 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Tanzania Journal of Health Research, Vol. 10, No. 4, Oct, 2008, pp. 246-252 Modes of delivery assistance in Bangladesh M. Rahman*, T.I.Tarafder and G. Mostofa Department of Population Science and Human Resource Development, University of Rajshahi,
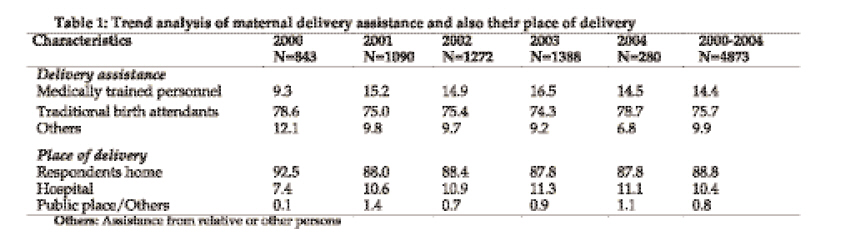
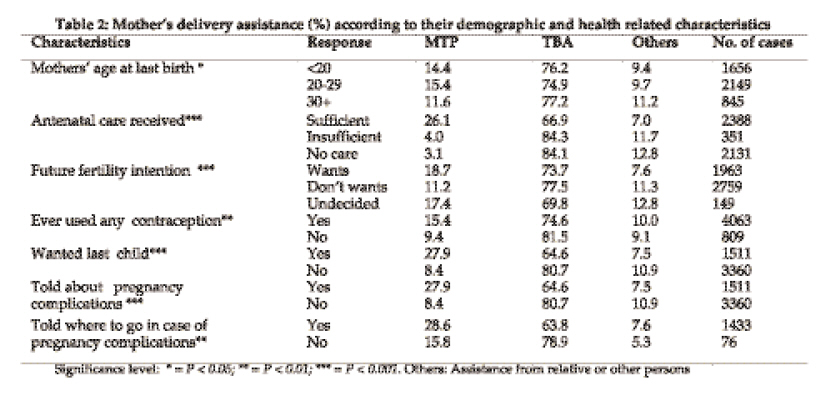
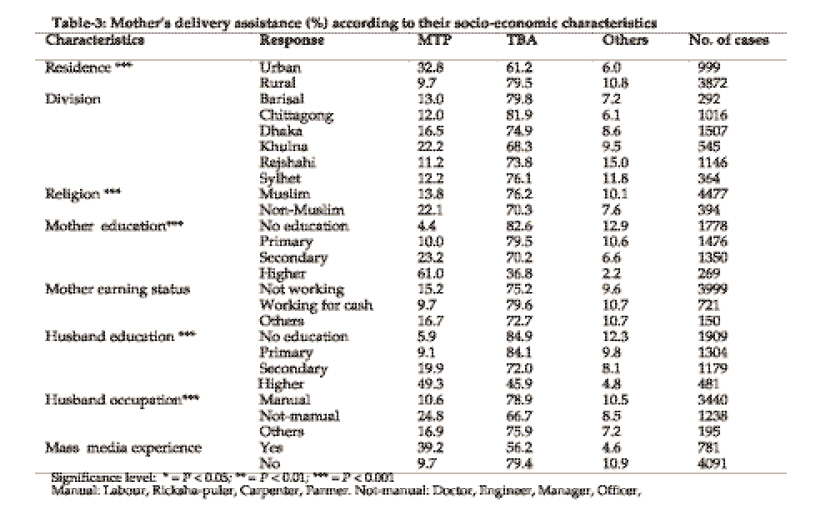
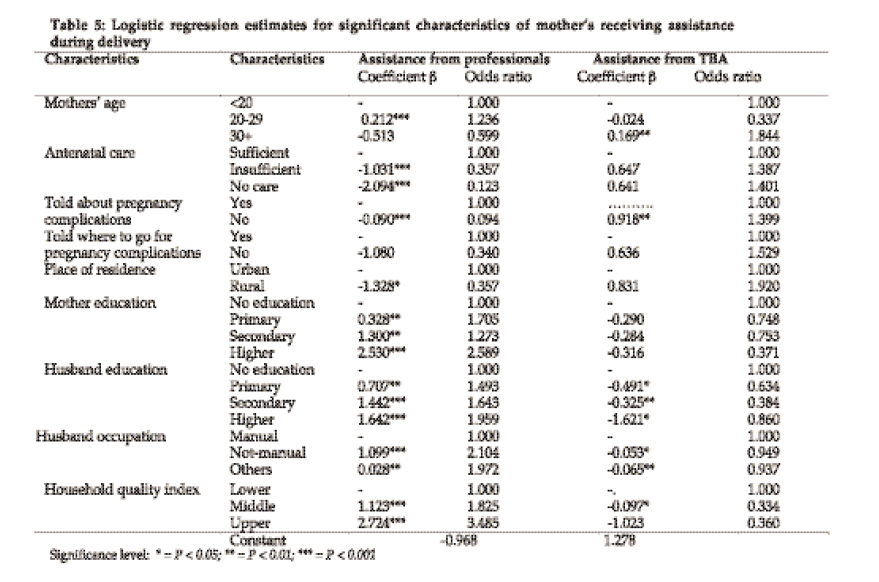
Rajshahi-6205, Bangladesh Received 28 April 2008 Revised 9 September 2008 Accepted 10 September 2008 Code Number: th08038 Abstract In Bangladesh, like many other developing countries among the major underlying factors leading to poor maternal situation include very low percentages of women actually seek professional medical assistance for pregnancy related care, deliveries and complications. This paper employs statistical methods to identify the factors associated with modes of delivery assistance in Bangladesh. To reach our goal Bangladesh Demographic and Health Survey of 2004 data for last five years (N = 4873) was used. Descriptive and multivariate logistic regression methods were employed in analyzing the data. It was observed that almost all the deliveries (88.8 %) took place at the homes of the women and most of them (85.6 %) were assisted by untrained traditional birth attendants, relatives or neighbours in unsafe and unhygienic conditions. Only 14.4% of the deliveries were assisted by the medically trained persons such as registered physicians, nurses or paramedics. The rate of receiving assistance from medically trained personnel was lower among mothers utilizing insufficient antenatal health care services. Middle aged women received delivery assistance more from medically trained personnel than the adolescents and women with higher age group. Multivariate logistic regression analysis shows that higher educated women were two-and-a-half times more likely to receive assistance from medically trained personnel than women with no education. Women whose husbands had a lower status job were less likely to have safe delivery practices. The main contributing factors likely to affect delivery practices were mass media exposure, husband’s occupation, education, antenatal care received, type of toilet facilities and household quality index. The results indicate several policy options. The high-risk group such as adolescents and higher aged women need special care and the existing health management system may be strengthened to create awareness among mothers of these groups for seeking appropriate measures from the beginning of pregnancy. There is need to ensure the availability of maternal health care centres for providing antenatal care and expand and improve the quality of normal delivery at home by trained providers and introduce post-partum visits. It is equally important that education for women is emphasised to bring about a lasting impact on the overall health condition of women. Key words: Antenatal care, home, delivery, Traditional birth attendant, Bangladesh Introduction Assistance during delivery is an important factor for delivery care in reducing health risks for both mothers and child. Proper health facilities and adequate medical supervision along with safe, hygienic conditions during delivery can reduce significantly the risk of infections and delivery related complications that may lead to maternal or neonatal morbidity and/or mortality. In Bangladesh, the current level of maternal mortality is very high, even by the standard of other developing countries. One of the main causes is the fact that most mothers go to unqualified persons during delivery (Mitra et al., 1994). Bangladesh is a developing country and maternity hospitals are quite inadequate. Most of the pregnant mothers are mainly accustomed to deliver