 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
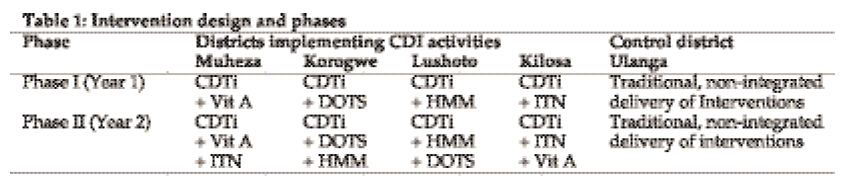
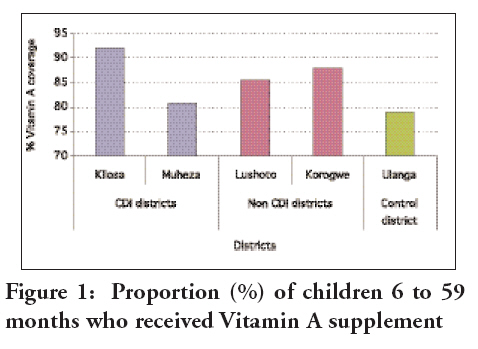
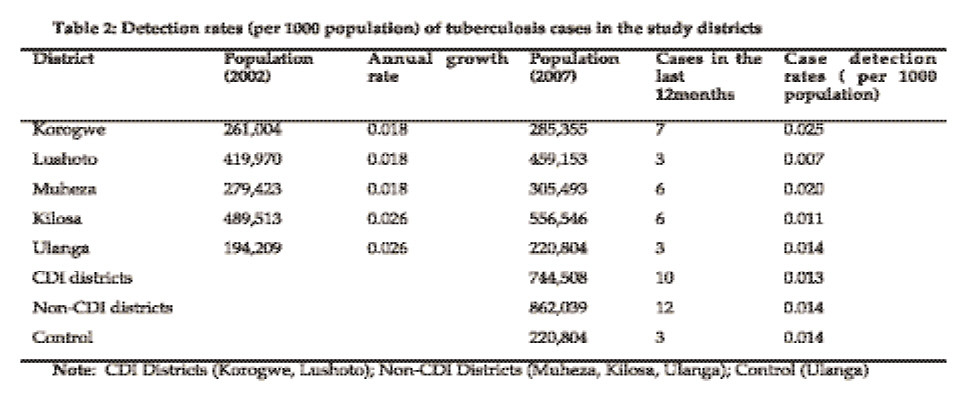
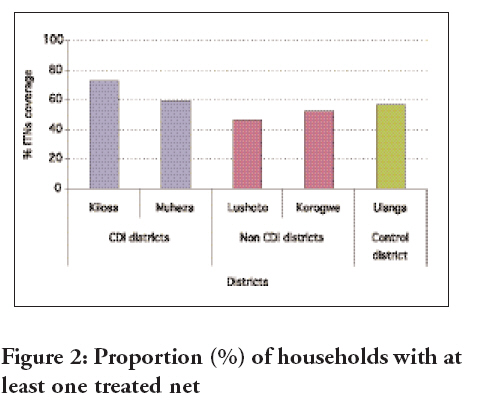
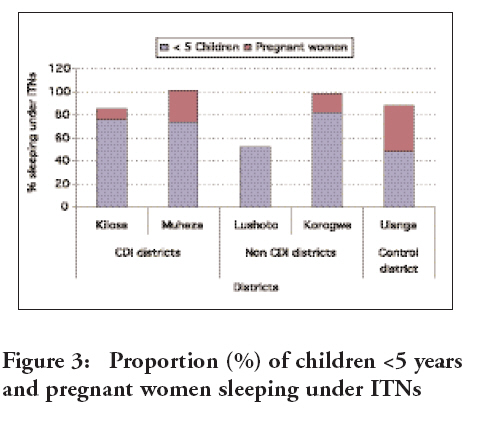
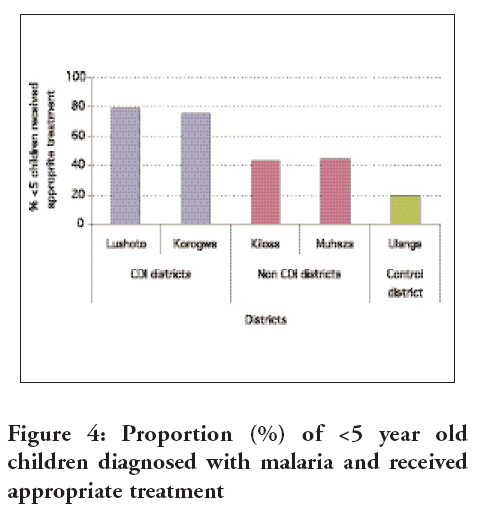
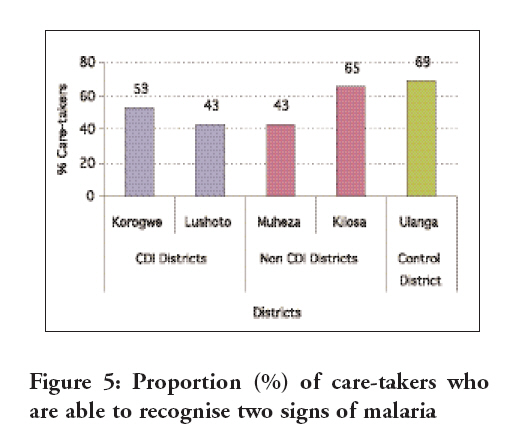
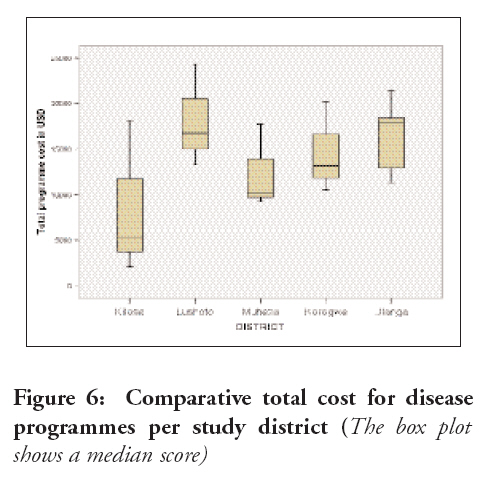
Tanzania Journal of Health Research, Vol. 10, No. 4, Oct, 2008, pp. 232-239 Community directed interventions for malaria, tuberculosis and vitamin A in onchocerciasis endemic districts of Tanzania W.N. Kisinza1*, W.J. Kisoka2, P.P. Mutalemwa3, J. Njau4, F. Tenu1, T. Nkya1, S.P. Kilima3 & S.M. Magesa1 1Amani Medical Research Centre, P. O. Box 81, Muheza, Tanzania Received 13 August 2008 Revised 4 September 2008 Accepted 5 September 2008 Code Number: th08036 Abstract In recognising the success attained through community-directed treatment with Ivermectin, there has been a growing interest to use a similar approach for delivery of interventions against other communicable diseases. This study was conducted in 2007 to evaluate the impact of community directed intervention (CDI) on delivering five health interventions namely Vitamin A supplementation (VAS), community-directed treatment with Ivermectin (CDTi), distribution of insecticide-treated nets (ITN), directly observed treatment of tuberculosis (DOTS), and home-based management of malaria (HMM). The study was carried out in onchocerciasis endemic districts of Kilosa, Muheza, Lushoto, Korogwe and Ulanga districts in Tanzania. A total of 250 households were involved in the study for the period of two years. During the first year, one new intervention was added in each study district. A second new intervention was then added in the same manner during the second study year. In the control district all interventions, with the exception of Ivermectin distribution, continued to be delivered in the traditional manner throughout the study period. Results showed that Ivermectin treatment coverage in the CDI districts (88%) was significantly (P<0.005) higher than in the control district (77%). The coverage of VAS was 84 ± 7%, showing very little difference between control and intervention districts (P>0.05). The DOTS treatment completion rate was observed only in Korogwe where 4 out 7 patients had completed their treatment. The proportions of pregnant women and <5 years children sleeping under ITN in the CDI districts (range: 83-100%) were significantly higher (P< 0.05) than those in the control district (40-43%). There was also a higher proportion of malaria cases referred in the intervention districts (42%) than in the control district (21%) (P<0.005). Likewise, the proportion of <5 years children who were presumptively diagnosed with malaria and received appropriated treatment within 24 hours in the intervention districts (17-29%) was higher than those in the control district (4%) (P<0.005). The costs incurred per integrated programme in the intervention districts were much lower than those in the control district. In conclusion, our results showed higher coverage of interventions in the CDI districts without necessarily increasing the cost. Key words: Community directed intervention, malaria, tuberculosis, vitamin A, Tanzania Introduction African countries are faced with a number of health problems, which complicate their development programmes. Studies have underscored the impact of communicable diseases such as malaria, onchocerciasis, tuberculosis and blindness on productivity consequently leading to poor quality of life. Control