 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
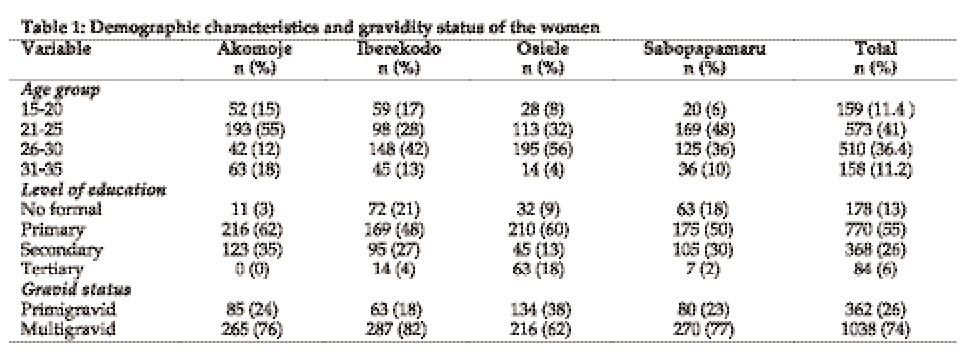
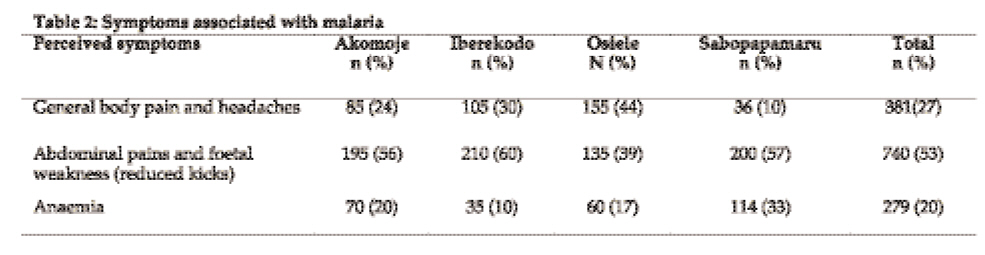
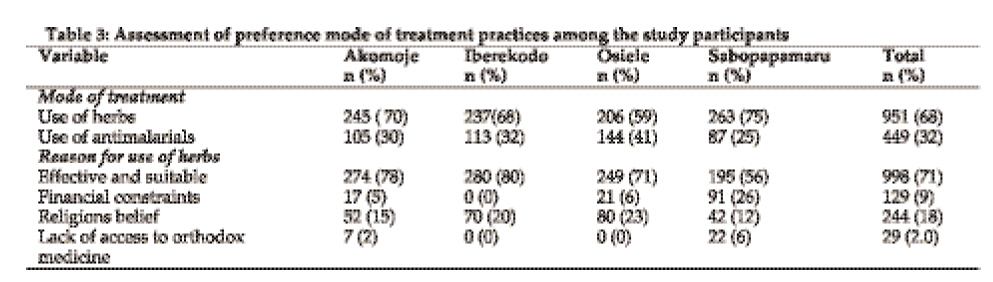
Tanzania Journal of Health Research, Vol. 10, No. 4, Oct, 2008, pp. 226-231 Knowledge and practices on malaria treatment measures among pregnant women in Abeokuta, Nigeria S.O. Sam-Wobo1*, T. Akinboroye1, J.C. Anosike2, and B. Adewale3 1 Department of Biological Sciences, University of Agriculture, PMB 2240, Abeokuta, Nigeria 2 Department of Animal and Environmental Biology, Imo State University, Owerri, Nigeria 3Public Health Division, National Institute for Medical Research, Yaba, Lagos, Nigeria Received: October 19, 2007 Revised 21 January 2008 Accepted 20 June 2008 Code Number: th08035 Abstract The knowledge and practices on malaria treatment measures were assessed among 1400 pregnant women in semi-urban and rural communities (Akomoje, Iberekodo, Osiele and Sabopapamaru) of Abeokuta, Nigeria in 2006. Data was collected using structured questionnaires and focus group discussions. The largest proportion (41%) of the respondents was in the age group 21-25years. About three quarters (74%) of the women were multigravids. Sixty-five percent of the women had between three to four episodes of malaria per year. According to the respondents, symptoms associated with malaria in pregnancy included abdominal pains and foetal weakness due to reduced kicks (53%), body pains and headaches (27%) and anaemia (20%). Sixty-eight percent of the pregnant women utilized herbs for treating symptoms associated with malaria due to its effectiveness and suitability and not due to financial constraint or lack of access to health facility. Though most women utilized herbs, 32% relied more on the use of antimalarials. Sulfadoxine-pyrimethamine was the preferred antimalarial during pregnancy at the 2nd and 3rd trimesters. Only 15% of the women were using insecticide treated mosquito nets for personal protection. The majority (77%) of respondents used nylon net to screen their windows off mosquitoes. Since malaria poses adverse effect on the mother and developing foetus, health education becomes very essential to the traditional birth attendants and the women who patronize them. Pregnant women who attend traditional birth homes should be encouraged to also attend orthodox antenatal clinics, in order to receive proper and adequate treatment against malaria for themselves and the foetus. Keywords: Malaria, prevention, treatment, pregnant women, Nigeria Introduction Malaria remains a major public health problem in sub-Saharan Africa, with 80% of malaria cases and 95% of malaria mortality worldwide occurring in this region (WHO, 1996; Snow et al., 1999). It is estimated that 90% of the annual 500 million cases of malaria occur in sub-Saharan Africa, where 1.5-3.0 million annual deaths are due to malaria (http://www.malaria.org). In Africa, an estimated 24 million pregnant women are threatened by malaria, which not only affects their health but also causes poor pregnancy outcomes (WHO, 2002). In Nigeria, about 50% of the population experience an episode of malaria annually, with under-five children and pregnant women at greater risk of the disease (FMoH, 2004). Malaria accounts for 11% of the maternal deaths in Nigeria (FMoH, 2004). Malaria in pregnancy can lead to abortion, stillbirth, intra-uterine growth retardation, low birth weight, premature labour and even maternal death (Kochar et al., 1999). Hence the condition needs to be treated and prevented as a matter of routine in all women at risk of infection (Schulman, 1999). The effect of malaria in pregnancy is more pronounced among primigravids than multigravids (Brabin, 1993). This is mainly due to the development of new uteroplacental vasculature in pregnant women especially at their first pregnancies which had no previous exposure to malaria infection and are thus