 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
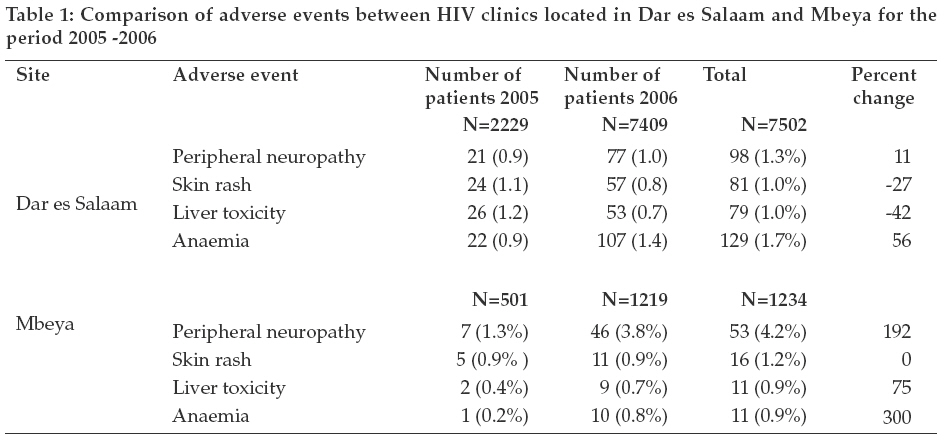
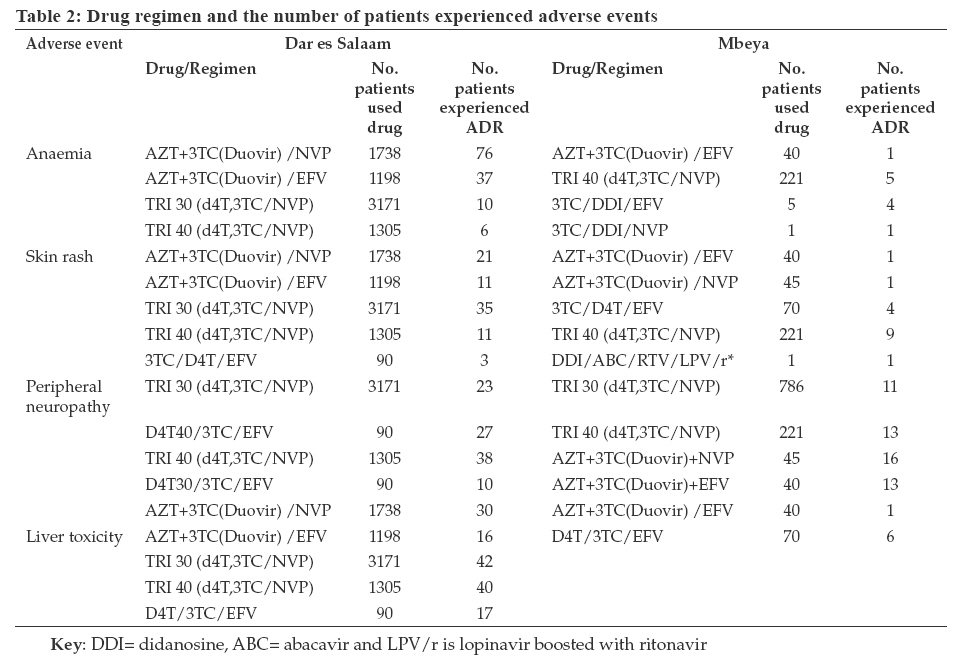
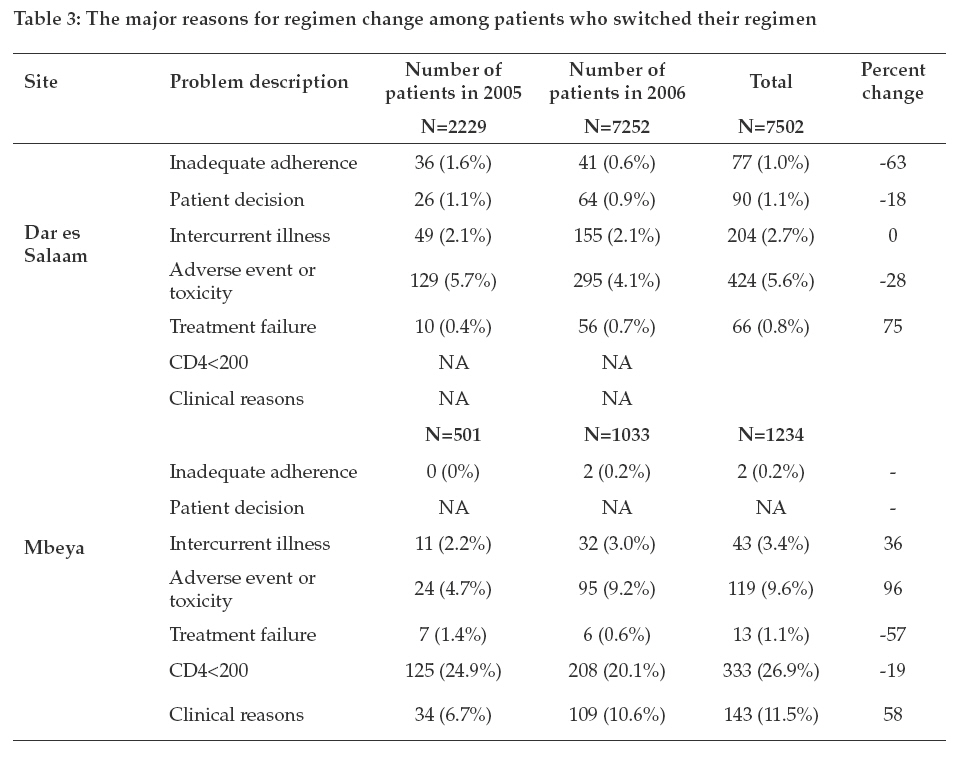
Tanzania Journal of Health Research, Vol. 11, No. 1, January, 2009, pp. 5-10 HIV patients presenting common adverse drug events caused by highly active antiretroviral therapy in Tanzania O.M.S. Minzi1*, H. Irunde2 and C. Moshiro3 1Muhimbili University of Health and Allied Sciences, School of Pharmacy, P.O. Box 6i01i, Dar es Salaam, Tanzania Received: 2 October 2008 Revised 16 November 2008 Accepted 17 November 2008 Code Number: th09002 Abstract Antiretroviral (ARV) drug toxicities pose treatment challenges and contribute to poor adherence. This study was carried out to document the commonly reported adverse reactions caused by ARV drugs in HIV patients in Tanzania. Information on drug induced adverse reactions (ADRs) in patients using ARV drugs was collected from the databases maintained in HIV clinics of Dar es Salaam and Mbeya. A total of 7502 and 1234 records of patients under ARV therapy by December 2006 were analysed in Dar es Salaam and Mbeya, respectively. In May, 2008 a cross-sectional study was conducted in which, the association between nevirapine (NVP) plasma concentrations and skin rashes problems was determined in 50 patients put on NVP based HAART for less than 2 weeks. Determination of NVP plasma concentration was carried out using a validated HPLC method in which patients from Dar es Salaam were involved. The study revealed that, anaemia, liver toxicity, skin rash and peripheral neuropathy were the most reported ADRs. The NVP plasma level determination revealed that there was no difference between those who had experienced skin rashes and those who did not (mean of 6.05 and 5.5μg/ml respectively). There was a slight increase in reported ADRs between 2005 and 2006. A total of 932 (12.4%) patients changed their regimen in Dar es Salaam between January 2005 and December, 2006. Similarly, a total of 542 (44%) patients in Mbeya changed their regimen during that period. It can be concluded that, in both Dar es Salaam and Mbeya patients developed ARV related ADRs which are similar to those reported elsewhere. Key words: HIV/AIDS, adverse reactions, antiretroviral drugs, Tanzania Introduction The introduction of antiretroviral therapy (ART) has revitalized communities and transformed perception of HIV/AIDS from a plague to a manageable, chronic illness (NACP, 2005). ARVs have dramatically reduced rates of mortality and morbidity as well as improved the quality of life for people living with HIV/AIDS. According to the current national guidelines, unless contraindicated, all eligible AIDS patients in Tanzania are put on Stavudine + Lamivudine + nevirapine (d4T/3TC/NVP) combination. However patients can be started on Zidovudine (AZT) based ART -AZT/3TC/NVP if there is peripheral neuropathy, d4T/3TC/EFV if there is tuberculosis (TB) and anaemia <7.5 gm/dl and AZT/3TC/EFV if there is TB and no anaemia (Vitezica et al., 2008). Despite ARVs being of much help to the health of most HIV/AIDS patients, the issues of drug induced toxicities has remained