births traditionally taking help from traditional qualified or unqualified birth attendant (TBA) or their relatives or neighbours. Recent statistics indicate that only 12% of births are attended by trained medical professional and overall three-fourths of births are attended by TBA (BMHS/MSS, 2001). The high perinatal mortality and maternal mortality in Bangladesh may be attributed to the low prevalence of delivery care and assistance. Delivery at home remains almost universal in Bangladesh. More than 90% of births are delivered at home often under unsafe and unhygienic conditions. Sixty-four percent of births are assisted by TBAs (10% being trained and 54% by untrained) (HSDP/MHR, 2003). Use of health facilities for delivery is more common in urban areas (22% of births) (BMHS/MSS, 2001). The latest national data shows maternal mortality ratio (MMR) to be around 300 per 100,000 live births (BMHS/MMS-2001) due to the lack of proper care or assistance. However, the estimates of the World Bank (2001) indicate that MMR is 440 per 100,000 live births. It is also estimated that the lifetime risk of dying from pregnancy and childbirth related causes in Bangladesh is 1 woman in 21, which compares to 1 woman in over 4,000 in industrialized countries (UNFPA, 2002). While the MMR tends to be considerably higher in low-income countries, there are some examples of other regional low-income countries such as Sri Lanka which has shown the ability to greatly reduce MMR to 80 per 100,000 live births (UNICEF, 1999). The choice of delivery places was also found to be affected by family size. Mothers with smaller family were more likely to be attended by a physician at their delivery places compared to mothers with large families (Kim & Oh, 1985). In this study we investigated the characteristics and trend of women of receiving delivery assistance over the last five years preceding the survey and identified factors that influenced the seeking delivery assistance in Bangladesh. Findings from this study are envisaged to provide important guidelines to improve the situation concerning the risk of delivery assistance in Bangladesh. Materials and Methods This study utilizes the data extracted from 2004 Bangladesh Demographic and Health Survey (BDHS), which were conducted under the authority of the National Institute of Population Research and Training of the Ministry of Health and Family Welfare in Bangladesh. The study considered only the case for their last child. In order to fulfil our objectives the respondents who took delivery assistance during the different years were classified into five groups as 2000, 2001, 2002, 2003 and 2004. Bivariate analysis was performed to determine the differentials of modes of delivery assistance by explanatory variables. Pearson’s Chi-square test of independence was performed to test the existence of significant association between categories of delivery assistance and selected risk factors. Considering the fact that among multivariate techniques the Cox’s linear logistic regression model is algebraically simple, computationally straightforward and efficient with acceptable degree of precision for a binary dependent variable, this study applied Cox’s linear logistic regression model (Cox, 1970) for multivariate analysis. Results Trend of delivery assistance and place of delivery A large proportion of delivery assistance was obtained from traditional birth attendants (TBA) than from qualified health professionals (Table 1). Delivery care from medically trained persons (MTP) such as doctors or nurses gradually increased from 2000 to 2003 but declined in 2004. It was also found that delivery assistance from other persons has decreased in 2004 than the previous time. The majority of the women gave birth at their home. There was an increasing trend for receiving delivery