immunologically naive, permitting parasite colonization. Considering the problems associated with malaria in pregnancy, the World Health Organization (WHO, 2001a) adopted the intermittent preventive treatment for malaria in pregnancy (IPTp) as one of the main strategies to reduce the morbidity and mortality of malaria. It is based on the assumption that every pregnant women living in an area of stable or unstable malaria transmission could harbour malaria parasite in the peripheral blood or placental (Le Hesran et al., 1997; Mwangoka et al., 2008), and therefore should be treated to minimise its effect on the mother and the foetus (WHO 2001a). Van Eijk et al (2004) opined that IPTp had a beneficial impact on mother and infant health by significantly reducing the maternal anaemia, placental parasitaemia, and low birth weight. In a number of countries in the tropics, multi-drug resistance of Plasmodium falciparum is common. This has led to new therapeutic approaches, such as artemisinin-based combination therapies, which are being promoted in such areas as effective first line treatment together with appropriate support such as microscopy and rapid diagnostic tests. In several East African countries, single-dose sulfadoxine-pyrimethamine is being adopted as first-line treatment, on account of its low cost and ease of use. However, growing resistance to this drug in some countries in Africa, including Nigeria, led to concern that its usefulness will be time-limited. Effective but more expensive artemisinin-based combination therapies are being introduced by roll back malaria (RBM) partners as part of national antimalarial drug policies (WHO, 2001b). In spite of its beneficial attributes, intermittent preventive treatment as initiated by RBM is confronted with some setbacks, which are linked to its low acceptance by some pregnant women, high cost of drugs and the development of adverse reaction after medication or treatment, and has contributed to some pregnant women devising alternative preventive treatment measures. This study was therefore carried out to assess the knowledge and practices of pregnant women in semi-urban communities on malaria treatment measures in Abeokuta, Nigeria. Materials and Methods Study area and data collection The study done in 2006 was carried out in four selected farming communities namely Akomoje, Iberekodo, Osiele and Sabopapamaru of Abeokuta, a rainforest belt of Nigeria which lies approximately between longitude 2°30/ and 4°30/E and between latitudes 6°30/ and 8°N. The study areas were stratified into geo-developmental settings (semi-urban and rural), types of schools present, and access to traditional or orthodox health facilities. Akomoje, Iberekodo and Osiele are semi-urban communities with presence of primary and post-primary schools and access to orthodox and traditional health facilities. Sabopapamaru, a rural community with presence of primary and post-primary schools has access only to traditional health facility The pregnant women were recruited by the formal gathering of women initiated by the traditional rulers of each community. Structured questionnaires on the cause, transmission, symptoms, treatment, control of malaria and its effects on pregnancy were obtained from pregnant women from each community who enrolled for the study. Other information sought included age, level of education, and gravidity status. Written informed consent of the traditional rulers and the pregnant women consent was obtained before questionnaire administration. Data analysis Standardized data entry formats were developed using MS Excel format. Distribution of prevalence was analysed with contingency tables and Chi-Square tests. Analyses into percentile and the assessment of the relationship between the variables and for significance were done using SPSS ver. 10. Results A total of 1400 (350 from each village) women were included in this study. Most (77.4%) of