of these diseases has been hampered by several factors including climatic factors, poor environmental sanitation, cultural habits, poverty and inadequate health delivery system. A series of research in the past decade identified mass distribution of Ivermectin in onchocerciasis endemic countries using the Community Directed Treatment with Ivermectin strategy (CDTI) as one of the effective approaches to controlling the socio-economic impact of the disease in Africa. The major challenge then, was to deliver annual Ivermectin treatment to all targeted communities and to sustain high treatment coverage over a very long period. To achieve this, the African Programmes for Onchocerciasis Control (APOC) adopted this strategy which for years has proven to be very effective in delivering Ivermectin to the target population (Amazigo, et al, 2007; Okeibunor, et al, 2004; Remme, 2004; TDR, 1996). In recognising the success attained through CDTI, there has been a growing interest at the national and international levels to use the same approach for delivery of interventions against other diseases threatening the development of African countries. This was also seen as an important opportunity to integrate Ivermectin treatment with other disease control activities for the sustainability of APOC assisted CDTI projects in Africa. But to ensure that this opportunity is properly exploited and based on sound scientific data, there was an urgent need to gather good scientific evidence on the effectiveness of the Community Directed Intervention (CDI) process against other diseases and for integrated disease control at the community level. The current multi-country study was therefore initiated on this basis. The main objective was to determine the extent to which the CDI process, currently used for onchocerciasis control in Africa can be used for the delivery of other health interventions. Specifically, the study sought to (i) document the CDI process for the integrated delivery of Ivermectin treatment, Vitamin A, insecticide treated nets (ITN), directly observed treatment short term (DOTS) and home-based management of malaria (HMM); (ii) determine the effectiveness of the CDI process for the delivery of interventions with different degrees of complexity; (iii) identify the critical factors that facilitate or hinder the CDI process and integration from achieving the desired outcomes for the interventions. Materials and Methods Study areas The study was conducted in Morogoro and Tanga Regions of Tanzania where a total of five districts were chosen on the basis of onchocerciasis endemicity and with APOC supported projects. In Tanga Region (4°to 6°S and 37°to 9°E) in north-eastern Tanzania, three districts namely, Lushoto (4°20/S; 38°00/E), Korogwe (5°9/ S 38°29 / E) and Muheza (39°0 /E; 5°0 /) which are hyper/meso endemic for Onchocerciasis, were selected. In Morogoro (6°49/ S, 37°40/ E), two districts, namely Kilosa (36°30/ S and 37°30/E) and Ulanga ((8°06/S, 36°41/E)) endemic for onchocerciasis and with functional APOC supported projects were included in the study. These districts were selected purposively to give the fourth intervention arm as well as control arm of the study. Ulanga district served as the control arm for this study, where all the interventions were implemented in the traditional form with the exception of Ivermectin distribution. The target population for the study, in all the districts were the stakeholders in the intervention processes. These included intervention programme managers, policy makers at the different levels of the delivery of the