assistance from Government and private hospitals from 2000 to 2004. Differentials in receiving delivery assistance Mothers receiving sufficient antenatal care, intention of future fertility, using contraceptive methods, wanted last child and knowledge about pregnancy complications found to have strong positive relationship with types of delivery assistance (Table 2). Middle aged mothers (20-29 years) received delivery assistance more from medically trained personnel (such as doctor/nurse) but higher proportion of mothers belonging to the age ≥30 years received assistance from TBA. Sufficient care was described and the number of those who received at least three antenatal care (ANC) visits with the first visit during the first three months of pregnancy. On the other hand, insufficient care referred to number of those who received ANC from other persons. Mothers who had taken sufficient antenatal care were taking assistance more from medically trained personnel than from other conjugal parts. Mothers who ever used any contraceptive methods and mother who wanted their last child were taking delivery assistance more from medically trained personnel than from TBA. About 27.9% mothers who gave positive response for their pregnancy complications sought assistance from medically trained persons. This rate is higher than who were not able to describe their pregnancy problems. A similar situation was observed for those mothers who knew where they could get proper healthcare services for pregnancy complications (Table 2). In urban areas, health facilities were much better and available than in rural areas. A higher proportion (61.2 %) of mothers went to TBA in urban areas for assistance during delivery, though this proportion was considerably lower than in rural areas (79.5 %) (Table 3). More mothers in urban areas (32.8%) were seeking assistance from medically trained personnel during delivery than in rural areas (9.7%) (Table 3). Rural mothers were using more assistance from TBA than urban mothers. More mothers in Khulna (22.2%) were getting assistance from medically trained personnel than in the other divisions. On the other hand, Chittagong division had the largest (81.9%) proportion of women receiving assistance from TBA. Muslim mothers sought less assistance from qualified medical personnel but more from TBA than non-Muslim mothers. Seeking assistance during delivery was positively related with mother’s and father’s education. Highly educated mothers and their husbands were taking delivery care more from medically trained persons than from TBA or others. Wives whose husbands were professional workers took more assistance from governmental health professionals. The opposite situation was observed when husbands were involved in manual or others activities. Mass media exposure also had a positive effect on assistance during delivery. It was also observed that mothers who were in the lower category of the household possession index, received more assistance from TBA and less assistance from medically trained person than the upper category. About one-fifth (20.3%) and 71.3% of mothers who were using modern toilet facilities sought assistance from medically trained persons and TBAs, respectively. Women who were using piped water for safe drinking purposes sought assistance more from medically qualified persons than mothers using water from other sources such as wells, rivers or lakes. Determinants of receiving assistance during delivery The fitted model considered the assistance during delivery as dependent variable and it was coded as 1 if the mothers received delivery assistance from medically trained providers. From logistic regression analysis it was observed that mothers in the 20-29 years age group were 1.2 times more likely to receive assistance during delivery from medically trained personnel