the respondents were in the age group 21-30 years. The largest proportion (55%) of the respondents had attained primary school education. The study further observed a 74% level of multigravids than primigravids in the study population (Table 1). Between 41-80% of the respondents in the different communities believed that malaria is caused by mosquito bites. Sixty-five percent of the women claimed to experience three to four episodes of malaria disease in a year. Abdominal pains and foetal weakness due to reduced kicks (53%), body pains and headaches (27%) and anaemia (20%) were the symptoms associated with malaria in pregnancy (Table 2). Abdominal pains and reduced foetal kicks were the most common symptoms in all villages except in Osiele. The study observed that 68% of pregnant women utilised herbal treatment as a means of treating symptoms associated with malaria (Table 3). This they attributed to its effectiveness and suitability. Financial constraint and lack of access to health facility were not the reasons for the choice of traditional herbal treatment but its efficacy. On average, sulfadoxine-pyrimethamine (42%) was the preferred antimalarial used during pregnancy. Other antimalarial drugs included chloroquine (30%) and daraprim (pyrimethamine) (28%). However, there was variation between villages on the preference of antimalarial drugs. Sulfadoxine-pyrimethamine was the most preferred drug among women in Osiele (68%) and Iberekodo (46%). Chloroquine was the most preference drug in Akomoje (44%) while daraprim in Sabopapamaru (52%). It was observed that 54% of respondent used the herbal drugs daily. This was due to the belief that daily intake in addition to forestalling attacks of malaria keeps the foetus in good condition. The utilization of antimalarial drugs during the 2nd and 3rd trimesters had the second highest value of 19%. This is an indication that some respondents who attend antenatal clinics combine both the herbal treatment regimes with sulfadoxine-pyrimethamine (used for IPTp). Taking of drugs twice daily, when symptoms occur and every Sunday was mentioned by 12%, 5% and 10%, respectively. Utilisation of insecticide treated mosquito nets by pregnant women was very low (15%). Respondents were of the opinion that mosquito nets do not provide good personal protection and yet they disturb the sleeper from getting fresh air. Seventy-seven of the respondents mentioned do have their houses screened with mosquito gauze. Discussion Results from the study indicate varied knowledge on the transmission of malaria among the respondents in the different communities. The commonest associated symptoms of malaria in pregnancy were abdominal pains, foetal weakness, body pains, headaches, and anaemia. In another survey carried out among rural communities of Abeokuta in Nigeria, majority of the respondents (73%) attributed malaria infection to doing of strenuous jobs in the hot sun, while only a small proportion (11.7%) attributed it to mosquito bites (Idowu et al., 2003). Like in our study, it has already been reported that communities in Abeoukuta have good knowledge of malaria symptoms even in infants and children (Idowu et al., 2003). In contrary, other studies in Nigeria have revealed a lack of knowledge on the cause of malaria and many misconceptions about the transmission and treatment of malaria (Erhun et al., 2004; Wagbatsoma et al., 2004). The demographic and gravidity status showed that multigravids were more than primigravids in addition to also the age group 21-25years. This could be due to the fact that semi-urban and rural women marry early which maybe due to cultural and occupational beliefs where childbearing is perceived to occur early and the offspring’s helps out in the family occupation. The significant variation in the level of education among pregnant women in the study (with most of them having only attained primary school education) may