intervention, community leaders and their volunteers as well as household members in the respective study communities. Study design and population This prospective operational research employed an assessment of pre- and post-intervention situations, thus giving elements of experimentation (with intervention and control arms) in the study. Elements of case study research were also included in that full documentation of intervention processes and responses were undertaken to ensure full explanation of how and why the CDI process works or does not. The study focused on the district as the unit of intervention and analysis. The study allowed an assessment of the effectiveness and efficiency of CDI in relation to the complexity of individual and different combinations of interventions Ten communities from each district were randomly selected making a total of 50 communities from which five households were randomly selected to obtain a total of 250 households in each year of the two year-study period. During the first year, one new intervention was added in each trial district. A different intervention was introduced to each of the four trial districts. A second new intervention was then added in the same manner during the second year. In the control district all interventions, with the exception of Ivermectin distribution, continued to be delivered in the traditional manner throughout the study period (Table 1). Intervention and evaluation process During the intervention process, the roles of the community were to (i) collectively design the approach to implementing the intervention in the community and identify the resources within the community; (ii) collectively plan how, when, where and by whom to implement the intervention, supervise and decide what support to provide to the implementers and how to monitor the process; (iii) select a member of the community who will provide the service and be directly responsible to the community in implementing the intervention plan; and (iv) collectively discuss the results of the monitoring and adjust the implementation strategy accordingly. The implementation was preceded by meetings with key stakeholders at all levels (national, district and community). Representatives from all national disease control programmes were included in the planning and implementation meetings. These included the National Malaria Control Programme, National Tuberculosis and Leprosy Programme, National Onchocerciasis Control Programme and Vitamin A Supplementation Programme. The districts were represented by the Council Health Management Team members and focal persons of each of the CDI target interventions. The meeting provided an opportunity to update the district teams on the CDI process and their roles in the implementation. District commitment was made, with a clear understanding of what is expected from them. Support was provided for the teams to put together a framework for their respective district CDI plans. Having concerned with the community leadership, the next step was public meeting of entire communities. During the meetings, the information and much of the process was discussed with the community leaders with emphasis on mobilization and sensitization of communities on the benefits of the interventions. The Community Directed Distributors (CDDs) as well as community leaders were trained on the methods of service delivery (regimen, frequency of dosage in case of drugs, exclusion criteria, adherence to regulations, recognition and management of adverse reactions, recordkeeping and reporting). Both the community leaders and the