than adolescent mothers (Table 5). However, mothers who were 30 years were 0.5 times less likely to receive assistance from medically trained personnel and 1.8 times more likely to receive delivery assistance from TBA. Mothers’ utilizing “insufficient” ANC services and mothers who did not receive care during their antenatal period reported respectively to be 0.35 and 0.12 times less to receive assistance during their delivery from medically trained personnel than those mothers who took sufficient ANC services. Mothers who had insufficient ANC and no care were 1.3 and 1.4 times more likely to receive assistance from TBA than those who took sufficient prenatal care, respectively. Parental education showed a strong positive association with receiving delivery assistance from governmental health facilities. Mothers with higher, secondary and primary education were respectively 2.5 times, 1.2 times, and 1.7 times more likely to receive delivery care from government trained medically personnel as against mothers having no education (Table 5). Husband education also appeared as a strong predictor for delivery assistant from well qualified persons. Mothers whose husbands had higher, secondary and primary education had respectively 1.9, 1.6 and 1.4 times more likely to receive delivery assistance from medically trained personnel than those who had no formal education. Mothers, whose husbands were not manual worker, were 2.1 times more likely to take assistance from medically trained personnel than those who were manual workers. Mass media exposure also showed significant effect on utilization of government health care facilities at the time of delivery. Mothers having no mass media exposure were 0.8 times likely to receive less assistance from medically trained personnel than those who had mass media exposure. Mothers who were using well water and from other sources were respectively 0.6 and 0.8 times less likely to have delivery assistance from medically trained personnel than mothers who were using piped water for safe drinking purposes. Mothers who were using modern toilet facilities reported to be 2.5 times more likely to receive assistance during delivery from government-trained personnel than mothers having had no toilet facilities. Discussion This study was designed to make a comparative scenario of maternal delivery care in the Bangladesh situation. The rise and fall of delivery assistance observed in this study is likely to be due to the fact that the BDHS data was collected in May 2004 and it was not possible to collect total yearly information. However, the increasing trend for receiving delivery assistance from Government and private hospitals over the years was probably due to an increase in number of health centres in recent years. The observation that old-aged mothers received delivery assistance less from medically trained personnel is probably due to the fact that they had no proper knowledge about safe delivery and generally follow the traditional patterns. Mothers who had taken sufficient antenatal care were taking assistance more from medically trained personnel comparative to other conjugal parts. This may be explained by the fact that conscious mothers are more sincere to take proper government health care during delivery as they take sufficient antenatal care. Findings from this study indicate that rural mothers were using more assistance from TBAs than their counterparts in urban areas. This is likely to be attributed to unavailability of healthcare facilities in rural areas and that TBAs (locally known as Dai-ma) are readily available to provide the services at the patient’s home at low cost. Usually, TBAs are from the same communities and they are readily accessible at the time of need and the women need not to face the difficulty of travelling to healthcare