of great concern. ARVs belonging to a non-nucleoside reverse transcriptase inhibitors (NNRTIs) class have been reported to be associated with rash and hepatoxicity (Knobel et al., 2008; Caron et al., 2008). So far, nucleoside reverse transcriptase inhibitors (NRTIs) are being implicated to be causative of lactic acidosis probably due to mitochondria damage (Cherry et al., 2006). NRTIs have also been implicated to cause hypersensitivity reactions, neuropathies, pancreatitis, anaemia and neutropenia (Taha et al., 2004; Vigouroux et al., 1999). Protease inhibitors have been found to be associated with hyperlipidemia, hyperglycaemia, gastrointestinal symptoms, body-fat distribution abnormalities and insulin resistance (Vigouroux et al., 1999; Barbaro 2006; Nuesch et al., 2006). Drug interactions are one of the major problems in these multi-drug regimens and such interactions can lead to increased toxicities (Barry et al., 1999). As ART programmes continue to expand, a larger population will be subjected to ARVs. The Tanzania Food and Drugs Authority have registered more than 50 antiretroviral drug products for use in the country (TFDA, 2006). Variability in drug metabolic capacity among various populations predicts variations in the gene expression of the metabolising enzymes which could be influenced by geographical/ interracial differences (Bertilsson, 1995; Pfister et al., 2003). Even within the same geographical locations, variability among individuals with respect to various metabolising isoenzymes exists (Bertilsson, 1995; Pfister et al., 2003; Stahle et al., 2004). Therefore, data derived from within the country may have greater relevance and form basis for a decision-making and for effective patient management. This study was undertaken so as to find out if there were ADRs other than those reported in patients using ARV drugs in other countries. Materials and Methods Study design and sites This was a retrospective study involving 15 HIV clinics in Dar es Salaam and eight clinics in Mbeya in Tanzania. Among these facilities were public and private hospitals accredited to provide ART by the National AIDS Control Programme (NACP). These facilities receive free ARV access from the government and are also supported by various international nongovernmental organisations supported by the President’s Emergency Plan for AIDS Relief (PEPFAR) funding mechanism. Data collection Data were collected from records of patients who were on ARVs from January 2005 to December 2006. A total of 8736 ARV patient records were analysed out of which 7502 were from HIV clinics located in Dar es Salaam and 1234 from Mbeya. The data collection tool captured the name of the individual ARV drug or a combination thereof a given patient used, the date of initiation, the date the adverse reactions (ADRs) were reported, the type of ADRs reported and whether the treatment regimen was changed and the reason for changing. Documentation of clinical investigations for ADRs performed at the HIV clinics was done through record review. Blood level analysis In May 2008 we conducted a cross-sectional study in two HIV clinics of Dar es Salaam in which, the association