health teams played supervisory roles during the implementation phase. The community leaders were responsible for ensuring that the CDDs adhere to treatment regulations and that community members comply with the exclusion criteria. The key indicators used for the evaluation of the CDI process included treatment coverage with Ivermectin, TB-DOTS treatment completion rate, percentage of households with at least one ITN, percentages of under five and pregnant mothers sleeping under ITN. Other indicators included vitamin A supplementation coverage, indicators of factors that facilitate or hinder the CDI process for integrated delivery of interventions of different complexity and cost and efficiency. Data analysis Quantitative data was entered onto computer using Epi-InfoTM vers. 3.5.1 and analysed using SPSS vers. 11. Standardized data entry formats were developed prior to the analysis phase. Simple descriptive statistics and graphic illustrations were used in presenting the key demographic characteristics of the study subjects. Results Coverage of Ivermectin treatment and Vitamin A supplementation Ivermectin coverage ranged from 77% to 91% with an average of 85% for all the five districts during the evaluation phase (85 ± 5.049 SD). Percentage coverage of Ivermectin treatment in the CDI districts was significantly higher (88%) than in the control (77%) (P< 0.05). The proportion of children aged 6 to 59 months who received Vitamin A supplementation during the last treatment round was 84% (ranged= 79%-92%) and during the evaluation phase was 84%±7.00. There was very little impact of CDI process for Vitamin A supplementation coverage and the difference between the CDI districts (84%) and comparison district (78.9%) (P = 0.188) was not significant (Figure 1). Tuberculosis - cases detection and treatment completion rates Korogwe and Lushoto were the intervention districts for TB DOTS, during the first and second year, respectively. The total number of TB patients in the study communities was found to be relatively low. Moreover, it was only in Korogwe district where 4 out of 7 patients had completed their treatment during the study period. This was due to the long TB-DOT treatment period. A small number of TB cases were detected in the rest of the districts [Muheza (6), Kilosa (6), Ulanga (3) and Lushoto (3)] where there treatment completion rate was not detected (Table 2). Utilisation of insecticide treated nets In Kilosa and Muheza, 72% and 60% of the households had at least one treated net, respectively. Households with at least an ITN in Ulanga accounted for 57% of the study population. The percentage of households with ITNs in the non CDI districts were 46% and 52% for Lushoto and Korogwe compared with the control (57%), the difference were not statistically significant (P > 0.05). There was no significant difference (P> 0.05) in the mean proportion of households with at least an ITN between CDI and control districts (Figure 2). The effectiveness of the CDI process was evaluated based on the proportion of pregnant women and under five children sleeping under ITNs between districts where nets were delivered through CDI process; non CDI districts and control district. The percentage of children under five years old sleeping under ITNs nets were significantly higher (P = 0.002) in CDI districts of Kilosa (76%) and Muheza (75%) than in the control district of Ulanga (48%) (Figure 3). Malaria home management The proportion of children under five years who were presumptively diagnosed with malaria and subsequently received appropriate treatment within 24 hours of