facilities or making appointments with medical professionals. Moreover, in Bangladesh, especially in rural areas, there is a problem of communication and transportation, which involves both, time and cost (Ahmed et al., 1998).On the other hand, though government health services are financially not so expensive, organizationally and physically they may not be ideal to fulfil the demand of the clients. The observation that Muslim mothers sought less assistance from qualified personnel but more from TBAs than non-Muslim mothers is most likely to be attributed to the religious beliefs. Muslims husbands do not give permission to their wives to go to doctors or outside their home (Safe Motherhood, 2001). The element of choice becomes more important in Bangladesh sociocultural climate where women are reluctant to be examined by a male physician or unfamiliar nurse in healthcare facilities. The health facilities in Bangladesh still lack sufficient number of female health personnel and there is an increasing demand that medical care for women be provided by women. For women who observe the traditional rules of modesty or Islamic Purdha, TBAs may appear to be a better alternative for them. Parental education shows strong positive association with receiving delivery assistance from governmental health facility. In this study husbands’ was a strong predictor for seeking delivery assistance from well qualified persons. Education and husband’s occupation was associated with a larger proportion of women seeking care from trained medical personnel. Well-educated persons know the harmful of taking assistance from TBA or other untrained persons. The professional workers are usually more educated and conscious about the health of their family members and thereby encourage and help their wives to seek assistance from health professionals. Mass media exposure also has positive effect on assistance during delivery. In recent years, a number of governmental and non-governmental organizations have enriched their maternal and child health related programmes on television, radio and newspapers which are likely to have increased the mother’s knowledge on safe motherhood. Household economic indices and hygienic conditions have implication in seeking care from healthcare facilities. It has been shown that hygienic conditions such as use of potable water and type of toilet facilities are positive indicators of maternal health care system (Goodburn et al., 1995). Interestingly, women who were using piped water for safe drinking purposes had taken assistance more from medically qualified persons than mothers using well water or from other sources such as rivers and lakes. In conclusion, the findings from this study suggest the need for creation of awareness regarding appropriate behaviours during pregnancy, delivery and the post-partum period, and generate demand for use of maternal health services about the benefits of safe delivery practices. Government should ensure availability of maternal health care centres for providing ante-natal care. Equally, important, there is a need to expand and improve the quality of post natal care. Likewise, the quality of normal delivery at home by trained providers should be improved through appropriate training and the introduction of post-partum visits. Selected non-medically trained providers, who provide outreach services to all women of reproductive age, should receive basic mid-wifely training. It is also desirable to conduct more research on the factors that are associated with mother’s receiving delivery assistance. References
© Copyright 2008 - Health User's Trust Fund (HRUTF) The following images related to this document are available:Photo images[th08038t1.jpg] [th08038t5.jpg] [th08038t2.jpg] [th08038t3.jpg] [th08038t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}