between nevirapine plasma concentrations and skin rashes problems was determined in 50 patients put on NVP for less than 2 weeks. In this study, nevirapine plasma concentrations were determined in 20 patients who developed skin rashes and 30 patients who did not. From each patient 4 ml venous blood was collected just before the next scheduled ARV drug in the intake. The patients were requested to come back for blood samples collection in the morning. The blood was collected in EDTA tubes and the samples were immediately centrifuged. The obtained plasma samples were kept at -20ºC until assay. Nevirapine plasma concentrations were determined using an HPLC method developed in our laboratory. Briefly, the method involves extraction of nevirapine and the internal standard in basified di-isopropyl ether followed by shaking and centrifugation. The organic layer is then transferred into other tubes and dried with a current of air followed by reconstitution with 120μl mobile phase. Into the chromatograph, 90μl of the resulting solution is then injected and peak areas ratios between analyte and internal standard are recorded (O. Minzi et al. unpubl.). Data analysis ARV drug combinations were analysed with respect to the adverse reactions they caused in patients. Data analysis was done using EPI-INFO version 6.0 software. Nevirapine plasma concentrations were compared between the group which developed skin rashes and the one which did not experience such a reaction. Ethical considerations The study received ethical clearance by the Medical Research Coordination Committee of the National Institute for Medical Research through a letter with reference number NIMR/ HQ/R.8a/Vol.IX/612. Permission to access the patient records was sought from medical incharges of all study facilities. Results Frequency of adverse reactions A total of 2229 and 501 patients were on ART in 2005 in Dar es Salaam and Mbeya respectively and by the end of 2006, the number of patients had increased to 7502 and 1234 in these regions respectively (Table 1). There was an increase in the proportion of patients who experienced adverse reactions in 2006 as compared to 2005. Peripheral neuropathy and anaemia were reported to significantly rise in 2006 as compared to 2005. There was a 56% increase on the number patients, from 22 (0.9%) patients in 2005 to 107 (1.4%) patients in HIV clinics in Dar es Salaam in 2006. A similar trend was observed with peripheral neuropathy which increased from 21 (0.9%) cases in 2005 to 77 (1.0%) in 2006 in the same facilities. In Mbeya, there was almost a three-fold increase (from 1.3% in 2005 to 3.8% 2006) in the proportion of patients who experienced peripheral neuropathy. Similarly, a substantial increase in anaemia reported cases was noted. Patients who used a drug combination which contained nevirapine experienced more liver toxicity and skin rashes episodes than those who used EFV based combinations. More patients who used HAART combinations which contained 40mg stavudine experienced peripheral neuropathy than their counterparts that used 30mg stavudine (Table 2). By analysing the mean plasma concentrations obtained between the groups