malaria onset in CDI districts was higher than in the control district (P<0.05). Lushoto had highest score (79%), followed by Korogwe (75%). The proportion was the lowest in Ulanga, the control district (20%). Kilosa and Muheza districts, where the home malaria management intervention was delivered in the traditional way, scored 44% and 43%, respectively (Figure 4). This shows a significant difference in the parameter between CDI districts and control district (P = 0.002). The proportion of <5 years children with malaria who were referred to the health facility/personnel in the intervention districts did not differ from the control district (P>0.05). Lushoto, the district where home management of malaria was delivered through the CDI approach had the highest score (100%) followed by Korogwe (95%). Conversely, the proportion of caretakers/mothers who were able to recognize at least two signs of malaria for prompt treatment was significantly higher (P=0.024) in the control district of Ulanga (69%) than in the CDI districts of Lushoto (43%) and Korogwe (53%). Similarly, with the exception of hot body, the control district scored higher in terms of aggregated knowledge of all malaria symptoms for prompt treatment seeking as compared to all intervention districts combined (Figure 5). Supply and programme costs Overall supply costs had less variation in both control and intervention districts because most of the supplies such as the Ivermectin and Vitamin A were freely supplied by the government, through the Council Health Management Team. Supplies in Tanga region were lower than those for Morogoro region. Muheza had the lowest mean supply costs because overall the district reported less ITN distribution. Meanwhile, Kilosa district had the highest mean supply costs followed by the control district of Ulanga. Ulanga was the control district whereas the remaining districts were the intervention districts. The supply cost included only transport charges for drugs (Ivermectin, Artemether lumefantrine), Tuberculosis drugs and Vitamin A), bed nets and re-treatment kits. The mean programme costs were much higher in the control district of Ulanga (US$ 16382.9 ± 4143.8) than all other intervention districts (USD 13405.3 ± 6353.6). Lushoto had the second highest median score cost (US$ 18107.1 ± 5641.7) followed by Korogwe (US$ 1464.8 ± 4986.7) and Muheza (US$ 12373.9 ± 4624.9) districts whereas Kilosa (US$ 8536.5 ± 8448.9) had the lowest mean programme costs for the CDI interventions (Figure 6). The disease programmes involved in the costing included malaria, Tuberculosis, Vitamin A and Onchocerciasis. The total cost per programme includes salaries and allowances for the programme employees, recurrent training and social mobilization costs. Other costs included equipment (vehicles and maintenance charges) as well as supervision and monitoring costs. Discussion The present study investigated the extent to which the community-directed treatment with Ivermectin strategy could be adopted for the delivery of other interventions including malaria home management, TB cases detection and treatment completion rates, coverage of vitamin A supplement and insecticide treated nets. The results clearly showed that CDI is an effective intervention process. The treatment coverage in the CDI districts was in most cases significantly higher than in the control district. However, there was very little difference between control and intervention districts in terms of coverage of Vitamin A supplementation. This is likely to be attributed to the fact that vitamin A supplementation is