or do not take enough for lunch due to financial constraints, a high prevalence of anaemia is a possible long term effect of low iron intake and high physiological needs. Additional iron is required during children growing period for increasing muscle mass and for the adolescent growth spurt. When the diet of these children is lacking the essential minerals and vitamins or when these are marginalized in their diet the observed nutritional deficiencies are likely to occur. The significantly lower haemoglobin levels found in underweight children and in children with vitamin A deficiency further suggests that the anaemia found could be diet related. In studies elsewhere vitamin A status has been found to influence positively the iron status (Dreyfuss et al., 2000; Persson et al., 2000; Tanumihardjo et al., 2004). Iodine deficiency in the present study was not correlating to anaemia, this could be due to the national efforts which had been started with legislation to make sure that all people in Tanzanian communities take fortified (iodated) salt as an essential nutrition action (Kavishe et al., 1993). A study in Mpwapwa (Ash et al., 2003) reported much lower rates of iron and vitamin A deficiencies among schoolchildren than in the present study. The differences observed between the two studies may be insignificant due to the different geographical locations of the two studies and different disease patterns. The former study was conducted in a semi-arid plateau region about 1000 meters above sea level compared with this one in the coastal areas. However, a recent study by Mulokozi (2003) showed that the semi arid areas in Tanzania have a higher prevalence of vitamin A deficiency than other parts. Since serum ferritin can be elevated as a result of infection or inflammatory conditions the iron deficiency rates in the two studies based on serum ferritin levels could also have been influenced by the disease pattern. There being no reliable feeding programme in these schools, inadequate diet and hence inadequate dietary iron intake could further be contributing to low iron stores with repercussions on academic achievement. Anaemia results from multiple causative factors and this is well shown by the results from this community. As observed in this study parasitic infections also play a significant role in anaemia causation in both young and older children. More than a half of the investigated school children had parasitic infections and older children appeared to be most affected. Hookworm and schistosomiasis, which have been found to correlate significantly with anaemia in these children, are the main causes of haemorrhagic anaemia (Prual et al., 1992). These infections have been an implicated cause of anaemia in many parts of the developing world (Bhargava et al., 2003). Malaria is also highly prevalent in these children as reported in illness histories by one third of the study children that showed they have been treated for malaria in the past one week. Population attributable risk of anaemia in children from this community show that underweight, iron deficiency and vitamin A deficiency are of public health importance and require interventions for up to 19% of the people. The socio-economic conditions in the studied population did not appear to have a direct influence on anaemia. However, being coming from predominantly middle or low SE strata (based on family possessions and purchasing power of schoolchildren for daily snacks) this could be an important risk factor influencing family per capita. Family per capita has been shown by studies elsewhere to be the main distal determinant in causality models of anaemia (Silva et al., 2007). When all the anaemia forms were considered a strong association was observed between anaemia and helminthic infections. The relative risk of having anaemia in children was higher with schistosomiasis and ascariasis. However, only schistosomiasis among the diseases was having a high population attributable risk. This was also observed in children with iron deficiency anaemia where the schistosomiasis was having the highest attributable fraction. Hookworm infection was also having a higher attributable risk percent for iron deficiency anaemia compared with ascariasis. Hookworm and schistosomiasis have been shown by studies among African children to be a common cause of iron deficiency due to the loss of blood they cause (Stoltzfus et al., 1997). There is a high possibility that the high rates of nutritional deficiencies noted in these children is a vicious cycle resulting from the high prevalence of geohelminths found in the study areas. The high intensities of hookworm observed are also explaining the high risk of children with iron deficiency to anaemia a factor also noted in schoolchildren by Stoltzfus et al. (1997) in Zanzibar. High prevalence of helminthic infections has also been shown to be associated with malnutrition in children in studies in Kenya (Stephenson, 1993). Children with Ascaris lumbricoides were also shown in the present study to have a raised relative risk of having iron deficiency anaemia. A. lumbricoides do not suck blood but their association with iron deficiency anaemia has also been reported in studies elsewhere and the explanation to their effect has been suggested to be a non specific lowering of haemoglobin during infection-the so called anaemia of chronic disease (Ulukanligil & Seyrek, 2004). Infections are known to flourish well in children with vitamin A deficiency since the latter is important in maintaining cell integrity and immune functions in the body. The anaemia of chronic disease could also exist in our study area due to infections such as malaria, which is endemic in the northern coast of Tanzania (Mboera, 2000). Malaria was not measured in the present study however; on clinical examination 38% of the children gave a history of a febrile illness suggestive of malaria. Malaria parasites can cause haemolytic anaemia, megaloblastic anaemia (due to folic acid deficiency) or iron deficiency anaemia due to the associated diserythropoiesis (Premji et al, 1997). Multivariate analysis also showed hookworm and schistosomiasis as significant factors predicting for anaemia in the study children. The geographical zones in the study area appear to have a bearing on the distribution of the nutritional deficiencies and diseases. The nutritional deficiencies of iron, vitamin A and iodine as well as underweight, had the highest prevalence in the wet lowland areas where the anaemia prevalence was highest (P<0.01). The low weight for age observed could be related to dietary inadequacy or to the high prevalence of diseases. The high prevalence of diseases in the lowland areas could be a factor influencing negatively the nutritional status of these children. Studies elsewhere have shown an association between micronutrient deficiencies and parasitic infections (Stoltzfus et al., 1997; Dreyfuss et al., 2000). The conditions in the wet lowland and parts of the dry lowland areas are favourable for disease propagation due to the humidity, good loamy soil and pockets of water that are suitable for helminthic infections and breeding places for malaria vectors. Anaemia prevalence varies in different parts of the world (De Maeyer et al., 1985). Among the factors that influence its distribution include the geographical zones. Though this could not be a general inference with regard to the relationship with anaemia prevalence, there is a general tendency for anaemia to be associated with the high prevalence of parasitic infections including malaria. In different geographical areas the disease as well as dietary pattern differs and these factors as well as socioeconomic factors, in one way or another influence the prevalence of anaemia. The zones in this study had significant differences in anaemia prevalence with a significantly lower mean Hb level in the wet lowland area. In conclusion the findings in this study show that anaemia affects more than a half of school children in this northern coastal area of Tanzania. The anaemia observed is associated with multiple risk factors ranging from biological, dietary and socio-cultural factors that can be intervened by public health measures. Thus it is recommended that when designing measures for prevention of anaemia in school health programmes, interventions targeting both nutritional deficiencies and parasitic infections should be employed. Acknowledgements This work was carried out through support by the Edna Mc Connell, James McDonnell and the Rockefeller Foundations, and the United Nations Development Programme and in part by the International Program for Chemical Sciences, Uppsala University in Sweden. The authors wish to thank all those who participated in the study; the Tanzania Food and Nutrition Centre, UKUMTA in Dar es Salaam and the District personnel in Tanga region of Tanzania. We highly appreciate the efforts made and participation by teachers, parents and children in study areas. References
© Copyright 2008 - Health User's Trust Fund (HRUTF) The following images related to this document are available:Photo images[th08031t4.jpg] [th08031t6.jpg] [th08031t2.jpg] [th08031t5.jpg] [th08031f1.jpg] [th08031t3.jpg] [th08031t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}