of patients who experienced nevirapine related rashes and those who did not experience any rashes, it was found that the mean drug concentrations was 6.05 and 5.5μg/ml respectively. Change of treatment regimen and reasons A total of 932 (12.4%) and 542 (44%) patients changed their initial ARV regimen in the HIV clinics due to various reasons (Table 3). Existence of severe adverse reactions was mentioned as one of the reasons in 5.6% and 9.6% of the patients in Dar es Salaam and Mbeya respectively. Discussion This study was conducted in order to document adverse reactions among patients who were on ARVs between January 2005 to December 2006 in HIV clinics of 2 regions highly hit by the pandemic and compare the nature of ADRs observed with those experienced in other countries. Most of ADRs observed in these facilities were in agreement with those previously reported elsewhere (Knobel et al., 2008; Caron et al., 2008; Taha et al., 2004; Vigouroux et al., 1999). Findings show that patients who used a drug combination which contained nevirapine experienced liver toxicity and skin rashes than those who used EFV based combinations. Nevirapine has been reported by other authors to be responsible for causing such conditions (Vitezica et al., 2008; Knobel et al., 2008). Anaemia cases were higher among patients who received AZT/ 3TC/NVP and least among patients who were treated with 3TC/D4T40/NVP and the figure went higher in 2006 in all facilities, confirming the involvement of AZT in bone marrow suppression and consequently anaemia. Similarly, peripheral neuropathy was significantly higher in 2006 than 2005 and was mainly observed among patients who were treated with stavudine based HAART particularly D4T40. Patient who used combination which contained 40mg stavudine experienced severe peripheral neuropathy than their counterparts who used 30mg Stavudine. Stavudine has been implicated to be the main cause of peripheral neuropathy in patients undergoing ART (Cherry et al., 2006). Recently, there have been recommendations to stop the use of D4T 40 mg in ART practices as it has no added therapeutic value over D4T 30 mg (Sánchez-Conde et al., 2005; McComsey et al., 2008). Stavudine induced toxicities are dose dependent and it is recommended to use the optimum dose which will be therapeutically adequate with minimum risk of causing toxicity (McComsey et al., 2008). As the present study shows, drug induced toxicities were among the major reasons of switching to 2nd line HAART. The common adverse reactions induced by ARV drugs in patents infected with HIV in Tanzania are similar to those reported in other countries. Data derived from within the country may have greater relevance and form a basis for decision-making and for effective patient management. Geographical and interracial differences in polymorphic drug oxidation with regard to cytochrome P450 enzymes have been reported before (Bertilsson, 1995). Even within the same geographical locations, variability among individuals with respect to various metabolising isoenzymes may exist and this in turn may influence treatment outcomes by some drugs (Barrett et al., 2002; Nolah et al., 