through the national immunization day (NID) campaign which is carried out in all the districts simultaneously. The use of ITN has been one of the mainstays of malaria prevention in Tanzania. The emphasis has been put on the widespread use of insecticide-treated nets. The target was to have 60% coverage of ITNs among the vulnerable groups (young children and pregnant women) by 2005 (Magesa et al., 2005). Recent studies have estimated even a much lower overall mean ITN coverage in Tanzania. In a study in 2006, 36% of households in Tanzania were having at least one ITN; with only 23% and 26% of pregnant women and children under five having used an ITN, the previous night (Hanson et al., 2007). In a most recent study, on average, 62.7% and 28.8% of the households in Tanzania were found to own at least one mosquito net (any type) and insecticide treated net, respectively (Mboera et al., 2008). Tanzania expects that ITN coverage of under fives in 2009, after the Under Five Catch-up Campaign is complete, to be at least 80% (Mboera et al., 2008). If this is to be achieved, there is a need for concerted effort in scaling up the distribution nets throughout the country. Our results indicate that CDI districts had a higher coverage than the control district further indicating good effectiveness of the CDI process, which could be deployed to scale up ITN coverage throughout the country. The CDI approach showed little impact for home management of malaria in terms of providing instructions to care takers for proper management of sick children. The proportion was significantly higher in the control district than the CDI districts. The reason for higher proportion observed in the control district was most likely to have been attributed to the influence of a number of ITN projects in Ulanga district. Although no antimalarial drugs were made available to communities in both intervention and control districts, the mothers/guardians in the CDI districts were more likely to refer their children to health facilities than those in the control district. In conclusion, the study has clearly and evidently shown that integrated community directed intervention approach is a cost effective method of delivering health interventions at community level without necessarily increasing the cost. Acknowledgements The authors wish to acknowledge the contributions and support from Dr. Grace Saguti (National Onchocerciasis Control Programme), Mr. Francis Modaha (Tanzania Food and Nutrition Centre), Dr. Fred Lwilla (National Tuberculosis and Leprosy Programme), and Dr. Renata Mandike and Ms. Suzan Omari (National Malaria Control Programme). We also wish to thank the respective District Medical Officers their invaluable support. We would also like to register our appreciation to the community members and leaders for their enthusiasm and readiness to take an active role in the study. We are also grateful to Mrs. Rose Nguruwe (Kilosa), Mr. Abdul Dafa (Lushoto) and Mr. James Mgaya (Muheza) for their instrumental role as district focal persons. The Director, Amani Medical Research Centre is thanked for logistic support. This study was funded through APOC, the Bill and Melinda Gates Foundation, UNICEF/UNDP/World Bank/WHO Special Programme for Research and Training in Tropical Diseases (TDR). References
© Copyright 2008 - Health User's Trust Fund (HRUTF) The following images related to this document are available:Photo images[th08036f2.jpg] [th08036f5.jpg] [th08036f3.jpg] [th08036f1.jpg] [th08036f6.jpg] [th08036t2.jpg] [th08036f4.jpg] [th08036t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}