have an impact in the adoption and implementation of various malaria control measures (WHO, 2001b). The choice of herbal treatment for treating symptoms associated with malaria was observed in the study to be high. It was interesting to note that neither financial constraint nor lack of access to health facility were the reasons for the choice of traditional herbal treatment as reported in a study by Erhun et al. (2004). In another study in Benin City, Nigeria, most of the respondents were found to prefer orthodox drugs for home treatment of malaria with only 3.3%-5.8% using herbal preparations (Wagbatsoma et al., 2004). Like in our study, the use of choloroquine and sulfadoxine-pyrimethamine in home management of malaria by the general population was common (Wagbatsoma et al., 2004) during the period of the study. The frequency of daily herbal drugs usage observed from the study is attributed to the treatment regime. There is the belief that daily intake forestalls attacks of malaria and also keeps the foetus in good condition. In a recent study in Nigeria, Idowu et al. (2003) reported that in the event of malaria infection, consumption of herbal preparations is the first line of treatment and that hospital visit was usually after many days of persistent illness without improvement despite all forms of self medication. The high preference of sulfadoxine-pyrimethamine among pregnant women observed in this study was not surprising. The current strategy for malaria control in pregnancy is intermittent preventive treatment (IPT). This is an approach whereby pregnant women are treated for malaria presumptively with curative doses of effective antimalarials at regular intervals during the second and third trimester (WHO, 2000). A recent study in Nigeria has shown that IPT with sulfadoxine-pyrimethamine is an effective practicable strategy to reduce risk of anaemia in low parity groups living in malaria endemic areas (Asa et al., 2008). Personal protection and vector control measures using insecticide-treated mosquito nets have proven highly efficacious in reducing morbidity and mortality in areas of high, moderate and low malaria transmission. However, net utilisation by the respondents was very low. This low net coverage was said to be associated with the common belief among he community that that nets do not provide good personal protection and disturb the sleeper from getting fresh air. Similarly, in another study in Abeokuta, Nigeria, none of the respondents was found to use mosquito nets (Idowu et al., 2003). Although the majority of the respondents claimed to use nylon net to screen their windows off mosquitoes but due to the heat in the house at night, most women prefer to open the door of houses and windows at night with their bodies exposed to fresh air. Like in our study, the prevention against malaria was observed by Wagbatsoma et al. (2004) in Benin City to be mostly achieved through the use of door/window gauze. Since malaria poses an adverse effect on both the mother and the developing foetus, health education is therefore a very important strategy in educating the people on the dangers posed by malaria disease. Traditional birth attendants should be educated on the effects of malaria in pregnancy since some pregnant women patronize them. Pregnant women who attend traditional birth homes alone and practice self-medication should be encouraged to also attend orthodox antenatal clinics, so as to receive proper and adequate treatment against malaria for themselves and the developing foetus. Acknowledgements We appreciate the chiefs and people of Akomoje, Iberekodo, Osiele and Sabopapamaru for their support and cooperation during the study. References
© Copyright 2008 - Health User's Trust Fund (HRUTF) The following images related to this document are available:Photo images[th08035t2.jpg] [th08035t1.jpg] [th08035t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}