2006; Marzolini et al., 2001; Manfred et al., 2005; Nunez et al., 2001). This means different individuals who are genetically different will have variable drug exposure and consequently will experience variable drug ADRs. For instance, a lower clearance and higher plasma levels of EFV in African-American compared to European-American has been reported suggesting higher likelihood of observing EFV induced ADRs in former than in the later (Barrett et al. 2002; Nolah et al., 2006; Marzolini et al., 2001; Manfred et al., 2005; Nunez et al., 2001). In a cross-sectional study in which, an attempt was made to determine if there was an association between nevirapine plasma concentrations and skin rashes problems, it was observed that the mean nevirapine plasma concentrations were 6.05 and 5.5μg/ml respectively, in patients who developed rashes and those who did not. These mean values had no relevant therapeutic difference as the steady plasma concentration of NVP ranges between 48 μg/ml in which all the obtained mean values lie (Nellen et al., 2008). Unfortunately, all databases had recorded ARV drugs in generic names, making it impossible to associate a specific ARV brand or product with a certain adverse event. Another limitation was lack of evidence on a particular ARV in a triple combination that caused ADR since the 3 drugs are taken at once by a patient. The reported ADRs were based on the knowledge of the clinician on ADRs for specific individual drug documented in the literature and therefore could make a prediction of the drug responsible for an ADR in a combination. This means that any adverse event not mentioned in the current literature could not be missed. Proper documentation of the drug safety data and continuous monitoring on ADRs of drugs is needed in individual countries which in turn could generate country specific data which is a cornerstone in optimisation good treatment outcomes In conclusion, this study has managed to identify the most commonly reported ARV inducedadversereactionsinTanzania. Thestudy has further confirmed that the adverse reactions experienced by HIV infected patients in Tanzania are not unique but similar to those commonly reported elsewhere. The information obtained in this study is useful in optimisation of treatment in HIV patients as well as improvement of HIV treatment guidelines in the country. Acknowledgements This study was funded by Tanzania Food and Drugs Authority on behalf of the Ministry of Health and Social Welfare which is highly acknowledged. We thank Mary Masanja and Moses Nandonde for their commitment to data collection.WealsothankthePermanentSecretary of the Ministry of Heath and Social Welfare for permitting us to conduct the study. This activity would not have been possible without the support from medical officers’ in-charge of the study sites. We also thank all patients who agreed to participate in the nevirapine plasma level determination study. References
© Copyright 2009 - Health User's Trust Fund (HRUTF) The following images related to this document are available:Photo images[th09002t1.jpg] [th09002t3.jpg] [th09002t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}